Download as pdf or txt
You might also like
- Miracles From The Vault... More Than 90 Life Saving, Award Winning 'Underground Cures' (Health & Alternative Medicine) (Health Science Institute)Document6 pagesMiracles From The Vault... More Than 90 Life Saving, Award Winning 'Underground Cures' (Health & Alternative Medicine) (Health Science Institute)prakash0% (7)
- Answers-Review Exercise An Outbreak of Enteritis During: Pilgrimage To MeccaDocument9 pagesAnswers-Review Exercise An Outbreak of Enteritis During: Pilgrimage To Meccayudha agustriNo ratings yet
- Clinical Concept Map-7Document1 pageClinical Concept Map-7Brandi Offield100% (1)
- Speaker NotesDocument21 pagesSpeaker Noteschinnupepsi4allNo ratings yet
- Psoriasis: Common DermatosesDocument7 pagesPsoriasis: Common DermatoseslaluneNo ratings yet
- Diagnosis and Management of Psoriasis: Clinical ReviewDocument9 pagesDiagnosis and Management of Psoriasis: Clinical Reviewirvan halimNo ratings yet
- Psoriasis: PathophysiologyDocument23 pagesPsoriasis: PathophysiologyImran KhanNo ratings yet
- Faculty of Medicine: Kafr El-Sheikh UniversityDocument11 pagesFaculty of Medicine: Kafr El-Sheikh UniversityjayNo ratings yet
- Psoriasis Lecture Notes 2015Document17 pagesPsoriasis Lecture Notes 2015SaulNo ratings yet
- Psoriasis and It's Homoeopathic ManagementDocument3 pagesPsoriasis and It's Homoeopathic ManagementInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Physical Trauma (Koebner's Phenomenon) Is A Major Factor in Eliciting LesionsDocument12 pagesPhysical Trauma (Koebner's Phenomenon) Is A Major Factor in Eliciting LesionsNaomi AnastacioNo ratings yet
- Psoriasis: A Systematic Review of Autoimmune DisorderDocument8 pagesPsoriasis: A Systematic Review of Autoimmune DisorderInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Patogenie LILI CompletDocument8 pagesPatogenie LILI CompletDianaNo ratings yet
- Psoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsDocument21 pagesPsoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsMapsNo ratings yet
- How To Cure PsoriasisDocument7 pagesHow To Cure Psoriasispallavsharma1987No ratings yet
- Psoriasis Management in The Community: BY DR U.B.Buhari Gpwer FRCGP MHADocument50 pagesPsoriasis Management in The Community: BY DR U.B.Buhari Gpwer FRCGP MHAEng Abdikariim AbdillahiNo ratings yet
- Y3 Immunologic DsesDocument65 pagesY3 Immunologic DsesJess PeltraNo ratings yet
- Psoriasis: Psoriasis Type of PsoriasisDocument18 pagesPsoriasis: Psoriasis Type of PsoriasisDeepikaNo ratings yet
- Psoriasis - Epidemiology, Clinical Features, and Quality of Life (Ii18.Full)Document7 pagesPsoriasis - Epidemiology, Clinical Features, and Quality of Life (Ii18.Full)Shahab UddinNo ratings yet
- Psoriasis and Miracles With HomoeopathyDocument3 pagesPsoriasis and Miracles With HomoeopathyEditor IJTSRDNo ratings yet
- Dermatology D. Azr Lec2 Mon 18.10.2010: Papulosquamous DiseasesDocument9 pagesDermatology D. Azr Lec2 Mon 18.10.2010: Papulosquamous DiseasesMohamed Al-zichrawyNo ratings yet
- PsoriasisDocument61 pagesPsoriasisWilliam WongNo ratings yet
- A Brief Summary of Clinical Types of Psoriasis: Invited ReviewDocument4 pagesA Brief Summary of Clinical Types of Psoriasis: Invited ReviewRemigius RiyanNo ratings yet
- Psoriasis: Key PointsDocument11 pagesPsoriasis: Key Pointsazucena rocio de la roca gonzalezNo ratings yet
- 2545-Article Text-7661-1-10-20190414 PDFDocument6 pages2545-Article Text-7661-1-10-20190414 PDFClariza ZulyanNo ratings yet
- PatogenezDocument10 pagesPatogenezlloplNo ratings yet
- Psoriasis: A Comprehensive Review: Nternational Ournal OF Harmacy & IFE CiencesDocument21 pagesPsoriasis: A Comprehensive Review: Nternational Ournal OF Harmacy & IFE Ciences24hintheghettoworkoutNo ratings yet
- Bur FieldDocument6 pagesBur FieldNexi anessaNo ratings yet
- 170 FullDocument4 pages170 FullRegita LatuihamalloNo ratings yet
- Psoriasis - StatPearls - NCBI BookshelfDocument8 pagesPsoriasis - StatPearls - NCBI BookshelfMehmet TaşçıNo ratings yet
- 610-Article Text-3639-1-10-20220823Document7 pages610-Article Text-3639-1-10-20220823Gaema MiripNo ratings yet
- Psoriasis: Posted: 02 Aug 2010 11:18 PM PDTDocument5 pagesPsoriasis: Posted: 02 Aug 2010 11:18 PM PDTScamb TrekNo ratings yet
- PsoarisDocument10 pagesPsoarisNayaNo ratings yet
- Psoriasis Western and Ayurvedic Approaches To Treatment by Kim TamiettiDocument13 pagesPsoriasis Western and Ayurvedic Approaches To Treatment by Kim TamiettiEstudio LFANo ratings yet
- PSORIASISDocument27 pagesPSORIASISnurulzakinahnunu100% (1)
- Ayurvedic Management of Psoriasis (Ek Kustha) - A Case StudyDocument8 pagesAyurvedic Management of Psoriasis (Ek Kustha) - A Case Studybhavana NandakumarNo ratings yet
- Kuliah 4 B - PSORIASISDocument30 pagesKuliah 4 B - PSORIASISTimothy TobiasNo ratings yet
- Acute and Chronic Dermatosis ..Document28 pagesAcute and Chronic Dermatosis ..mohammed alrubaiaanNo ratings yet
- Psoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsDocument21 pagesPsoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsOktavianti Prisilia SoumokilNo ratings yet
- Psoriasis and Anesthetic ConsiderationsDocument10 pagesPsoriasis and Anesthetic ConsiderationsChantall Anaya MtzNo ratings yet
- Childhood PsioriasisDocument6 pagesChildhood PsioriasisYuliana DaisongNo ratings yet
- Referat Kulit KakayDocument26 pagesReferat Kulit KakayRezky Dwiputra FellanysNo ratings yet
- Askep Psoriasis: Bab I PendahuluanDocument64 pagesAskep Psoriasis: Bab I PendahuluanMoh Syukrin LamukeNo ratings yet
- Recent Insights Into The Immunopathogenesis of Psoriasis Provide New Therapeutic OpportunitiesDocument13 pagesRecent Insights Into The Immunopathogenesis of Psoriasis Provide New Therapeutic Opportunitiesraudhatul muttaqinNo ratings yet
- Psoriasis Pada Kehamilan JurnalDocument7 pagesPsoriasis Pada Kehamilan Jurnalaprila citra daraNo ratings yet
- Jurnal PsoriasisDocument6 pagesJurnal PsoriasisseptyneNo ratings yet
- Psoriasis Vulgaris DG KortikosteroidDocument7 pagesPsoriasis Vulgaris DG KortikosteroidNurmaniar MajidNo ratings yet
- PsoriasisDocument32 pagesPsoriasisChirag VijayvargiyaNo ratings yet
- White Scaly Papules and Plaques On His Elbows, Extensor Arms, Knees, and ShinsDocument54 pagesWhite Scaly Papules and Plaques On His Elbows, Extensor Arms, Knees, and ShinsJohn Christopher LucesNo ratings yet
- PSORIASISDocument1 pagePSORIASISbashirabubaker2No ratings yet
- Eritemul NodosDocument10 pagesEritemul NodosglasshandsNo ratings yet
- Griffiths2007 PDFDocument9 pagesGriffiths2007 PDFFirah Triple'sNo ratings yet
- Autoinflammatory Syndromes Associated With Hidradenitis Suppurativa and or AcneDocument8 pagesAutoinflammatory Syndromes Associated With Hidradenitis Suppurativa and or AcneFreddy RojasNo ratings yet
- Diagnosis Dan Penatalaksanaan Psoriasis Pada Orang Dewasa: Novella Ruana Fista Hamady 102014197 / C5Document19 pagesDiagnosis Dan Penatalaksanaan Psoriasis Pada Orang Dewasa: Novella Ruana Fista Hamady 102014197 / C5vellahamadyNo ratings yet
- Psoriasis: ClassificationDocument10 pagesPsoriasis: ClassificationRaluk OnytzaNo ratings yet
- A Clinico-Epidemiological Study On Palmoplantar DermatosesDocument8 pagesA Clinico-Epidemiological Study On Palmoplantar DermatosesIJAR JOURNALNo ratings yet
- E Poster - Dini DaniatyDocument1 pageE Poster - Dini DaniatyDini DaniatyNo ratings yet
- Psoriasis 1Document32 pagesPsoriasis 1SabaniaresmenNo ratings yet
- The Acutely Ill Patient With Fever and Rash Department of Microbiology Micro II-643 Infectious Diseases Victoria Michelen, MDDocument49 pagesThe Acutely Ill Patient With Fever and Rash Department of Microbiology Micro II-643 Infectious Diseases Victoria Michelen, MDFelito SifonteNo ratings yet
- Cellulitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCellulitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Activities of The Year 2023Document2 pagesActivities of The Year 2023Franz SalazarNo ratings yet
- Zombies Infection PDFDocument5 pagesZombies Infection PDFPatriciaNo ratings yet
- Jurnal RabiesDocument4 pagesJurnal RabiesDe'Uma Beiby SwettyNo ratings yet
- Mono 50Document425 pagesMono 50MellysaNo ratings yet
- Case Report 1676563639Document6 pagesCase Report 1676563639noah jemedafeNo ratings yet
- Chapter 14 MicrobioDocument14 pagesChapter 14 MicrobiobenbengNo ratings yet
- Trifold Corona VirusDocument2 pagesTrifold Corona VirusChelle BersaminNo ratings yet
- 01 14 2021 GERD Inflammatory Bowel Disease Irritable Bowel Syndrome ALLENDocument66 pages01 14 2021 GERD Inflammatory Bowel Disease Irritable Bowel Syndrome ALLENMikey ZhitnitskyNo ratings yet
- Research Paper On Dengue Fever in PakistanDocument6 pagesResearch Paper On Dengue Fever in Pakistangvzz4v44100% (1)
- Filedate - 381download Ebook Community Public Health Nursing Promoting The Health of Populations PDF Full Chapter PDFDocument67 pagesFiledate - 381download Ebook Community Public Health Nursing Promoting The Health of Populations PDF Full Chapter PDFnancy.larsen721100% (33)
- Weekly Epidemiological Report: A Publication of The Epidemiology Unit Ministry of Health, Nutrition & Indigenous MedicineDocument4 pagesWeekly Epidemiological Report: A Publication of The Epidemiology Unit Ministry of Health, Nutrition & Indigenous MedicineVijayakanth VijayakumarNo ratings yet
- Anaphylactic ShockDocument14 pagesAnaphylactic ShockAuliya AndiNo ratings yet
- Treating Canine Distemper VirusDocument23 pagesTreating Canine Distemper VirusJack HollandNo ratings yet
- Polyneuropathy: ClinicalDocument33 pagesPolyneuropathy: ClinicalIzabella MihályNo ratings yet
- A "Hit-And-Run" Affair - A Possible Link For Cancer Progression in VirallyDocument8 pagesA "Hit-And-Run" Affair - A Possible Link For Cancer Progression in Virally2211801733No ratings yet
- RLE NCMB 314-M2-CU 9 Respiratory ChangesDocument6 pagesRLE NCMB 314-M2-CU 9 Respiratory ChangesJordz PlaciNo ratings yet
- Courses InfoDocument3 pagesCourses InfoHAJARATHNo ratings yet
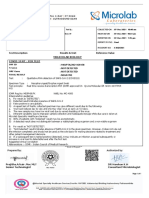
- Molecular Biology: Results & Unit Reference Value Test DescriptionDocument1 pageMolecular Biology: Results & Unit Reference Value Test DescriptionLibu GeorgebabuNo ratings yet
- Psychiatry 1Document4 pagesPsychiatry 1Axel JusufNo ratings yet
- Vetlexicon News Update - Jan 2020 US SizeDocument2 pagesVetlexicon News Update - Jan 2020 US SizeTheBoss 20No ratings yet
- BHF CVD Statistics Global FactsheetDocument12 pagesBHF CVD Statistics Global FactsheetRobby Paguh TariganNo ratings yet
- BSNURSE: NCP - HypertensionDocument3 pagesBSNURSE: NCP - Hypertensionmickey_beeNo ratings yet
- NYSED Health and Safety Guide For The 2021 2022 School YearDocument21 pagesNYSED Health and Safety Guide For The 2021 2022 School YearNewsChannel 9100% (2)
- CH 039 STG Rickettsial DiseaseDocument11 pagesCH 039 STG Rickettsial Diseasesuheena.CNo ratings yet
- Nhs Covid Pass - Vaccinated: Pfizer/Biontech Covid-19 Vaccine Pfizer/Biontech Covid-19 VaccineDocument1 pageNhs Covid Pass - Vaccinated: Pfizer/Biontech Covid-19 Vaccine Pfizer/Biontech Covid-19 VaccineAnca IroaiaNo ratings yet
- Tuberculosis: Mr. Vinod V. Bagilkar Lecturer Department of Pediatric NursingDocument57 pagesTuberculosis: Mr. Vinod V. Bagilkar Lecturer Department of Pediatric NursingSELEMAYE ZENEBENo ratings yet
- Crisis ManagementDocument13 pagesCrisis ManagementShamala ganesanNo ratings yet