Download as pdf or txt
You might also like
- What Next After 10th, Inter, DegreeDocument10 pagesWhat Next After 10th, Inter, DegreeBlue JaguarNo ratings yet
- A Broken Wave-Lionel EsherDocument39 pagesA Broken Wave-Lionel EsherChristian NoetzlyNo ratings yet
- Global Public Health: Click To Edit Master Title StyleDocument77 pagesGlobal Public Health: Click To Edit Master Title StyleDono WidiatmokoNo ratings yet
- A Machine-Learning Algorithm For Neonatal Seizure Recognition: A Multicentre, Randomised, Controlled TrialDocument10 pagesA Machine-Learning Algorithm For Neonatal Seizure Recognition: A Multicentre, Randomised, Controlled TrialAnonymous 1DK1jQgAGNo ratings yet
- Valerie 2018Document8 pagesValerie 2018Rannah AlmeidaNo ratings yet
- Pinchefsky 2019Document10 pagesPinchefsky 2019Devi Albaiti JannatiNo ratings yet
- Journal Medicine: The New EnglandDocument8 pagesJournal Medicine: The New EnglandHam jungNo ratings yet
- Nej M 200009073431001Document8 pagesNej M 200009073431001Asri Ani NurchasanahNo ratings yet
- Cross 2023 PediatricepilepsysurgeryDocument11 pagesCross 2023 PediatricepilepsysurgeryGala GonzalezNo ratings yet
- ExcluídoDocument4 pagesExcluídoVeronica GomesNo ratings yet
- Early Use of Antibiotics Is Associated With A Lower Incidence of Necrotizing EnterocolitisDocument9 pagesEarly Use of Antibiotics Is Associated With A Lower Incidence of Necrotizing EnterocolitisRestu TriwulandaniNo ratings yet
- 2020 Epigenetics - ExplainedDocument15 pages2020 Epigenetics - ExplainedDaniela GasnașNo ratings yet
- El-Khouly 2021Document9 pagesEl-Khouly 2021docadax848No ratings yet
- Abstract in Surgery PDFDocument188 pagesAbstract in Surgery PDFDrAmmar MagdyNo ratings yet
- Summary Proceedings From The Neurology Group On Neonatal SeizuresDocument7 pagesSummary Proceedings From The Neurology Group On Neonatal SeizuresTran Trang AnhNo ratings yet
- Seminars in Fetal & Neonatal Medicine: Chakrapani Vasudevan, Malcolm LeveneDocument7 pagesSeminars in Fetal & Neonatal Medicine: Chakrapani Vasudevan, Malcolm LeveneAngelica AponteNo ratings yet
- Australian GuidelinesDocument12 pagesAustralian GuidelinesMaria Agostina EspecheNo ratings yet
- Recommendations For Uniform Definitions Used in Newborn Screening For Severe Combined ImmunodeficiencyDocument9 pagesRecommendations For Uniform Definitions Used in Newborn Screening For Severe Combined ImmunodeficiencyZ. Raquel García OsornoNo ratings yet
- NPE Teaching Manual El-Khuffash 2019 - Dr. Ahmad Kautsar, Sp.ADocument117 pagesNPE Teaching Manual El-Khuffash 2019 - Dr. Ahmad Kautsar, Sp.AlaurentiaNo ratings yet
- Enterovirus and Parechovirus Meningitis in InfantsDocument6 pagesEnterovirus and Parechovirus Meningitis in InfantsCarlos Peña PaterninaNo ratings yet
- Hemodynamics and Cardiology 2019 PDFDocument594 pagesHemodynamics and Cardiology 2019 PDFStollery SandboxNo ratings yet
- Tomson2011 PDFDocument9 pagesTomson2011 PDFsujonosuputroNo ratings yet
- Availability of Active Therapeutic Hypothermia at Birth For Neonatal Hypoxic Ischaemic Encephalopathy A UK Population Study From 2011 To 2018Document13 pagesAvailability of Active Therapeutic Hypothermia at Birth For Neonatal Hypoxic Ischaemic Encephalopathy A UK Population Study From 2011 To 2018Eduardo Rios DuboisNo ratings yet
- ERCP-related Adverse Events: European Society of Gastrointestinal Endoscopy (ESGE) GuidelineDocument24 pagesERCP-related Adverse Events: European Society of Gastrointestinal Endoscopy (ESGE) GuidelineFarid RakhmanNo ratings yet
- PECARN Algorithms For Minor Head TraumaDocument11 pagesPECARN Algorithms For Minor Head Traumaedgarjavier65No ratings yet
- Ferric Carboxymaltose Versus Ferrous Fumarate in ADocument11 pagesFerric Carboxymaltose Versus Ferrous Fumarate in AEstifanos KassahunNo ratings yet
- 1 s2.0 S0720048X11003214 MainDocument5 pages1 s2.0 S0720048X11003214 MainHamza ArjahNo ratings yet
- JPM 13 01411 v2Document15 pagesJPM 13 01411 v2Luluil MunirohNo ratings yet
- MainDocument11 pagesMaintriska antonyNo ratings yet
- 2019 Two-Year Neurodevelopmental Outcomes After Mild Hypoxic IschemicDocument8 pages2019 Two-Year Neurodevelopmental Outcomes After Mild Hypoxic IschemicIan RodriguezNo ratings yet
- Deep LearningDocument6 pagesDeep Learningragou100% (1)
- Devries2009 Evolving Understanding ofDocument10 pagesDevries2009 Evolving Understanding ofModou NianeNo ratings yet
- Atención de Los Niños Con Alergias A FármacosDocument5 pagesAtención de Los Niños Con Alergias A FármacosHugo RoldanNo ratings yet
- Neonatal Seizures With Hypothermia - Laptook - SuggestedDocument8 pagesNeonatal Seizures With Hypothermia - Laptook - Suggestedseemee23820No ratings yet
- ProteccionCerebral - lea.ArchDisChildFetalNeonatalEd.2017Document7 pagesProteccionCerebral - lea.ArchDisChildFetalNeonatalEd.2017gfloreshNo ratings yet
- EEG Lab at KKH First Outside USDocument8 pagesEEG Lab at KKH First Outside USweberyehNo ratings yet
- 2021 Article 817Document10 pages2021 Article 817Muriel FialiwanNo ratings yet
- Grading Quality of Evidence About Diagnostic Tests and StrategiesDocument8 pagesGrading Quality of Evidence About Diagnostic Tests and StrategiesSalem RawashdahNo ratings yet
- Ped ProcalcitoninasepsisneoDocument11 pagesPed ProcalcitoninasepsisneoMirna Karime Gar CerNo ratings yet
- CV Updated 2022 Tse YapDocument4 pagesCV Updated 2022 Tse YapCharlotte YapNo ratings yet
- @MBmedicalbook 2019 .Document575 pages@MBmedicalbook 2019 .Hanif AbdullahNo ratings yet
- Bibliografia Risco 1Document16 pagesBibliografia Risco 1PridesoulNo ratings yet
- Beetween Vascular Endothelial Growth FactorDocument9 pagesBeetween Vascular Endothelial Growth FactorZakkiyatus ZainiyahNo ratings yet
- Remote and Longterm Selfmonitoring of Electroencephalographic and Noninvasive Measurable Variables at Home in Patients With Epilepsy EEGHOME Protocol For An Observational studyJMIR Research ProtocolsDocument12 pagesRemote and Longterm Selfmonitoring of Electroencephalographic and Noninvasive Measurable Variables at Home in Patients With Epilepsy EEGHOME Protocol For An Observational studyJMIR Research ProtocolsMiguel PalacioNo ratings yet
- Neonatal Infantile Finalapril5Document81 pagesNeonatal Infantile Finalapril5AlexandraChituNo ratings yet
- 10 1093@rheumatology@kez041Document10 pages10 1093@rheumatology@kez041afrilia.iNo ratings yet
- Safety and Efficacy of Independent Allied Healthcare Professionals in The Assessment and Management of Plagiocephaly PatientsDocument5 pagesSafety and Efficacy of Independent Allied Healthcare Professionals in The Assessment and Management of Plagiocephaly Patientsquajeutterugrau-6658No ratings yet
- Early Life Serum Neurofilament Dynamics Predict Neurodevelopmental Outcome of Preterm InfantsDocument8 pagesEarly Life Serum Neurofilament Dynamics Predict Neurodevelopmental Outcome of Preterm InfantsKatharina GoeralNo ratings yet
- 361 FullDocument7 pages361 FullnissashiblyNo ratings yet
- FilefullDocument5 pagesFilefullAinun NisahNo ratings yet
- Association Between Opioid Use During Mechanical Ventilation in - 2023 - EclinicDocument9 pagesAssociation Between Opioid Use During Mechanical Ventilation in - 2023 - Eclinicronaldquezada038No ratings yet
- HHS Public Access: Author ManuscriptDocument21 pagesHHS Public Access: Author Manuscripttq9prx5s5qNo ratings yet
- The 2022 Update of IUIS Phenotypical Classifcation For Human Inborn Errors of ImmunityDocument13 pagesThe 2022 Update of IUIS Phenotypical Classifcation For Human Inborn Errors of ImmunitygabrielNo ratings yet
- 2015 Article 10Document11 pages2015 Article 10dechastraNo ratings yet
- Phoenix StudyDocument10 pagesPhoenix StudyzaaaidaNo ratings yet
- Piis1474442208701418 PDFDocument8 pagesPiis1474442208701418 PDFsebastian quiroz floresNo ratings yet
- 10 1684@epd 2019 1105Document21 pages10 1684@epd 2019 1105michaelwillsonNo ratings yet
- Principles and Practice of Child Neurology in Infancy, 2nd EditionFrom EverandPrinciples and Practice of Child Neurology in Infancy, 2nd EditionNo ratings yet
- Realtime Continuous Glucose Monitoring in Preterm Infants REACTDocument9 pagesRealtime Continuous Glucose Monitoring in Preterm Infants REACTFray BotodNo ratings yet
- Psychosocial Care For Injured Children: Worldwide Survey Among Hospital Emergency Department StaffDocument13 pagesPsychosocial Care For Injured Children: Worldwide Survey Among Hospital Emergency Department StaffNilla Afiatni SamarkhanNo ratings yet
- Clinical Management of Seizures in Newborns: Diagnosis and TreatmentDocument10 pagesClinical Management of Seizures in Newborns: Diagnosis and TreatmentfitriNo ratings yet
- Assessing The Quality of The Management of Tonsillitis Among Australian Children: A Population-Based Sample SurveyDocument8 pagesAssessing The Quality of The Management of Tonsillitis Among Australian Children: A Population-Based Sample SurveyIntan Nur HijrinaNo ratings yet
- Intravenous Iron in Heart Failure and Chronic Kidney DiseaseDocument9 pagesIntravenous Iron in Heart Failure and Chronic Kidney DiseaseAris BayuNo ratings yet
- Daftar Harga Jualan OmaDocument1 pageDaftar Harga Jualan OmaAris BayuNo ratings yet
- 10 1001@jamapediatrics 2018 5056Document7 pages10 1001@jamapediatrics 2018 5056Aris BayuNo ratings yet
- KT/V or Bicarbonate: What Is More Important For Growth in Pediatric Peritoneal Dialysis Patients?Document7 pagesKT/V or Bicarbonate: What Is More Important For Growth in Pediatric Peritoneal Dialysis Patients?Aris BayuNo ratings yet
- Association of Screen Time With Parent - Reported Cognitive Delay in Preschool Children of Kerala, IndiaDocument8 pagesAssociation of Screen Time With Parent - Reported Cognitive Delay in Preschool Children of Kerala, IndiaAris BayuNo ratings yet
- The Association of Parent - IndDocument15 pagesThe Association of Parent - IndAris BayuNo ratings yet
- Ijph 66 630700Document7 pagesIjph 66 630700Aris BayuNo ratings yet
- Height-For-Age BOYS: 2 To 5 Years (Z-Scores)Document3 pagesHeight-For-Age BOYS: 2 To 5 Years (Z-Scores)Aris BayuNo ratings yet
- Stepwise Approach in Longterm Management of Asthma in ChildrenDocument41 pagesStepwise Approach in Longterm Management of Asthma in ChildrenAris BayuNo ratings yet
- Original Article: Virendra K. Pal, Ajai Agrawal, Suwarna Suman, V. B. PratapDocument4 pagesOriginal Article: Virendra K. Pal, Ajai Agrawal, Suwarna Suman, V. B. PratapAris BayuNo ratings yet
- Hipersensitivity 200111Document67 pagesHipersensitivity 200111Aris BayuNo ratings yet
- Laser in Situ Keratomileusis For Astigmatism 0.75 Diopter Combined With Low Myopia: A Retrospective Data AnalysisDocument9 pagesLaser in Situ Keratomileusis For Astigmatism 0.75 Diopter Combined With Low Myopia: A Retrospective Data AnalysisAris BayuNo ratings yet
- Neonatal Complications of Premature Rupture of Membranes: AbstractDocument5 pagesNeonatal Complications of Premature Rupture of Membranes: AbstractAris BayuNo ratings yet
- BlackBerry Smartphone Security Feature Overview 1907956 0302033105 001 7.1 USDocument16 pagesBlackBerry Smartphone Security Feature Overview 1907956 0302033105 001 7.1 USAris BayuNo ratings yet
- Physics Education Thesis TopicsDocument4 pagesPhysics Education Thesis TopicsPaperWriterServicesCanada100% (2)
- Effects of Handling On Animals Welfare During TranDocument54 pagesEffects of Handling On Animals Welfare During TranNikhilesh WaniNo ratings yet
- Anti-Virus Malware DNS Trap FeatureDocument2 pagesAnti-Virus Malware DNS Trap Featuredas zobNo ratings yet
- Vocabulary For TOEFL iBTDocument191 pagesVocabulary For TOEFL iBTJavzaaNo ratings yet
- FUJITSU Server PRIMERGY RX1330 M1 Rack Server: Data SheetDocument9 pagesFUJITSU Server PRIMERGY RX1330 M1 Rack Server: Data SheetSérgio MarquesNo ratings yet
- Bigmart Sales Solution MethodologyDocument5 pagesBigmart Sales Solution MethodologyArnab DeyNo ratings yet
- From Protista To DNADocument11 pagesFrom Protista To DNAtantalus11No ratings yet
- Iso 50005 - 2021Document51 pagesIso 50005 - 2021Lilia LiliaNo ratings yet
- Preterm Prelabor Rupture of Membranes - Clinical Manifestations and Diagnosis - UpToDateDocument26 pagesPreterm Prelabor Rupture of Membranes - Clinical Manifestations and Diagnosis - UpToDateCristinaCaprosNo ratings yet
- Cs607 Midterm Solved Mcqs by JunaidDocument49 pagesCs607 Midterm Solved Mcqs by JunaidZainab Tatheer100% (1)
- Murphybed dn1117Document17 pagesMurphybed dn1117mcvelli40100% (2)
- Sample Assignment 1-1Document20 pagesSample Assignment 1-1Nir IslamNo ratings yet
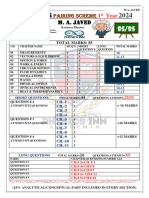
- Pairing Scheme 1st Year 2024 BY PHYSICS INN ACDEMIA M.A. JAVEDDocument1 pagePairing Scheme 1st Year 2024 BY PHYSICS INN ACDEMIA M.A. JAVEDabdull phyNo ratings yet
- BK Ambari InstallationDocument72 pagesBK Ambari InstallationFernovy GesnerNo ratings yet
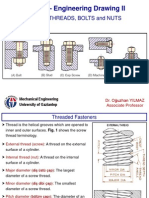
- SCREW THREADS, BOLTS and NUTS PDFDocument10 pagesSCREW THREADS, BOLTS and NUTS PDFhrhgk50% (2)
- Bhubneshwor LeadsDocument4 pagesBhubneshwor LeadsCo2 RenuUNo ratings yet
- OCEANSDocument4 pagesOCEANSamna hamidNo ratings yet
- Physics PDFDocument276 pagesPhysics PDFBenjamín Medina CarrilloNo ratings yet
- BELSummer Training ReportDocument33 pagesBELSummer Training ReportPalak MeenaNo ratings yet
- The Verb To BeDocument1 pageThe Verb To Bek.havleovaNo ratings yet
- Cobol 1.0Document43 pagesCobol 1.0sarathNo ratings yet
- Petrochemical Standards (PDFDrive)Document68 pagesPetrochemical Standards (PDFDrive)fatimahNo ratings yet
- Car Sticker Policy PDFDocument11 pagesCar Sticker Policy PDFMohsin KhanNo ratings yet
- Shreya Shukla Case Study-2Document41 pagesShreya Shukla Case Study-2Rishabh UpadhyayNo ratings yet
- Detect Me: DirectionDocument6 pagesDetect Me: DirectionMaymay Auau100% (2)
- ELECTRICAL QUESTIONS AND ANSWERS-MCQ-9A - ETO - Electro Technical OfficerDocument11 pagesELECTRICAL QUESTIONS AND ANSWERS-MCQ-9A - ETO - Electro Technical Officeramit100% (2)
- Assessment of Critical Success FactorsDocument34 pagesAssessment of Critical Success FactorsTMC officeNo ratings yet