
Personal Information Form 08
Personal Information Form 08
You might also like
- Community-Led Health Equity Impact Assessment - Save Burdett CoalitionDocument32 pagesCommunity-Led Health Equity Impact Assessment - Save Burdett CoalitionRachel SilbersteinNo ratings yet
- Victorian AOD Intake ToolDocument5 pagesVictorian AOD Intake ToolHarjotBrarNo ratings yet
- Registration Form: St. Jude General Hospital and Medical CenterDocument1 pageRegistration Form: St. Jude General Hospital and Medical CenterTon RiveraNo ratings yet
- Snap IV InstructionsDocument2 pagesSnap IV Instructionsverouka100% (1)
- Pharmacology Alphabet AllDocument4 pagesPharmacology Alphabet Allsflower85No ratings yet
- Company Employee Form PDFDocument2 pagesCompany Employee Form PDFblindskateNo ratings yet
- THAS - Referral Form 2022Document2 pagesTHAS - Referral Form 2022NemesisNo ratings yet
- ST - Amant Clinical Services External Referral Dec 2021 3Document3 pagesST - Amant Clinical Services External Referral Dec 2021 3dsoucyNo ratings yet
- Initial Interview FormDocument1 pageInitial Interview FormStephan ChiariniNo ratings yet
- Referral Form Template 15Document1 pageReferral Form Template 15tanyalyn salvadorNo ratings yet
- Demographics: Subject Initials Subject ID DateDocument2 pagesDemographics: Subject Initials Subject ID DateAnusha DenduluriNo ratings yet
- IPRFormDocument2 pagesIPRFormSuvendu SahaNo ratings yet
- Patient Registration Form 1 2018 Adult UpdatedDocument4 pagesPatient Registration Form 1 2018 Adult UpdatedEskinderNo ratings yet
- Blank History FormDocument9 pagesBlank History FormlatashaNo ratings yet
- Case HX SLP AdultDocument2 pagesCase HX SLP AdultHarshit AmbeshNo ratings yet
- Benjs Medicenter Patient InformationDocument1 pageBenjs Medicenter Patient InformationcharNo ratings yet
- Checklist For New Patients or Prior Patients Not Seen Within 3 YearsDocument20 pagesChecklist For New Patients or Prior Patients Not Seen Within 3 YearsRebecca KnightNo ratings yet
- Admission Form - Kooweerup Regional Health ServiceDocument1 pageAdmission Form - Kooweerup Regional Health ServiceAileen ThomsNo ratings yet
- Ron Edeal, MFT, Intake Form: Client Name: DateDocument1 pageRon Edeal, MFT, Intake Form: Client Name: DateanitnerolNo ratings yet
- Merged Forms File For Website 5Document5 pagesMerged Forms File For Website 5ann hillNo ratings yet
- Employment Application Form-DASSDocument2 pagesEmployment Application Form-DASSnavin212No ratings yet
- Reg Form1Document2 pagesReg Form1api-289158317No ratings yet
- NC ITP Referral FormDocument1 pageNC ITP Referral Form『7mD〆 ٰNo ratings yet
- Application For Household Support GrantDocument5 pagesApplication For Household Support GrantgbabunetNo ratings yet
- New-Medical History Form - Clearly Orthodontics With Social MediaDocument2 pagesNew-Medical History Form - Clearly Orthodontics With Social MediaAatekaNo ratings yet
- Solicitud de Empleo.1Document3 pagesSolicitud de Empleo.1Heidy Lucia Lopez JuarezNo ratings yet
- Cannalogue Medical DocumentDocument1 pageCannalogue Medical DocumentolgaNo ratings yet
- Write Clearly and in Block Letters: Personal DataDocument2 pagesWrite Clearly and in Block Letters: Personal DataIrfan MustafaiNo ratings yet
- Patient Reg Packet MH.1.29.22Document6 pagesPatient Reg Packet MH.1.29.22Michael FullwoodNo ratings yet
- TGI Employment Application FormDocument2 pagesTGI Employment Application FormReago FedelinNo ratings yet
- TGI Employment Application FormDocument2 pagesTGI Employment Application FormReago FedelinNo ratings yet
- Self Referral Application Form: If You Need Any Help To Complete This Form Please CallDocument4 pagesSelf Referral Application Form: If You Need Any Help To Complete This Form Please CallMay Myat MonNo ratings yet
- 4 Yeldall Application Form PrintableDocument10 pages4 Yeldall Application Form Printableapi-634298404No ratings yet
- Pediatric Patient Registration Form TemplateDocument5 pagesPediatric Patient Registration Form TemplateHasfi YakobNo ratings yet
- Patient Admission Form Sept2014Document1 pagePatient Admission Form Sept2014elmore kakaNo ratings yet
- 5f46c432d9030864565565a15bd2c OriginalDocument7 pages5f46c432d9030864565565a15bd2c OriginalFawwaaz DamareeNo ratings yet
- Adult Registration Form - The Hall Practice (Jan 2020)Document6 pagesAdult Registration Form - The Hall Practice (Jan 2020)Kishan SthankiyaNo ratings yet
- Youth Club App PhillyDocument3 pagesYouth Club App Phillyapi-357278378No ratings yet
- Youth Fellowship Registration Form: NameDocument1 pageYouth Fellowship Registration Form: NameSteven MitchellNo ratings yet
- TSCC Registration Forms 2023Document4 pagesTSCC Registration Forms 2023api-251804492No ratings yet
- Ableliving Application FormDocument5 pagesAbleliving Application FormBezimeni BezimenovicNo ratings yet
- Athithi Application FormDocument1 pageAthithi Application Formnazeemashihab2006No ratings yet
- What My Family Should Know: A Guide For Getting Your Affairs in OrderDocument24 pagesWhat My Family Should Know: A Guide For Getting Your Affairs in OrderDheeraj GuptaNo ratings yet
- Referral Form NavanDocument2 pagesReferral Form Navankayleighquinn89No ratings yet
- 1.formal ApplicationDocument8 pages1.formal ApplicationNaturalBite ChefNo ratings yet
- Employee Personal ProfileDocument3 pagesEmployee Personal ProfileGeorge RizkNo ratings yet
- Espoir Academy Admission Application Editable 3.0Document3 pagesEspoir Academy Admission Application Editable 3.0regan.chetty07No ratings yet
- Division of Developmental Disabilities: Community Services Cover SheetDocument30 pagesDivision of Developmental Disabilities: Community Services Cover Sheetmjkd56No ratings yet
- Application FormDocument2 pagesApplication FormBrookeNo ratings yet
- Application SheetDocument2 pagesApplication SheetErickha GazaNo ratings yet
- Risima Apllication FormDocument11 pagesRisima Apllication FormdulciholdingsNo ratings yet
- Victim Informatio N Form - For "Complaina NT" or "Civil Party" (English)Document5 pagesVictim Informatio N Form - For "Complaina NT" or "Civil Party" (English)kilettersNo ratings yet
- Colour Labels Limited Employee Information: Personal Information (Attach Copies of Statutory Documents)Document4 pagesColour Labels Limited Employee Information: Personal Information (Attach Copies of Statutory Documents)JamesNo ratings yet
- Health Registration Form - InternationalDocument3 pagesHealth Registration Form - Internationaldolapo BalogunNo ratings yet
- Sewb ReferralDocument1 pageSewb Referralapi-311640433No ratings yet
- QF Maf 171 Professional Staff Application PDFDocument7 pagesQF Maf 171 Professional Staff Application PDFAJNCNo ratings yet
- Application Form (Chev/1)Document8 pagesApplication Form (Chev/1)aver04No ratings yet
- Registration FormDocument1 pageRegistration Formkatie_luvstamiiNo ratings yet
- DS 160Document5 pagesDS 160Bert SantosNo ratings yet
- Formulari I AplikimitDocument4 pagesFormulari I AplikimitHuti NoelNo ratings yet
- INSTRUCTIONS: Copiesoftheaccomplishedformwillbecarefully: ID Picture 2x2Document2 pagesINSTRUCTIONS: Copiesoftheaccomplishedformwillbecarefully: ID Picture 2x2Missy AcostaNo ratings yet
- Application Form For Free Advertisement: Institute InformationDocument2 pagesApplication Form For Free Advertisement: Institute InformationmanirocsNo ratings yet
- Divorce in Washington: The Legal Process, Your Rights, and What to ExpectFrom EverandDivorce in Washington: The Legal Process, Your Rights, and What to ExpectNo ratings yet
- Hyderabad: Cortico-Basal Implantology CourseDocument6 pagesHyderabad: Cortico-Basal Implantology CourseYousuf AdamNo ratings yet
- Laporan Penggunaan Obat Rasional (Diagnosa: Ispa)Document8 pagesLaporan Penggunaan Obat Rasional (Diagnosa: Ispa)SessyNo ratings yet
- PasienDocument12 pagesPasienDharma Abdi Riel ManullangNo ratings yet
- Contemporary Perspectives On Ageism: Liat Ayalon Clemens Tesch-Römer EditorsDocument582 pagesContemporary Perspectives On Ageism: Liat Ayalon Clemens Tesch-Römer EditorsLi Perfect100% (1)
- Multiple Trauma Vs Multiple FractureDocument35 pagesMultiple Trauma Vs Multiple Fracturetayyoo1302No ratings yet
- Poultry Health ManagementDocument32 pagesPoultry Health Managementdawn100% (2)
- 21 - 6182 - e (C) - PF1 (M) - F (P) - PF1 (PP) - Pfa (PR)Document3 pages21 - 6182 - e (C) - PF1 (M) - F (P) - PF1 (PP) - Pfa (PR)Vinna KusumawatiNo ratings yet
- ConsentDocument2 pagesConsentbipinNo ratings yet
- Radiol 13121947Document7 pagesRadiol 13121947Eduardo Agustín Vargas CamposNo ratings yet
- Syndarogya Proposal Form: Synbk Code Bic Code 9 2 1 0 0 0Document2 pagesSyndarogya Proposal Form: Synbk Code Bic Code 9 2 1 0 0 0Akhil ShastryNo ratings yet
- Gastric Lavage - Position Statement 2013Document7 pagesGastric Lavage - Position Statement 2013UrgenciasCol FoamNo ratings yet
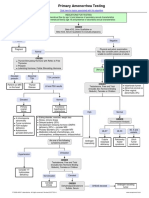
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Lennox Gastaut SyndromeDocument12 pagesLennox Gastaut SyndromedulcejuvennyNo ratings yet
- Uterine Atony: Cudanin, Regine R. Kimaykimay, Angeline PDocument31 pagesUterine Atony: Cudanin, Regine R. Kimaykimay, Angeline PregNo ratings yet
- Primary Biliary CholangitisDocument23 pagesPrimary Biliary CholangitisAbdul hadiNo ratings yet
- Clinical Pharmacy 3Document19 pagesClinical Pharmacy 3dlazkaywanNo ratings yet
- Study Closely The Concept Map On Sudden Pregnancy ComplicationsDocument13 pagesStudy Closely The Concept Map On Sudden Pregnancy ComplicationsJek Dela CruzNo ratings yet
- Edgar CayceDocument15 pagesEdgar CayceAlenka VenišnikNo ratings yet
- Adr FormDocument2 pagesAdr FormSachin Kumar PrajapatiNo ratings yet
- Peripartum CardiomyopathyDocument18 pagesPeripartum CardiomyopathyMJ WesleyNo ratings yet
- Case Analysis SchizophreniaDocument2 pagesCase Analysis Schizophreniamark OrpillaNo ratings yet
- Case On TrachomaDocument20 pagesCase On Trachomadimple alluriNo ratings yet
- Implementing Improvement Strategies To Prevent Unplanned Extubation in Neonatal Intensive Care Units - SLIDE DECKDocument19 pagesImplementing Improvement Strategies To Prevent Unplanned Extubation in Neonatal Intensive Care Units - SLIDE DECKeman hamzaNo ratings yet
- Icd-9-Cm RizDocument33 pagesIcd-9-Cm RizDinky AndreanNo ratings yet
- Holistic Nursing Care: Theories and Perspectives: February 2013Document6 pagesHolistic Nursing Care: Theories and Perspectives: February 2013Aulia Al JamalulaiiNo ratings yet






















































































Download as doc, pdf, or txt
You might also like
- Community-Led Health Equity Impact Assessment - Save Burdett CoalitionDocument32 pagesCommunity-Led Health Equity Impact Assessment - Save Burdett CoalitionRachel SilbersteinNo ratings yet
- Victorian AOD Intake ToolDocument5 pagesVictorian AOD Intake ToolHarjotBrarNo ratings yet
- Registration Form: St. Jude General Hospital and Medical CenterDocument1 pageRegistration Form: St. Jude General Hospital and Medical CenterTon RiveraNo ratings yet
- Snap IV InstructionsDocument2 pagesSnap IV Instructionsverouka100% (1)
- Pharmacology Alphabet AllDocument4 pagesPharmacology Alphabet Allsflower85No ratings yet
- Company Employee Form PDFDocument2 pagesCompany Employee Form PDFblindskateNo ratings yet
- THAS - Referral Form 2022Document2 pagesTHAS - Referral Form 2022NemesisNo ratings yet
- ST - Amant Clinical Services External Referral Dec 2021 3Document3 pagesST - Amant Clinical Services External Referral Dec 2021 3dsoucyNo ratings yet
- Initial Interview FormDocument1 pageInitial Interview FormStephan ChiariniNo ratings yet
- Referral Form Template 15Document1 pageReferral Form Template 15tanyalyn salvadorNo ratings yet
- Demographics: Subject Initials Subject ID DateDocument2 pagesDemographics: Subject Initials Subject ID DateAnusha DenduluriNo ratings yet
- IPRFormDocument2 pagesIPRFormSuvendu SahaNo ratings yet
- Patient Registration Form 1 2018 Adult UpdatedDocument4 pagesPatient Registration Form 1 2018 Adult UpdatedEskinderNo ratings yet
- Blank History FormDocument9 pagesBlank History FormlatashaNo ratings yet
- Case HX SLP AdultDocument2 pagesCase HX SLP AdultHarshit AmbeshNo ratings yet
- Benjs Medicenter Patient InformationDocument1 pageBenjs Medicenter Patient InformationcharNo ratings yet
- Checklist For New Patients or Prior Patients Not Seen Within 3 YearsDocument20 pagesChecklist For New Patients or Prior Patients Not Seen Within 3 YearsRebecca KnightNo ratings yet
- Admission Form - Kooweerup Regional Health ServiceDocument1 pageAdmission Form - Kooweerup Regional Health ServiceAileen ThomsNo ratings yet
- Ron Edeal, MFT, Intake Form: Client Name: DateDocument1 pageRon Edeal, MFT, Intake Form: Client Name: DateanitnerolNo ratings yet
- Merged Forms File For Website 5Document5 pagesMerged Forms File For Website 5ann hillNo ratings yet
- Employment Application Form-DASSDocument2 pagesEmployment Application Form-DASSnavin212No ratings yet
- Reg Form1Document2 pagesReg Form1api-289158317No ratings yet
- NC ITP Referral FormDocument1 pageNC ITP Referral Form『7mD〆 ٰNo ratings yet
- Application For Household Support GrantDocument5 pagesApplication For Household Support GrantgbabunetNo ratings yet
- New-Medical History Form - Clearly Orthodontics With Social MediaDocument2 pagesNew-Medical History Form - Clearly Orthodontics With Social MediaAatekaNo ratings yet
- Solicitud de Empleo.1Document3 pagesSolicitud de Empleo.1Heidy Lucia Lopez JuarezNo ratings yet
- Cannalogue Medical DocumentDocument1 pageCannalogue Medical DocumentolgaNo ratings yet
- Write Clearly and in Block Letters: Personal DataDocument2 pagesWrite Clearly and in Block Letters: Personal DataIrfan MustafaiNo ratings yet
- Patient Reg Packet MH.1.29.22Document6 pagesPatient Reg Packet MH.1.29.22Michael FullwoodNo ratings yet
- TGI Employment Application FormDocument2 pagesTGI Employment Application FormReago FedelinNo ratings yet
- TGI Employment Application FormDocument2 pagesTGI Employment Application FormReago FedelinNo ratings yet
- Self Referral Application Form: If You Need Any Help To Complete This Form Please CallDocument4 pagesSelf Referral Application Form: If You Need Any Help To Complete This Form Please CallMay Myat MonNo ratings yet
- 4 Yeldall Application Form PrintableDocument10 pages4 Yeldall Application Form Printableapi-634298404No ratings yet
- Pediatric Patient Registration Form TemplateDocument5 pagesPediatric Patient Registration Form TemplateHasfi YakobNo ratings yet
- Patient Admission Form Sept2014Document1 pagePatient Admission Form Sept2014elmore kakaNo ratings yet
- 5f46c432d9030864565565a15bd2c OriginalDocument7 pages5f46c432d9030864565565a15bd2c OriginalFawwaaz DamareeNo ratings yet
- Adult Registration Form - The Hall Practice (Jan 2020)Document6 pagesAdult Registration Form - The Hall Practice (Jan 2020)Kishan SthankiyaNo ratings yet
- Youth Club App PhillyDocument3 pagesYouth Club App Phillyapi-357278378No ratings yet
- Youth Fellowship Registration Form: NameDocument1 pageYouth Fellowship Registration Form: NameSteven MitchellNo ratings yet
- TSCC Registration Forms 2023Document4 pagesTSCC Registration Forms 2023api-251804492No ratings yet
- Ableliving Application FormDocument5 pagesAbleliving Application FormBezimeni BezimenovicNo ratings yet
- Athithi Application FormDocument1 pageAthithi Application Formnazeemashihab2006No ratings yet
- What My Family Should Know: A Guide For Getting Your Affairs in OrderDocument24 pagesWhat My Family Should Know: A Guide For Getting Your Affairs in OrderDheeraj GuptaNo ratings yet
- Referral Form NavanDocument2 pagesReferral Form Navankayleighquinn89No ratings yet
- 1.formal ApplicationDocument8 pages1.formal ApplicationNaturalBite ChefNo ratings yet
- Employee Personal ProfileDocument3 pagesEmployee Personal ProfileGeorge RizkNo ratings yet
- Espoir Academy Admission Application Editable 3.0Document3 pagesEspoir Academy Admission Application Editable 3.0regan.chetty07No ratings yet
- Division of Developmental Disabilities: Community Services Cover SheetDocument30 pagesDivision of Developmental Disabilities: Community Services Cover Sheetmjkd56No ratings yet
- Application FormDocument2 pagesApplication FormBrookeNo ratings yet
- Application SheetDocument2 pagesApplication SheetErickha GazaNo ratings yet
- Risima Apllication FormDocument11 pagesRisima Apllication FormdulciholdingsNo ratings yet
- Victim Informatio N Form - For "Complaina NT" or "Civil Party" (English)Document5 pagesVictim Informatio N Form - For "Complaina NT" or "Civil Party" (English)kilettersNo ratings yet
- Colour Labels Limited Employee Information: Personal Information (Attach Copies of Statutory Documents)Document4 pagesColour Labels Limited Employee Information: Personal Information (Attach Copies of Statutory Documents)JamesNo ratings yet
- Health Registration Form - InternationalDocument3 pagesHealth Registration Form - Internationaldolapo BalogunNo ratings yet
- Sewb ReferralDocument1 pageSewb Referralapi-311640433No ratings yet
- QF Maf 171 Professional Staff Application PDFDocument7 pagesQF Maf 171 Professional Staff Application PDFAJNCNo ratings yet
- Application Form (Chev/1)Document8 pagesApplication Form (Chev/1)aver04No ratings yet
- Registration FormDocument1 pageRegistration Formkatie_luvstamiiNo ratings yet
- DS 160Document5 pagesDS 160Bert SantosNo ratings yet
- Formulari I AplikimitDocument4 pagesFormulari I AplikimitHuti NoelNo ratings yet
- INSTRUCTIONS: Copiesoftheaccomplishedformwillbecarefully: ID Picture 2x2Document2 pagesINSTRUCTIONS: Copiesoftheaccomplishedformwillbecarefully: ID Picture 2x2Missy AcostaNo ratings yet
- Application Form For Free Advertisement: Institute InformationDocument2 pagesApplication Form For Free Advertisement: Institute InformationmanirocsNo ratings yet
- Divorce in Washington: The Legal Process, Your Rights, and What to ExpectFrom EverandDivorce in Washington: The Legal Process, Your Rights, and What to ExpectNo ratings yet
- Hyderabad: Cortico-Basal Implantology CourseDocument6 pagesHyderabad: Cortico-Basal Implantology CourseYousuf AdamNo ratings yet
- Laporan Penggunaan Obat Rasional (Diagnosa: Ispa)Document8 pagesLaporan Penggunaan Obat Rasional (Diagnosa: Ispa)SessyNo ratings yet
- PasienDocument12 pagesPasienDharma Abdi Riel ManullangNo ratings yet
- Contemporary Perspectives On Ageism: Liat Ayalon Clemens Tesch-Römer EditorsDocument582 pagesContemporary Perspectives On Ageism: Liat Ayalon Clemens Tesch-Römer EditorsLi Perfect100% (1)
- Multiple Trauma Vs Multiple FractureDocument35 pagesMultiple Trauma Vs Multiple Fracturetayyoo1302No ratings yet
- Poultry Health ManagementDocument32 pagesPoultry Health Managementdawn100% (2)
- 21 - 6182 - e (C) - PF1 (M) - F (P) - PF1 (PP) - Pfa (PR)Document3 pages21 - 6182 - e (C) - PF1 (M) - F (P) - PF1 (PP) - Pfa (PR)Vinna KusumawatiNo ratings yet
- ConsentDocument2 pagesConsentbipinNo ratings yet
- Radiol 13121947Document7 pagesRadiol 13121947Eduardo Agustín Vargas CamposNo ratings yet
- Syndarogya Proposal Form: Synbk Code Bic Code 9 2 1 0 0 0Document2 pagesSyndarogya Proposal Form: Synbk Code Bic Code 9 2 1 0 0 0Akhil ShastryNo ratings yet
- Gastric Lavage - Position Statement 2013Document7 pagesGastric Lavage - Position Statement 2013UrgenciasCol FoamNo ratings yet
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Lennox Gastaut SyndromeDocument12 pagesLennox Gastaut SyndromedulcejuvennyNo ratings yet
- Uterine Atony: Cudanin, Regine R. Kimaykimay, Angeline PDocument31 pagesUterine Atony: Cudanin, Regine R. Kimaykimay, Angeline PregNo ratings yet
- Primary Biliary CholangitisDocument23 pagesPrimary Biliary CholangitisAbdul hadiNo ratings yet
- Clinical Pharmacy 3Document19 pagesClinical Pharmacy 3dlazkaywanNo ratings yet
- Study Closely The Concept Map On Sudden Pregnancy ComplicationsDocument13 pagesStudy Closely The Concept Map On Sudden Pregnancy ComplicationsJek Dela CruzNo ratings yet
- Edgar CayceDocument15 pagesEdgar CayceAlenka VenišnikNo ratings yet
- Adr FormDocument2 pagesAdr FormSachin Kumar PrajapatiNo ratings yet
- Peripartum CardiomyopathyDocument18 pagesPeripartum CardiomyopathyMJ WesleyNo ratings yet
- Case Analysis SchizophreniaDocument2 pagesCase Analysis Schizophreniamark OrpillaNo ratings yet
- Case On TrachomaDocument20 pagesCase On Trachomadimple alluriNo ratings yet
- Implementing Improvement Strategies To Prevent Unplanned Extubation in Neonatal Intensive Care Units - SLIDE DECKDocument19 pagesImplementing Improvement Strategies To Prevent Unplanned Extubation in Neonatal Intensive Care Units - SLIDE DECKeman hamzaNo ratings yet
- Icd-9-Cm RizDocument33 pagesIcd-9-Cm RizDinky AndreanNo ratings yet
- Holistic Nursing Care: Theories and Perspectives: February 2013Document6 pagesHolistic Nursing Care: Theories and Perspectives: February 2013Aulia Al JamalulaiiNo ratings yet