Download as pdf or txt
You might also like
- Dentin As A Bonding SubstrateDocument27 pagesDentin As A Bonding SubstrateAle MonzalvoNo ratings yet
- AUOBF Manual Activity 5Document3 pagesAUOBF Manual Activity 5Hannah SalendabNo ratings yet
- IAAD Working Instructions - Light CuringDocument3 pagesIAAD Working Instructions - Light CuringgabyNo ratings yet
- Immediate Dental Implant Placement Into Infected vs. Non-Infected Sockets: A Meta-AnalysisDocument7 pagesImmediate Dental Implant Placement Into Infected vs. Non-Infected Sockets: A Meta-Analysismarlene tamayoNo ratings yet
- Terry Part-One PDFDocument8 pagesTerry Part-One PDFhptuanamaNo ratings yet
- Accelerated Fatigue Resistance of Thick CAD/CAM Composite Resin Overlays Bonded With Light - and Dual-Polymerizing Luting ResinsDocument8 pagesAccelerated Fatigue Resistance of Thick CAD/CAM Composite Resin Overlays Bonded With Light - and Dual-Polymerizing Luting ResinsTiago SpeziaNo ratings yet
- Bioemulation PDFDocument13 pagesBioemulation PDFjotapintor100% (1)
- Ultimate Ceramic Veneers A Laboratory-Guided Ultraconservative PreparationDocument15 pagesUltimate Ceramic Veneers A Laboratory-Guided Ultraconservative PreparationEvelina HaddadienNo ratings yet
- 3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFDocument10 pages3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFAnisha AnilNo ratings yet
- 2011 FERRACANE Resin Composite-State of The Art - pontONSDocument10 pages2011 FERRACANE Resin Composite-State of The Art - pontONSSandra RojasNo ratings yet
- PRD 22 5 Magne1Document10 pagesPRD 22 5 Magne1sofa83No ratings yet
- Occlusal Considerations For Full-Arch Implant-Supported Prostheses - A Guideline (2022)Document5 pagesOcclusal Considerations For Full-Arch Implant-Supported Prostheses - A Guideline (2022)Francisca Dinamarca LamaNo ratings yet
- Selective Caries ExcavationDocument10 pagesSelective Caries Excavationjorefe12No ratings yet
- 10 1016@j Prosdent 2020 05 007Document5 pages10 1016@j Prosdent 2020 05 007Anjali DuttaNo ratings yet
- Prepared Cavities On The StrenDocument4 pagesPrepared Cavities On The StrenPriyank RaiNo ratings yet
- DelipariJAD2008 RibbondPostDocument8 pagesDelipariJAD2008 RibbondPostDeno MerindaNo ratings yet
- Greene & Manfredini 2023 - Overtreatment Successes - 230709 - 135204Document11 pagesGreene & Manfredini 2023 - Overtreatment Successes - 230709 - 135204Abigail HernándezNo ratings yet
- Deliperi S - PPAD - 2005 PDFDocument9 pagesDeliperi S - PPAD - 2005 PDFAlfredo PortocarreroNo ratings yet
- Denu 2017 44 9 821Document7 pagesDenu 2017 44 9 821Yolanda EvansNo ratings yet
- Managing The Unstable CDDocument8 pagesManaging The Unstable CDNajeeb UllahNo ratings yet
- The Endocrown - A Different Type of All-Ceramic Reconstruction For Molars - JcdaDocument10 pagesThe Endocrown - A Different Type of All-Ceramic Reconstruction For Molars - Jcdaabcder1234No ratings yet
- GTC 4 - Impressions & Retraction Cord (PPSG Lectures)Document34 pagesGTC 4 - Impressions & Retraction Cord (PPSG Lectures)Aisha MutiaraNo ratings yet
- Eur JEsthet Dent 2013 MeyenbergDocument97 pagesEur JEsthet Dent 2013 Meyenbergsoma kiranNo ratings yet
- Real-Time In-Depth Imaging of Gap Formation in Bulk-Fill Resin CompositesDocument12 pagesReal-Time In-Depth Imaging of Gap Formation in Bulk-Fill Resin CompositesPaula Francisca MoragaNo ratings yet
- The Use of Separating Rings in The Placement of Class II Composite ResinsDocument9 pagesThe Use of Separating Rings in The Placement of Class II Composite ResinsLeslie MorrowNo ratings yet
- Digital Smile Design - Predictable Results (#741934) - 1117267Document6 pagesDigital Smile Design - Predictable Results (#741934) - 1117267yuumiNo ratings yet
- The Dahl Concept Past Present and FutureDocument9 pagesThe Dahl Concept Past Present and FuturevivigaitanNo ratings yet
- Restorative Gap Management in The Esthetic Zone Dental Book NetDocument347 pagesRestorative Gap Management in The Esthetic Zone Dental Book NetLorena LlancariNo ratings yet
- Periodontal-Restorative Interactions: A Review: DentistryDocument7 pagesPeriodontal-Restorative Interactions: A Review: DentistrySahana RangarajanNo ratings yet
- IJEDe 15 03 Rocca 852 2Document22 pagesIJEDe 15 03 Rocca 852 2hannaly estradaNo ratings yet
- Biologic Interfaces in Esthetic Dentistry. Part I: The Perio/restorative InterfaceDocument21 pagesBiologic Interfaces in Esthetic Dentistry. Part I: The Perio/restorative InterfaceRoopa BabannavarNo ratings yet
- Micro and Macro Dental Esthetics: The Key To Smile IndividualizationDocument14 pagesMicro and Macro Dental Esthetics: The Key To Smile IndividualizationRoo GaunaNo ratings yet
- Fracture Resistance of Endodontically Treated Teeth Without Ferrule Using A Novel H-Shaped Short PostDocument13 pagesFracture Resistance of Endodontically Treated Teeth Without Ferrule Using A Novel H-Shaped Short PostTiago CostaNo ratings yet
- Posterior Composite Restoration UpdateDocument10 pagesPosterior Composite Restoration UpdateBianca IovoaiaNo ratings yet
- Digital Smile Design in Prosthodontics - An OverviewDocument7 pagesDigital Smile Design in Prosthodontics - An OverviewGanesh Pavan Kumar KarriNo ratings yet
- Amalgam Vs CompositeDocument58 pagesAmalgam Vs Compositeanmol0% (1)
- JC 12 Clinical Efficacy of Methods For Bonding To ZirconiaDocument37 pagesJC 12 Clinical Efficacy of Methods For Bonding To ZirconiaMrinmayee ThakurNo ratings yet
- Implants in Esthetic ZoneDocument10 pagesImplants in Esthetic ZoneInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Implant Thread Designs: An Overview: July 2017Document10 pagesImplant Thread Designs: An Overview: July 2017Seno FauziNo ratings yet
- Decoupling With Time - Inside Dentistry - August 2021 - Inside Dentistry - CDEWoDocument7 pagesDecoupling With Time - Inside Dentistry - August 2021 - Inside Dentistry - CDEWoBreno VictorNo ratings yet
- Longevity and Reasons For Failure of Sandwich and Total-Etch Posterior Composite Resin RestorationsDocument7 pagesLongevity and Reasons For Failure of Sandwich and Total-Etch Posterior Composite Resin RestorationsMAYRA ALEJANDRA BAHAMON TRUJILLONo ratings yet
- 3 - Matrix Systems and The Class II Composite Resin PDFDocument8 pages3 - Matrix Systems and The Class II Composite Resin PDFRaissa IcaNo ratings yet
- The Protocols of Biomimetic Restorative Dentistry - 2002 To 2017 - June 2017 - Inside DentistryDocument7 pagesThe Protocols of Biomimetic Restorative Dentistry - 2002 To 2017 - June 2017 - Inside DentistrysonaliNo ratings yet
- The Simultaneous Modeling Technique Closing Gaps in PosteriorsDocument24 pagesThe Simultaneous Modeling Technique Closing Gaps in PosteriorsÄpriolia SuNo ratings yet
- Is Fracture Resistance of Endodontically Treated Mandibular Molars Restored With Indirect Onlay Composite Restorations Influenced by Fibre Post Insertion?Document7 pagesIs Fracture Resistance of Endodontically Treated Mandibular Molars Restored With Indirect Onlay Composite Restorations Influenced by Fibre Post Insertion?Millie Vega100% (1)
- Esthetic Considerations in Interdental Papilla PDFDocument11 pagesEsthetic Considerations in Interdental Papilla PDFXavier AltamiranoNo ratings yet
- Papper PeriodDocument12 pagesPapper PeriodLoretoReyesMoralesNo ratings yet
- Journal-A Dental Esthetic Checklist For Treatment Planning in Esthetic DentistryDocument8 pagesJournal-A Dental Esthetic Checklist For Treatment Planning in Esthetic Dentistryalmond_pretzelNo ratings yet
- 20 2003 - Magne - Anatomic Crown Width LengthDocument9 pages20 2003 - Magne - Anatomic Crown Width LengthSilvia KriNo ratings yet
- Healing Following Implant Surgery: Osseous Healing-Early PhaseDocument2 pagesHealing Following Implant Surgery: Osseous Healing-Early PhaseUrjita PatilNo ratings yet
- Nanofilled Resin Composite Properties and Clinical Performance - A ReviewDocument18 pagesNanofilled Resin Composite Properties and Clinical Performance - A ReviewInside Dentistry educationNo ratings yet
- Blanqueamiento No Vital PDFDocument11 pagesBlanqueamiento No Vital PDFPatricio Alejandro Cornejo Mutizabal100% (1)
- Full Mouth ReconstructDocument5 pagesFull Mouth ReconstructMuaiyed Buzayan AkremyNo ratings yet
- Anderson (1985) A Comparison of Digital and Optical Criteria For Detecting Carious DentinDocument4 pagesAnderson (1985) A Comparison of Digital and Optical Criteria For Detecting Carious DentinОлександр БайдоNo ratings yet
- Reconstruction of The Lost Interproximal Papilla - Presentation of Surgical and Nonsurgical Approaches.Document14 pagesReconstruction of The Lost Interproximal Papilla - Presentation of Surgical and Nonsurgical Approaches.EugenioNo ratings yet
- Clinical Performance of Novel-Design Porcelain Veneers For The Recovery of Coronal Volume and LengthDocument18 pagesClinical Performance of Novel-Design Porcelain Veneers For The Recovery of Coronal Volume and LengthZardasht NajmadineNo ratings yet
- Adhesion of Resin Cement To Dentin Effec PDFDocument12 pagesAdhesion of Resin Cement To Dentin Effec PDFNathaly Granda ZapataNo ratings yet
- Linkevisius Ti-BaseDocument6 pagesLinkevisius Ti-Basekatherina rozicNo ratings yet
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionFrom EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionNo ratings yet
- Reflective Journal 4Document2 pagesReflective Journal 4api-350779667No ratings yet
- Patient and Family Discharge Checklist: Patient Name: Reason For AdmissionDocument7 pagesPatient and Family Discharge Checklist: Patient Name: Reason For Admissiondwirabiatul adwiyahaliNo ratings yet
- Assessment of The European Community System of PharmacovigilanceDocument199 pagesAssessment of The European Community System of PharmacovigilanceAde AddeNo ratings yet
- State Industrial Profile - Tamil Nadu - 4316Document193 pagesState Industrial Profile - Tamil Nadu - 4316Anonymous a8rdyKOCNo ratings yet
- Daftar Obat Slow MovingDocument54 pagesDaftar Obat Slow MovingANTONIUS BAYUNo ratings yet
- Active and Retentive Components of Ras 1-3-2011 TuesdayDocument15 pagesActive and Retentive Components of Ras 1-3-2011 TuesdayJustin SameulNo ratings yet
- Kirby Bauer Disc DiffusionDocument9 pagesKirby Bauer Disc DiffusionSubhradeep GhoshNo ratings yet
- Listening Practice 2Document5 pagesListening Practice 2Vy PhạmNo ratings yet
- Using Liquid Crystal Glasses To Treat Amblyopia in ChildrenDocument3 pagesUsing Liquid Crystal Glasses To Treat Amblyopia in ChildrenWagner de AvizNo ratings yet
- Search Results: Rasa Shastra: The Hidden Art of Medical AlchemyDocument1 pageSearch Results: Rasa Shastra: The Hidden Art of Medical AlchemyneelNo ratings yet
- Breaking Down BloodDocument2 pagesBreaking Down BloodWWMTNo ratings yet
- Technical Specifications of Enterprise5000AP & 8000X - 03-09-2020Document3 pagesTechnical Specifications of Enterprise5000AP & 8000X - 03-09-2020WALFS Infra MeridianNo ratings yet
- Capsaicina Tópica en El Tratamiento Del Dolor Neuropático: RevisiónDocument13 pagesCapsaicina Tópica en El Tratamiento Del Dolor Neuropático: RevisiónJAVIER RODRIGUEZNo ratings yet
- Strength Duration Curves ProcedureDocument4 pagesStrength Duration Curves ProcedureDr GowrishankarPotturi PT67% (3)
- Eucast Rast Breakpoint Table V 4.0 PDFDocument14 pagesEucast Rast Breakpoint Table V 4.0 PDFGuneyden GuneydenNo ratings yet
- Record Penyerahan ApdDocument1 pageRecord Penyerahan ApdRejib KibarNo ratings yet
- (04!14!2023) Test-Service Orders 5Document3 pages(04!14!2023) Test-Service Orders 5koolkatashwoodNo ratings yet
- Adventist University of The Philippines: Dental ChartDocument6 pagesAdventist University of The Philippines: Dental ChartYossy TjahyonoNo ratings yet
- Extend - Bottled Balloons-1Document2 pagesExtend - Bottled Balloons-1TcherKamilaNo ratings yet
- SBAR - Major DepressionDocument3 pagesSBAR - Major DepressionTonya PhelpsNo ratings yet
- PranoyDocument24 pagesPranoySupriyo ChatterjeeNo ratings yet
- First AidDocument3 pagesFirst AidVince JaoNo ratings yet
- Bag Technique: PREPARED BY: Dr. Irynne D. Cabanban Prof. Emmanuel ImmaculataDocument35 pagesBag Technique: PREPARED BY: Dr. Irynne D. Cabanban Prof. Emmanuel ImmaculataClarissa Maglalang100% (2)
- C659BDocument3 pagesC659BDawn CasuncadNo ratings yet
- Print Ko BukasDocument3 pagesPrint Ko BukasKatrina CaveNo ratings yet
- 3M Avagard-Hand-Antiseptic-Data-Sheet PDFDocument6 pages3M Avagard-Hand-Antiseptic-Data-Sheet PDFHaitham AlbajawiNo ratings yet
- Immunization ScheduleDocument2 pagesImmunization ScheduleabdulNo ratings yet
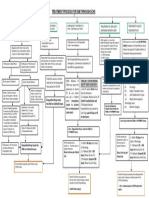
- Treatment Process For Esm Through Echs: Reqd)Document1 pageTreatment Process For Esm Through Echs: Reqd)Sasi KumarNo ratings yet
- Formulation and Evaluation of Immediate Release Tablets of AcyclovirDocument4 pagesFormulation and Evaluation of Immediate Release Tablets of Acyclovir9147Indah WulandariNo ratings yet