Download as pdf or txt
You might also like
- Rehab Cheat SheetDocument18 pagesRehab Cheat SheetZ A100% (3)
- Form - Student Health Certificate-1Document2 pagesForm - Student Health Certificate-1hmhida33% (3)
- Dentistry Reviewer: C. Tricuspid ValveDocument47 pagesDentistry Reviewer: C. Tricuspid ValvePatricia L.No ratings yet
- Biofilms and Their Role - 0Document4 pagesBiofilms and Their Role - 0ibrahimNo ratings yet
- Feridas CrônicasDocument12 pagesFeridas CrônicasANNE LOUISE FALCAO PASCOALNo ratings yet
- TB PDFDocument12 pagesTB PDFHana AshrafNo ratings yet
- International Wound Journal - 2018 - Percival - Role of Anaerobes in Polymicrobial Communities and Biofilms ComplicatingDocument7 pagesInternational Wound Journal - 2018 - Percival - Role of Anaerobes in Polymicrobial Communities and Biofilms ComplicatingIdamelis Rodríguez GarcíaNo ratings yet
- Staphylococcus Epidermidis: Bio®lms: Importance and ImplicationsDocument6 pagesStaphylococcus Epidermidis: Bio®lms: Importance and Implicationsferro indahNo ratings yet
- 2021 Article 624Document18 pages2021 Article 624icrgNo ratings yet
- Crit Care Nurse 2009 Knechel 34 43Document12 pagesCrit Care Nurse 2009 Knechel 34 43Hilman NurmahdiNo ratings yet
- The Role of Bacterial Biofilms in Device-Associated InfectionDocument10 pagesThe Role of Bacterial Biofilms in Device-Associated InfectionLorena Bellan DomicianoNo ratings yet
- Biofilm in OtorhinolaryngologyDocument10 pagesBiofilm in OtorhinolaryngologyMohammed SahibNo ratings yet
- Biofilms 2Document8 pagesBiofilms 2Nasir KhanNo ratings yet
- Staphylococcus BiofilmsDocument20 pagesStaphylococcus BiofilmsOssian89No ratings yet
- BiofilmDocument9 pagesBiofilmJorge W Henao MorenoNo ratings yet
- Breaking Down BiofilmsDocument3 pagesBreaking Down Biofilmsleila.hiloutNo ratings yet
- Lyong HaDocument2 pagesLyong HaZahraNo ratings yet
- Luka 2 PDFDocument6 pagesLuka 2 PDFBarryNo ratings yet
- JMB 31 1 1Document7 pagesJMB 31 1 1icrgNo ratings yet
- Biofilms - Definicion4Document5 pagesBiofilms - Definicion4Ignacio BeneméritoNo ratings yet
- Biofilms and Polimicrobial InfectionsDocument53 pagesBiofilms and Polimicrobial InfectionsMustafa JaradatNo ratings yet
- Biofilms in InfectionDocument53 pagesBiofilms in Infectionandyraff100% (2)
- Platelets y Escherichia ColiDocument12 pagesPlatelets y Escherichia Coliedson floresNo ratings yet
- Antibiotic Prophylaxis in Surgical Site Infection PreventionDocument7 pagesAntibiotic Prophylaxis in Surgical Site Infection PreventionlickyfrogyNo ratings yet
- Biofilm in DermatologyDocument5 pagesBiofilm in DermatologysovalaxNo ratings yet
- 395-404 5.55.15 PM 6.22.13 PM 6.23.17 PMDocument10 pages395-404 5.55.15 PM 6.22.13 PM 6.23.17 PMSaiful AbdulNo ratings yet
- Antibiotic Failure Beyond Antimicrobial Resistan - 2023 - Drug Resistance UpdatDocument28 pagesAntibiotic Failure Beyond Antimicrobial Resistan - 2023 - Drug Resistance UpdatDana MateiNo ratings yet
- Tsui 2016Document51 pagesTsui 2016Arika EffiyanaNo ratings yet
- Microbiology of Pathogenic Factors 2024Document40 pagesMicrobiology of Pathogenic Factors 2024aguilarjanicaNo ratings yet
- Opportunistic MycosesDocument7 pagesOpportunistic MycosesAbhishek ChandraNo ratings yet
- 01162020EDIT - Antimicrobial Activity of Vitex Negundo Leaf Extracts As An Antimicrobial CreamDocument51 pages01162020EDIT - Antimicrobial Activity of Vitex Negundo Leaf Extracts As An Antimicrobial CreamIanne Lorraine L. DANTENo ratings yet
- Maxillofacial MicrobiologyDocument60 pagesMaxillofacial MicrobiologyAbel AbrahamNo ratings yet
- Probiotic Escherichia Coli Inhibits Biofilm Formation of Pathogenic Ecoli Via Extracellular Activity of DegPDocument12 pagesProbiotic Escherichia Coli Inhibits Biofilm Formation of Pathogenic Ecoli Via Extracellular Activity of DegPBudi MulyawanNo ratings yet
- Morrison 2020Document17 pagesMorrison 2020ANGEL DANIEL CASTAÑEDA PAREDESNo ratings yet
- Microbioma y OtorrinoDocument19 pagesMicrobioma y Otorrinodayenu barraNo ratings yet
- Bacteri UlkusDocument6 pagesBacteri Ulkuseki_herawatiNo ratings yet
- Course NoteDocument135 pagesCourse NoteNat SattabongkodNo ratings yet
- Wajib - Tuberculosis - Pathophysiology, Clinical Features, and DiagnosisDocument12 pagesWajib - Tuberculosis - Pathophysiology, Clinical Features, and DiagnosisnurulahdiahNo ratings yet
- Chapter Overview: 8: FungiDocument17 pagesChapter Overview: 8: FungiBianca ElbrechtNo ratings yet
- Candida Albicans Biofilms and Polymicrobial InteractionsDocument22 pagesCandida Albicans Biofilms and Polymicrobial InteractionsCatalina AguayoNo ratings yet
- (7P) Host-Microbial Interactions in Periodontal DiseasesDocument6 pages(7P) Host-Microbial Interactions in Periodontal DiseasesNegrus StefanNo ratings yet
- Sharma Et Al-2016-Journal of Applied MicrobiologyDocument11 pagesSharma Et Al-2016-Journal of Applied MicrobiologyJoanaNo ratings yet
- Understanding The Immune SystemDocument8 pagesUnderstanding The Immune Systemmohamed waleedNo ratings yet
- The Role of Bacterial Biofilm in Persistent Infections and Control StrategiesDocument8 pagesThe Role of Bacterial Biofilm in Persistent Infections and Control StrategiesJenny TaylorNo ratings yet
- Wound Healing and Perioperative Care - Vol 18 Issue 1 Feb 2006 OmfsDocument7 pagesWound Healing and Perioperative Care - Vol 18 Issue 1 Feb 2006 Omfsapi-265532519No ratings yet
- Recent Trends On Wound Management: New Therapeutic Choices Based On Polymeric CarriersDocument24 pagesRecent Trends On Wound Management: New Therapeutic Choices Based On Polymeric Carriersrozh rasulNo ratings yet
- SummaryDocument11 pagesSummaryNun NunNo ratings yet
- Cutaneous Tuberculosis: Epidemiologic, Etiopathogenic and Clinical Aspects - Part IDocument10 pagesCutaneous Tuberculosis: Epidemiologic, Etiopathogenic and Clinical Aspects - Part IDellNo ratings yet
- Preventing Candida Albicans From Subverting Host Plasminogen For Invasive Infection TreatmentDocument17 pagesPreventing Candida Albicans From Subverting Host Plasminogen For Invasive Infection Treatmentvuongquynh290900No ratings yet
- Green DKK, 2015Document14 pagesGreen DKK, 2015Nabila NatasyaNo ratings yet
- 7307 12912 1 SMDocument11 pages7307 12912 1 SMRin ChanNo ratings yet
- Vol. 6, Issue 1, January 2018, PharmaTutor, Paper-2Document7 pagesVol. 6, Issue 1, January 2018, PharmaTutor, Paper-2mmmmmNo ratings yet
- Endemic Mycoses: Blastomycosis, Histoplasmosis, and SporotrichosisDocument18 pagesEndemic Mycoses: Blastomycosis, Histoplasmosis, and SporotrichosisaugustosavioNo ratings yet
- Mobley 2009Document40 pagesMobley 2009Cuy BordaNo ratings yet
- Wound Healing and Its Impairment in The Diabetic Foot: ReviewDocument9 pagesWound Healing and Its Impairment in The Diabetic Foot: ReviewJoey TsaiNo ratings yet
- 26 83 1 PBDocument4 pages26 83 1 PBINDRANo ratings yet
- Wound Infection SepsisDocument27 pagesWound Infection SepsisDonny Artya KesumaNo ratings yet
- Jurnal 3 MoluskumDocument2 pagesJurnal 3 MoluskumFausiah Ulva MNo ratings yet
- Biofilm Susceptibility To Antimicrobials: Abstract-Microbial Biofilms, Where Organisms AreDocument8 pagesBiofilm Susceptibility To Antimicrobials: Abstract-Microbial Biofilms, Where Organisms AresiribabummtNo ratings yet
- Immunology Notes WJEC 2022 SLJ 3Document37 pagesImmunology Notes WJEC 2022 SLJ 3zainpaNo ratings yet
- Female Urinary Tract Infections in Clinical PracticeFrom EverandFemale Urinary Tract Infections in Clinical PracticeBob YangNo ratings yet
- Clinical Relevance MicrobiologyDocument14 pagesClinical Relevance Microbiologyeva arna abrarNo ratings yet
- Modern Wound Care (Article Journal)Document14 pagesModern Wound Care (Article Journal)eva arna abrarNo ratings yet
- Identification InfectionDocument6 pagesIdentification Infectioneva arna abrarNo ratings yet
- Women & Diabetes Our Right To A Healthy FutureDocument4 pagesWomen & Diabetes Our Right To A Healthy Futureeva arna abrarNo ratings yet
- Biomarker For InfectionDocument21 pagesBiomarker For Infectioneva arna abrarNo ratings yet
- Bioburden in Chronic WoundDocument24 pagesBioburden in Chronic Woundeva arna abrarNo ratings yet
- Community Wound BacteriDocument11 pagesCommunity Wound Bacterieva arna abrarNo ratings yet
- Research Methods For Nurses and MidwivesDocument5 pagesResearch Methods For Nurses and Midwiveseva arna abrarNo ratings yet
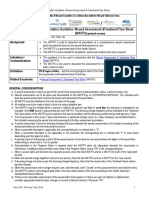
- Documentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)Document4 pagesDocumentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)eva arna abrarNo ratings yet
- Ound Ssessment and Anagement: Document Summary/Key PointsDocument21 pagesOund Ssessment and Anagement: Document Summary/Key Pointseva arna abrarNo ratings yet
- Management of Wounds in The Community: Five Principles: Clinical FocusDocument4 pagesManagement of Wounds in The Community: Five Principles: Clinical Focuseva arna abrarNo ratings yet
- Documentation Guideline: Wound Assessment &treatment Flow Sheet (WATFS) Portrait Version With PSLS#Document6 pagesDocumentation Guideline: Wound Assessment &treatment Flow Sheet (WATFS) Portrait Version With PSLS#eva arna abrarNo ratings yet
- Dr. Ashman's ENT Notes PDFDocument56 pagesDr. Ashman's ENT Notes PDFJulian GordonNo ratings yet
- All Things MoringaDocument40 pagesAll Things MoringaAnjee SugatriNo ratings yet
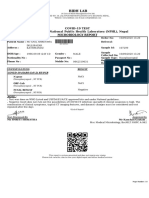
- Covid-19 Test Authorized by National Public Health Laboratory (NPHL), Nepal Microbiology ReportDocument1 pageCovid-19 Test Authorized by National Public Health Laboratory (NPHL), Nepal Microbiology ReportAnil ShresthaNo ratings yet
- 3i T3 Implant Surgical Manual - CATMT3 - ENDocument67 pages3i T3 Implant Surgical Manual - CATMT3 - ENSalem RawashdahNo ratings yet
- Enrichment Activities C1: Grade Level: Six Quarter: First Subject: MAPEH-HealthDocument11 pagesEnrichment Activities C1: Grade Level: Six Quarter: First Subject: MAPEH-HealthARLENE MARASIGAN100% (1)
- LDN Information (2!19!17 Update)Document18 pagesLDN Information (2!19!17 Update)bktango100% (1)
- ASPEN Critical Care - Susan BrantleyDocument44 pagesASPEN Critical Care - Susan BrantleyVitoria SilvaNo ratings yet
- Thyroid DisorderDocument19 pagesThyroid DisorderBudi AthAnza SuhartonoNo ratings yet
- Art of Case Taking by Pierre SchmidtDocument18 pagesArt of Case Taking by Pierre SchmidtDr. Debprasad Das100% (1)
- Certificate of Accuracy For "HIV" Antibody TestingDocument2 pagesCertificate of Accuracy For "HIV" Antibody Testingtomasbrewster2409No ratings yet
- Eyehance MTFDocument6 pagesEyehance MTFanandprasad244No ratings yet
- Bachelor of Science in Nursing: Care of Mother and Child and AdolescentDocument12 pagesBachelor of Science in Nursing: Care of Mother and Child and AdolescentJaja ManezNo ratings yet
- Naija Docs Magazine Issue 6Document46 pagesNaija Docs Magazine Issue 6Olumide ElebuteNo ratings yet
- Oncology Revision: Paul BaillieDocument299 pagesOncology Revision: Paul BaillieMourian AmanNo ratings yet
- Alzheimer WorksheetDocument3 pagesAlzheimer WorksheetRoberto Queiroz GomesNo ratings yet
- (50 Studies Every Doctor Should Know (Series)) Ashaunta T. Anderson, Nina L. Shapiro, Stephen C. Aronoff, Jeremiah Davis, Michael Levy, Michael E. Hochman-50 Studies Every Pediatrician Should Know-OxfDocument361 pages(50 Studies Every Doctor Should Know (Series)) Ashaunta T. Anderson, Nina L. Shapiro, Stephen C. Aronoff, Jeremiah Davis, Michael Levy, Michael E. Hochman-50 Studies Every Pediatrician Should Know-OxfMarcos R Galvão BatistaNo ratings yet
- Preservatives Used in Eye Drops: Paytaxt Private Institute Pharmacy Department 1 StageDocument7 pagesPreservatives Used in Eye Drops: Paytaxt Private Institute Pharmacy Department 1 StageShakar Ezaddin AbdullahNo ratings yet
- Langdon, Helen (20 06 22)Document2 pagesLangdon, Helen (20 06 22)helen langdonNo ratings yet
- History of Present IllnessDocument4 pagesHistory of Present Illnessegabe386No ratings yet
- Diagnostic LaparosDocument11 pagesDiagnostic LaparosDr-Shadi MeteirNo ratings yet
- Activity Based Risk Assessment: Batamindo Industrial ParkDocument6 pagesActivity Based Risk Assessment: Batamindo Industrial ParkEko Gede SeptandhoNo ratings yet
- Lecture - 6-7 - Chronic Apical Periodontitis. Clinical Signs, Diagnostic MethodsDocument40 pagesLecture - 6-7 - Chronic Apical Periodontitis. Clinical Signs, Diagnostic MethodsA.J. YounesNo ratings yet
- Ipgme&r Opd ScheduleDocument8 pagesIpgme&r Opd Schedulean o nymousNo ratings yet
- Osteopathic Treatment in Equestrian SportDocument6 pagesOsteopathic Treatment in Equestrian SportSam LoretNo ratings yet
- Abdominal MassDocument7 pagesAbdominal MassRoseben SomidoNo ratings yet
- Stok Opname: Tablet No Nama Obat SisaDocument7 pagesStok Opname: Tablet No Nama Obat SisajuleNo ratings yet
- Endocrinology 2Document108 pagesEndocrinology 2moad kiNo ratings yet