
Hiv Aids Status Disclosure Increases Support Behavioural Change and Hiv Prevention in The Long Term A Case For An Urban Clinic Kampala Uganda
Hiv Aids Status Disclosure Increases Support Behavioural Change and Hiv Prevention in The Long Term A Case For An Urban Clinic Kampala Uganda
You might also like
- Jakki Mohr, Sanjit Sengupta, Stanley Slater Marketing of High-Technology Products and InnovationsDocument569 pagesJakki Mohr, Sanjit Sengupta, Stanley Slater Marketing of High-Technology Products and InnovationsArshed Rosales100% (3)
- (Get Now) SOAP For Family Medicine by Daniel Maldonado: Â Š PDF Â Š KINDLE Â ŠDocument12 pages(Get Now) SOAP For Family Medicine by Daniel Maldonado: Â Š PDF Â Š KINDLE Â ŠMauricio Solano DiazNo ratings yet
- Corrective Math Common ProblemsDocument6 pagesCorrective Math Common ProblemsmissfhNo ratings yet
- Ramniranjan Jhunjhunwala College of Arts, Science and Commerce (Autonomous)Document1 pageRamniranjan Jhunjhunwala College of Arts, Science and Commerce (Autonomous)Angelina JoyNo ratings yet
- UniverseDocument117 pagesUniverseremow75% (8)
- Bus 100 Final & Answers 07Document24 pagesBus 100 Final & Answers 07Larry McGeeNo ratings yet
- Methodical Series Tests For Fuller Ship Hull Forms: Ocean EngngDocument48 pagesMethodical Series Tests For Fuller Ship Hull Forms: Ocean EngngEdson SerejoNo ratings yet
- Sample Road Design ReportDocument77 pagesSample Road Design ReportKwaku frimpongNo ratings yet
- Reasons For Disclosure of HIV Status by People Living With HIV/AIDS and in HIV Care in Uganda: An Exploratory StudyDocument9 pagesReasons For Disclosure of HIV Status by People Living With HIV/AIDS and in HIV Care in Uganda: An Exploratory StudyJessieRealistaNo ratings yet
- 299 ArabicDocument9 pages299 ArabicTinkhaniMbichilaNo ratings yet
- Sample of Research Paper About AidsDocument7 pagesSample of Research Paper About Aidsaflefvsva100% (1)
- Blocking The Benefit of Group Based HIV Prevention Efforts During Adolescence - StigmaDocument8 pagesBlocking The Benefit of Group Based HIV Prevention Efforts During Adolescence - StigmaAMALIA PEBRIYANTINo ratings yet
- Perceptions About Sexual Abstinence and Knowledge of HIV/AIDS Prevention Among In-School Adolescents in A Western Nigerian CityDocument10 pagesPerceptions About Sexual Abstinence and Knowledge of HIV/AIDS Prevention Among In-School Adolescents in A Western Nigerian CityСалов ЕгорNo ratings yet
- Literature Review Hiv StigmaDocument4 pagesLiterature Review Hiv Stigmaafmzfgmwuzncdj100% (1)
- VIH/SIDA - RevelacaoDocument7 pagesVIH/SIDA - Revelacaovanessa waltersNo ratings yet
- Example of Research Paper About AidsDocument7 pagesExample of Research Paper About Aidsgvym06g6100% (1)
- Sang 2018Document8 pagesSang 2018bernardodelvientoNo ratings yet
- Research Paper On Aids PDFDocument5 pagesResearch Paper On Aids PDFm1dyhuh1jud2100% (1)
- Hiv Prevention Literature ReviewDocument9 pagesHiv Prevention Literature Reviewafmzatvuipwdal100% (1)
- HolaaaaaDocument5 pagesHolaaaaaAlejandro Molina MedinaNo ratings yet
- Original Paper: Electronic Supplementary MaterialDocument14 pagesOriginal Paper: Electronic Supplementary MaterialRiska Resty WasitaNo ratings yet
- Literature Review On Hiv InfectionDocument7 pagesLiterature Review On Hiv Infectionafdtunqho100% (1)
- Primary HIV Infection: Knowledge Amongst Gay Men: Report: July 2011Document15 pagesPrimary HIV Infection: Knowledge Amongst Gay Men: Report: July 2011api-26601760No ratings yet
- Research Paper Topics About HivDocument8 pagesResearch Paper Topics About Hivlrqylwznd100% (1)
- Zero Feet Away: Perspective On HIV/AIDS and Unprotected Sex in Men Who Have Sex With Men Utilizing Location-Based Mobile AppsDocument2 pagesZero Feet Away: Perspective On HIV/AIDS and Unprotected Sex in Men Who Have Sex With Men Utilizing Location-Based Mobile AppsSergio Nahuel CandidoNo ratings yet
- Factors Influencing HIV Disclosure Among People Living With HIV/AIDS in Nigeria: A Systematic Review Using Narrative Synthesis and Meta-AnalysisDocument16 pagesFactors Influencing HIV Disclosure Among People Living With HIV/AIDS in Nigeria: A Systematic Review Using Narrative Synthesis and Meta-AnalysisTrisna SariNo ratings yet
- Hiv Aids Thesis TopicsDocument5 pagesHiv Aids Thesis TopicsCollegePapersHelpSingapore100% (1)
- Brener 2013Document4 pagesBrener 2013Paul Ávila VanegasNo ratings yet
- Public Health - Vol 2 - Issue 4 - Article 5Document44 pagesPublic Health - Vol 2 - Issue 4 - Article 5kaisamerno2003No ratings yet
- Research Paper On Hiv Aids PDFDocument6 pagesResearch Paper On Hiv Aids PDFafnhbijlzdufjj100% (1)
- Ias 16 4 18749Document7 pagesIas 16 4 18749Amos AprekuNo ratings yet
- HIV Exposure in The U.S and South Africa: Sabrina C, Helen R, Francisco MDocument10 pagesHIV Exposure in The U.S and South Africa: Sabrina C, Helen R, Francisco Mapi-624293067No ratings yet
- Initiation of ARV Treatment Protects Uninfected Sexual Partners From HIV (HPTN Study 052)Document2 pagesInitiation of ARV Treatment Protects Uninfected Sexual Partners From HIV (HPTN Study 052)Laura Lopez GonzalezNo ratings yet
- Research PaperDocument13 pagesResearch PaperKelly AlmadrigoNo ratings yet
- Thesis On Hiv Aids in IndiaDocument8 pagesThesis On Hiv Aids in IndiaBuyLiteratureReviewPaperSingapore100% (2)
- The Family and Hiv TodayDocument6 pagesThe Family and Hiv TodaykarunnalNo ratings yet
- Literature Review Hiv AidsDocument7 pagesLiterature Review Hiv Aidsfvga1ym2100% (1)
- Methods 508Document2 pagesMethods 508Nurul MazniNo ratings yet
- Super Final Output (For Hardbound)Document108 pagesSuper Final Output (For Hardbound)Melody Kaye MonsantoNo ratings yet
- Factors Impacting Antiretroviral Therapy Adherence Among Human Immunodeficiency Virus-Positive Adolescents in Sub-Saharan AfricaDocument12 pagesFactors Impacting Antiretroviral Therapy Adherence Among Human Immunodeficiency Virus-Positive Adolescents in Sub-Saharan AfricaDouglas ChukwuNo ratings yet
- Free Research Papers On Hiv AidsDocument8 pagesFree Research Papers On Hiv Aidsorlfgcvkg100% (1)
- Dissertation On Hiv PreventionDocument5 pagesDissertation On Hiv PreventionPaySomeoneToWritePaperManchester100% (1)
- Introduction To HIV PreventionDocument23 pagesIntroduction To HIV Preventionvgv1976No ratings yet
- Months After Licensure Human Papillomavirus Vaccination Practices: A Survey of US Physicians 18Document11 pagesMonths After Licensure Human Papillomavirus Vaccination Practices: A Survey of US Physicians 18api-30279712No ratings yet
- Social Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsFrom EverandSocial Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsNo ratings yet
- Gender Inequality in Hiv: Prevention Now, Programme Briefs, No. 4. 2002 UNFPADocument5 pagesGender Inequality in Hiv: Prevention Now, Programme Briefs, No. 4. 2002 UNFPAPerkymeNo ratings yet
- AidspaperfinalDocument11 pagesAidspaperfinalapi-356346513No ratings yet
- StigmaDocument12 pagesStigmaSheyla CanizalesNo ratings yet
- Internalized HIV AIDS Related Stigma inDocument9 pagesInternalized HIV AIDS Related Stigma inABBA MALLANo ratings yet
- Hiv-Aids Research Paper-1Document9 pagesHiv-Aids Research Paper-1api-449156426No ratings yet
- 06 StiDocument5 pages06 StiJayson TrajanoNo ratings yet
- Hiv CounselingDocument7 pagesHiv CounselingUmar IsaNo ratings yet
- Navigating Disclosure Obstacles Encountered by Individuals With HIV at Kakomo Healing Centre IV in Kabale DistrictDocument15 pagesNavigating Disclosure Obstacles Encountered by Individuals With HIV at Kakomo Healing Centre IV in Kabale DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Lorms Health and DiseasesDocument3 pagesLorms Health and Diseasessarahsze6No ratings yet
- Stigma and Discrimination-HIV and Aids Context: (A Case Study of University CommunityDocument9 pagesStigma and Discrimination-HIV and Aids Context: (A Case Study of University CommunityJASH MATHEWNo ratings yet
- Name: Agun Fauji Nim: P1337420214014 Class: 2BDocument2 pagesName: Agun Fauji Nim: P1337420214014 Class: 2BRijal MulyadinataNo ratings yet
- A Study of Stigma and Discrimination Towards People Living With Hiv/AidsDocument20 pagesA Study of Stigma and Discrimination Towards People Living With Hiv/Aidsmusamuwaga100% (1)
- Research Paper About Aids in AfricaDocument13 pagesResearch Paper About Aids in Africafzg9e1r9100% (1)
- HIV / AIDS: Social and Ethical Issues: EditorialDocument2 pagesHIV / AIDS: Social and Ethical Issues: EditorialventyNo ratings yet
- The Demand For, and Impact Of, Learning HIV Status: by Rebecca L. ThorntonDocument35 pagesThe Demand For, and Impact Of, Learning HIV Status: by Rebecca L. ThorntonFernanda CáceresNo ratings yet
- Rapid Routine Hiv Testing For Psychiatric Inpatients 2155 6113 1000555Document5 pagesRapid Routine Hiv Testing For Psychiatric Inpatients 2155 6113 1000555Elisa BaronNo ratings yet
- Research Paper Topics On Aids in AfricaDocument5 pagesResearch Paper Topics On Aids in Africapukytij0wyg3100% (1)
- CITRADocument9 pagesCITRAAchriani AsraNo ratings yet
- Treatment Adherence in HIV Stigmatized Environments in South Africa: Stigma Avoidance and Medication ManagementDocument9 pagesTreatment Adherence in HIV Stigmatized Environments in South Africa: Stigma Avoidance and Medication ManagementLeonardo RivagorzaNo ratings yet
- Hiv Aids Research Paper PDFDocument9 pagesHiv Aids Research Paper PDFcan3z5gx100% (1)
- Attitudes Towards Mental Illness in Malawi: A Cross-Sectional SurveyDocument6 pagesAttitudes Towards Mental Illness in Malawi: A Cross-Sectional SurveyAdina OlteanuNo ratings yet
- Barriers To Early Treatment Seeking Among Patients With Sexually Transmitted Infections in A Rural Community Setting at Kaproron Health Centre IVDocument15 pagesBarriers To Early Treatment Seeking Among Patients With Sexually Transmitted Infections in A Rural Community Setting at Kaproron Health Centre IVKIU PUBLICATION AND EXTENSIONNo ratings yet
- 3134478Document4 pages3134478Intan WidyawatiNo ratings yet
- Relational Model ConceptsDocument5 pagesRelational Model ConceptsAbhinandan BhatNo ratings yet
- WEG cfw501 Programming Manual 10002391560 1.8x Manual EnglishDocument192 pagesWEG cfw501 Programming Manual 10002391560 1.8x Manual EnglishLeandro RochaNo ratings yet
- FURUNO FAR-FR2855 Installation Manual RDP115 Basic DiagramsDocument86 pagesFURUNO FAR-FR2855 Installation Manual RDP115 Basic Diagramstoumassis_pNo ratings yet
- Canal SystemsDocument69 pagesCanal SystemsAnter TsatseNo ratings yet
- Basic Hydrocyclone OperationDocument23 pagesBasic Hydrocyclone Operationgeo rayfandyNo ratings yet
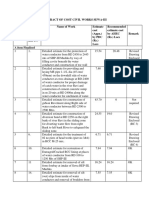
- Abstract of Cost Civil Works SewaDocument3 pagesAbstract of Cost Civil Works SewaPrabhat MicNo ratings yet
- Earthing SystemDocument10 pagesEarthing SystemnishanthaindikaNo ratings yet
- Design of Basic ComputerDocument29 pagesDesign of Basic ComputerM DEEPANANo ratings yet
- General Studies Class 12Document6 pagesGeneral Studies Class 12rpcoolrahul73100% (1)
- Department of Master of Computer Application: M.C.A. First Year (II Semester)Document7 pagesDepartment of Master of Computer Application: M.C.A. First Year (II Semester)Roshan ChandekarNo ratings yet
- Connecting With Your ValuesDocument3 pagesConnecting With Your ValuesNishant AnandNo ratings yet
- DLL Grade 4 Q3 W2Document4 pagesDLL Grade 4 Q3 W2Floy ClarinNo ratings yet
- Cyrillan Project Final ReportDocument28 pagesCyrillan Project Final ReportDat Nguyen ThanhNo ratings yet
- NOTE - Elevator Controls - ManualzzDocument107 pagesNOTE - Elevator Controls - ManualzzFrancisco Javier BurgosNo ratings yet
- Mode of Failure FoundationDocument11 pagesMode of Failure FoundationFirash ImranNo ratings yet
- Fukuoka - Serene Green Roof of JapanDocument7 pagesFukuoka - Serene Green Roof of JapanJo ChanNo ratings yet
- Microeconomics Question Set 4 (20231107) AnswerkeyDocument9 pagesMicroeconomics Question Set 4 (20231107) AnswerkeyMegumi TsuchiyaNo ratings yet
- Tech Gr9 m3 Hydraulic Pneumatic SystemsDocument26 pagesTech Gr9 m3 Hydraulic Pneumatic SystemsEduBoard100% (1)
- Liebherr Vehicle CardDocument16 pagesLiebherr Vehicle CardArimbi GembiekNo ratings yet
- G7M-1131-00 - OFF-LINE MAINTENANCE PROCEDURE FOR MORE THAN 1kV CIRCUIT BREAKERSDocument9 pagesG7M-1131-00 - OFF-LINE MAINTENANCE PROCEDURE FOR MORE THAN 1kV CIRCUIT BREAKERSMohammad QureshiNo ratings yet
- VDB3722MA Driver With Microstep Série NovaDocument16 pagesVDB3722MA Driver With Microstep Série NovaJefferson Alcantara GomesNo ratings yet
























































































Download as pdf or txt
You might also like
- Jakki Mohr, Sanjit Sengupta, Stanley Slater Marketing of High-Technology Products and InnovationsDocument569 pagesJakki Mohr, Sanjit Sengupta, Stanley Slater Marketing of High-Technology Products and InnovationsArshed Rosales100% (3)
- (Get Now) SOAP For Family Medicine by Daniel Maldonado: Â Š PDF Â Š KINDLE Â ŠDocument12 pages(Get Now) SOAP For Family Medicine by Daniel Maldonado: Â Š PDF Â Š KINDLE Â ŠMauricio Solano DiazNo ratings yet
- Corrective Math Common ProblemsDocument6 pagesCorrective Math Common ProblemsmissfhNo ratings yet
- Ramniranjan Jhunjhunwala College of Arts, Science and Commerce (Autonomous)Document1 pageRamniranjan Jhunjhunwala College of Arts, Science and Commerce (Autonomous)Angelina JoyNo ratings yet
- UniverseDocument117 pagesUniverseremow75% (8)
- Bus 100 Final & Answers 07Document24 pagesBus 100 Final & Answers 07Larry McGeeNo ratings yet
- Methodical Series Tests For Fuller Ship Hull Forms: Ocean EngngDocument48 pagesMethodical Series Tests For Fuller Ship Hull Forms: Ocean EngngEdson SerejoNo ratings yet
- Sample Road Design ReportDocument77 pagesSample Road Design ReportKwaku frimpongNo ratings yet
- Reasons For Disclosure of HIV Status by People Living With HIV/AIDS and in HIV Care in Uganda: An Exploratory StudyDocument9 pagesReasons For Disclosure of HIV Status by People Living With HIV/AIDS and in HIV Care in Uganda: An Exploratory StudyJessieRealistaNo ratings yet
- 299 ArabicDocument9 pages299 ArabicTinkhaniMbichilaNo ratings yet
- Sample of Research Paper About AidsDocument7 pagesSample of Research Paper About Aidsaflefvsva100% (1)
- Blocking The Benefit of Group Based HIV Prevention Efforts During Adolescence - StigmaDocument8 pagesBlocking The Benefit of Group Based HIV Prevention Efforts During Adolescence - StigmaAMALIA PEBRIYANTINo ratings yet
- Perceptions About Sexual Abstinence and Knowledge of HIV/AIDS Prevention Among In-School Adolescents in A Western Nigerian CityDocument10 pagesPerceptions About Sexual Abstinence and Knowledge of HIV/AIDS Prevention Among In-School Adolescents in A Western Nigerian CityСалов ЕгорNo ratings yet
- Literature Review Hiv StigmaDocument4 pagesLiterature Review Hiv Stigmaafmzfgmwuzncdj100% (1)
- VIH/SIDA - RevelacaoDocument7 pagesVIH/SIDA - Revelacaovanessa waltersNo ratings yet
- Example of Research Paper About AidsDocument7 pagesExample of Research Paper About Aidsgvym06g6100% (1)
- Sang 2018Document8 pagesSang 2018bernardodelvientoNo ratings yet
- Research Paper On Aids PDFDocument5 pagesResearch Paper On Aids PDFm1dyhuh1jud2100% (1)
- Hiv Prevention Literature ReviewDocument9 pagesHiv Prevention Literature Reviewafmzatvuipwdal100% (1)
- HolaaaaaDocument5 pagesHolaaaaaAlejandro Molina MedinaNo ratings yet
- Original Paper: Electronic Supplementary MaterialDocument14 pagesOriginal Paper: Electronic Supplementary MaterialRiska Resty WasitaNo ratings yet
- Literature Review On Hiv InfectionDocument7 pagesLiterature Review On Hiv Infectionafdtunqho100% (1)
- Primary HIV Infection: Knowledge Amongst Gay Men: Report: July 2011Document15 pagesPrimary HIV Infection: Knowledge Amongst Gay Men: Report: July 2011api-26601760No ratings yet
- Research Paper Topics About HivDocument8 pagesResearch Paper Topics About Hivlrqylwznd100% (1)
- Zero Feet Away: Perspective On HIV/AIDS and Unprotected Sex in Men Who Have Sex With Men Utilizing Location-Based Mobile AppsDocument2 pagesZero Feet Away: Perspective On HIV/AIDS and Unprotected Sex in Men Who Have Sex With Men Utilizing Location-Based Mobile AppsSergio Nahuel CandidoNo ratings yet
- Factors Influencing HIV Disclosure Among People Living With HIV/AIDS in Nigeria: A Systematic Review Using Narrative Synthesis and Meta-AnalysisDocument16 pagesFactors Influencing HIV Disclosure Among People Living With HIV/AIDS in Nigeria: A Systematic Review Using Narrative Synthesis and Meta-AnalysisTrisna SariNo ratings yet
- Hiv Aids Thesis TopicsDocument5 pagesHiv Aids Thesis TopicsCollegePapersHelpSingapore100% (1)
- Brener 2013Document4 pagesBrener 2013Paul Ávila VanegasNo ratings yet
- Public Health - Vol 2 - Issue 4 - Article 5Document44 pagesPublic Health - Vol 2 - Issue 4 - Article 5kaisamerno2003No ratings yet
- Research Paper On Hiv Aids PDFDocument6 pagesResearch Paper On Hiv Aids PDFafnhbijlzdufjj100% (1)
- Ias 16 4 18749Document7 pagesIas 16 4 18749Amos AprekuNo ratings yet
- HIV Exposure in The U.S and South Africa: Sabrina C, Helen R, Francisco MDocument10 pagesHIV Exposure in The U.S and South Africa: Sabrina C, Helen R, Francisco Mapi-624293067No ratings yet
- Initiation of ARV Treatment Protects Uninfected Sexual Partners From HIV (HPTN Study 052)Document2 pagesInitiation of ARV Treatment Protects Uninfected Sexual Partners From HIV (HPTN Study 052)Laura Lopez GonzalezNo ratings yet
- Research PaperDocument13 pagesResearch PaperKelly AlmadrigoNo ratings yet
- Thesis On Hiv Aids in IndiaDocument8 pagesThesis On Hiv Aids in IndiaBuyLiteratureReviewPaperSingapore100% (2)
- The Family and Hiv TodayDocument6 pagesThe Family and Hiv TodaykarunnalNo ratings yet
- Literature Review Hiv AidsDocument7 pagesLiterature Review Hiv Aidsfvga1ym2100% (1)
- Methods 508Document2 pagesMethods 508Nurul MazniNo ratings yet
- Super Final Output (For Hardbound)Document108 pagesSuper Final Output (For Hardbound)Melody Kaye MonsantoNo ratings yet
- Factors Impacting Antiretroviral Therapy Adherence Among Human Immunodeficiency Virus-Positive Adolescents in Sub-Saharan AfricaDocument12 pagesFactors Impacting Antiretroviral Therapy Adherence Among Human Immunodeficiency Virus-Positive Adolescents in Sub-Saharan AfricaDouglas ChukwuNo ratings yet
- Free Research Papers On Hiv AidsDocument8 pagesFree Research Papers On Hiv Aidsorlfgcvkg100% (1)
- Dissertation On Hiv PreventionDocument5 pagesDissertation On Hiv PreventionPaySomeoneToWritePaperManchester100% (1)
- Introduction To HIV PreventionDocument23 pagesIntroduction To HIV Preventionvgv1976No ratings yet
- Months After Licensure Human Papillomavirus Vaccination Practices: A Survey of US Physicians 18Document11 pagesMonths After Licensure Human Papillomavirus Vaccination Practices: A Survey of US Physicians 18api-30279712No ratings yet
- Social Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsFrom EverandSocial Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsNo ratings yet
- Gender Inequality in Hiv: Prevention Now, Programme Briefs, No. 4. 2002 UNFPADocument5 pagesGender Inequality in Hiv: Prevention Now, Programme Briefs, No. 4. 2002 UNFPAPerkymeNo ratings yet
- AidspaperfinalDocument11 pagesAidspaperfinalapi-356346513No ratings yet
- StigmaDocument12 pagesStigmaSheyla CanizalesNo ratings yet
- Internalized HIV AIDS Related Stigma inDocument9 pagesInternalized HIV AIDS Related Stigma inABBA MALLANo ratings yet
- Hiv-Aids Research Paper-1Document9 pagesHiv-Aids Research Paper-1api-449156426No ratings yet
- 06 StiDocument5 pages06 StiJayson TrajanoNo ratings yet
- Hiv CounselingDocument7 pagesHiv CounselingUmar IsaNo ratings yet
- Navigating Disclosure Obstacles Encountered by Individuals With HIV at Kakomo Healing Centre IV in Kabale DistrictDocument15 pagesNavigating Disclosure Obstacles Encountered by Individuals With HIV at Kakomo Healing Centre IV in Kabale DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Lorms Health and DiseasesDocument3 pagesLorms Health and Diseasessarahsze6No ratings yet
- Stigma and Discrimination-HIV and Aids Context: (A Case Study of University CommunityDocument9 pagesStigma and Discrimination-HIV and Aids Context: (A Case Study of University CommunityJASH MATHEWNo ratings yet
- Name: Agun Fauji Nim: P1337420214014 Class: 2BDocument2 pagesName: Agun Fauji Nim: P1337420214014 Class: 2BRijal MulyadinataNo ratings yet
- A Study of Stigma and Discrimination Towards People Living With Hiv/AidsDocument20 pagesA Study of Stigma and Discrimination Towards People Living With Hiv/Aidsmusamuwaga100% (1)
- Research Paper About Aids in AfricaDocument13 pagesResearch Paper About Aids in Africafzg9e1r9100% (1)
- HIV / AIDS: Social and Ethical Issues: EditorialDocument2 pagesHIV / AIDS: Social and Ethical Issues: EditorialventyNo ratings yet
- The Demand For, and Impact Of, Learning HIV Status: by Rebecca L. ThorntonDocument35 pagesThe Demand For, and Impact Of, Learning HIV Status: by Rebecca L. ThorntonFernanda CáceresNo ratings yet
- Rapid Routine Hiv Testing For Psychiatric Inpatients 2155 6113 1000555Document5 pagesRapid Routine Hiv Testing For Psychiatric Inpatients 2155 6113 1000555Elisa BaronNo ratings yet
- Research Paper Topics On Aids in AfricaDocument5 pagesResearch Paper Topics On Aids in Africapukytij0wyg3100% (1)
- CITRADocument9 pagesCITRAAchriani AsraNo ratings yet
- Treatment Adherence in HIV Stigmatized Environments in South Africa: Stigma Avoidance and Medication ManagementDocument9 pagesTreatment Adherence in HIV Stigmatized Environments in South Africa: Stigma Avoidance and Medication ManagementLeonardo RivagorzaNo ratings yet
- Hiv Aids Research Paper PDFDocument9 pagesHiv Aids Research Paper PDFcan3z5gx100% (1)
- Attitudes Towards Mental Illness in Malawi: A Cross-Sectional SurveyDocument6 pagesAttitudes Towards Mental Illness in Malawi: A Cross-Sectional SurveyAdina OlteanuNo ratings yet
- Barriers To Early Treatment Seeking Among Patients With Sexually Transmitted Infections in A Rural Community Setting at Kaproron Health Centre IVDocument15 pagesBarriers To Early Treatment Seeking Among Patients With Sexually Transmitted Infections in A Rural Community Setting at Kaproron Health Centre IVKIU PUBLICATION AND EXTENSIONNo ratings yet
- 3134478Document4 pages3134478Intan WidyawatiNo ratings yet
- Relational Model ConceptsDocument5 pagesRelational Model ConceptsAbhinandan BhatNo ratings yet
- WEG cfw501 Programming Manual 10002391560 1.8x Manual EnglishDocument192 pagesWEG cfw501 Programming Manual 10002391560 1.8x Manual EnglishLeandro RochaNo ratings yet
- FURUNO FAR-FR2855 Installation Manual RDP115 Basic DiagramsDocument86 pagesFURUNO FAR-FR2855 Installation Manual RDP115 Basic Diagramstoumassis_pNo ratings yet
- Canal SystemsDocument69 pagesCanal SystemsAnter TsatseNo ratings yet
- Basic Hydrocyclone OperationDocument23 pagesBasic Hydrocyclone Operationgeo rayfandyNo ratings yet
- Abstract of Cost Civil Works SewaDocument3 pagesAbstract of Cost Civil Works SewaPrabhat MicNo ratings yet
- Earthing SystemDocument10 pagesEarthing SystemnishanthaindikaNo ratings yet
- Design of Basic ComputerDocument29 pagesDesign of Basic ComputerM DEEPANANo ratings yet
- General Studies Class 12Document6 pagesGeneral Studies Class 12rpcoolrahul73100% (1)
- Department of Master of Computer Application: M.C.A. First Year (II Semester)Document7 pagesDepartment of Master of Computer Application: M.C.A. First Year (II Semester)Roshan ChandekarNo ratings yet
- Connecting With Your ValuesDocument3 pagesConnecting With Your ValuesNishant AnandNo ratings yet
- DLL Grade 4 Q3 W2Document4 pagesDLL Grade 4 Q3 W2Floy ClarinNo ratings yet
- Cyrillan Project Final ReportDocument28 pagesCyrillan Project Final ReportDat Nguyen ThanhNo ratings yet
- NOTE - Elevator Controls - ManualzzDocument107 pagesNOTE - Elevator Controls - ManualzzFrancisco Javier BurgosNo ratings yet
- Mode of Failure FoundationDocument11 pagesMode of Failure FoundationFirash ImranNo ratings yet
- Fukuoka - Serene Green Roof of JapanDocument7 pagesFukuoka - Serene Green Roof of JapanJo ChanNo ratings yet
- Microeconomics Question Set 4 (20231107) AnswerkeyDocument9 pagesMicroeconomics Question Set 4 (20231107) AnswerkeyMegumi TsuchiyaNo ratings yet
- Tech Gr9 m3 Hydraulic Pneumatic SystemsDocument26 pagesTech Gr9 m3 Hydraulic Pneumatic SystemsEduBoard100% (1)
- Liebherr Vehicle CardDocument16 pagesLiebherr Vehicle CardArimbi GembiekNo ratings yet
- G7M-1131-00 - OFF-LINE MAINTENANCE PROCEDURE FOR MORE THAN 1kV CIRCUIT BREAKERSDocument9 pagesG7M-1131-00 - OFF-LINE MAINTENANCE PROCEDURE FOR MORE THAN 1kV CIRCUIT BREAKERSMohammad QureshiNo ratings yet
- VDB3722MA Driver With Microstep Série NovaDocument16 pagesVDB3722MA Driver With Microstep Série NovaJefferson Alcantara GomesNo ratings yet