Download as pdf or txt
You might also like
- Exercise Prescription and ManagementDocument6 pagesExercise Prescription and ManagementSittie Aisah AmpatuaNo ratings yet
- Exercise Testing and Prescription in Older AdultsDocument19 pagesExercise Testing and Prescription in Older Adultspushplata.19770No ratings yet
- ACSMGuidelines UNMDocument6 pagesACSMGuidelines UNMWagner PereiraNo ratings yet
- Articulo 1Document7 pagesArticulo 1Maria Valentina Rodriguez DiazNo ratings yet
- Effects of Resistance Training On Functional Strength and MuscleDocument7 pagesEffects of Resistance Training On Functional Strength and MuscleDianne PenagosNo ratings yet
- Prescription of Resistance Training For Healthy PopulationsDocument12 pagesPrescription of Resistance Training For Healthy PopulationsInglês The Right WayNo ratings yet
- Pulmonary Rehabilitation Resources in A Complex and Rapidly Changing World-American Thoracic SocietyDocument4 pagesPulmonary Rehabilitation Resources in A Complex and Rapidly Changing World-American Thoracic SocietyGleidys NavarroNo ratings yet
- Progressive Resistive Exercise: Erbil Polytechnic UniversityDocument10 pagesProgressive Resistive Exercise: Erbil Polytechnic UniversityNur DilshadNo ratings yet
- Final ProjectDocument11 pagesFinal Projectapi-283142068No ratings yet
- Pathfit02 Prelims ReviewerDocument3 pagesPathfit02 Prelims ReviewerowenbacatancorporalNo ratings yet
- Manual of Basic Physiotherapeutic Exercises For Family and Caregivers of Stroke PatientsDocument5 pagesManual of Basic Physiotherapeutic Exercises For Family and Caregivers of Stroke PatientsKookie YerimNo ratings yet
- Functional Exercise ProgressionDocument6 pagesFunctional Exercise ProgressionAnastasia Skamagki100% (1)
- Training Effects of Long Versus Short Bouts of Exercise in Healthy Subjects.Document4 pagesTraining Effects of Long Versus Short Bouts of Exercise in Healthy Subjects.HosseinNo ratings yet
- Non-Traditional Exercise Options in The Outpatient Orthopedic SettingDocument16 pagesNon-Traditional Exercise Options in The Outpatient Orthopedic Settingapi-518613757No ratings yet
- Exercise PrescriptionDocument49 pagesExercise PrescriptionLynette Fernandez50% (2)
- Horn WebinarDocument53 pagesHorn WebinarGerr McGregorNo ratings yet
- Exercise Training Based On Individual Physical Fitness and Interval Walking Training To Prevent Lifestyle-Related Diseases in Middle-Aged and Older PeopleDocument7 pagesExercise Training Based On Individual Physical Fitness and Interval Walking Training To Prevent Lifestyle-Related Diseases in Middle-Aged and Older PeopleAris MuhtaromNo ratings yet
- DoctorsHanbook ch14 PDFDocument10 pagesDoctorsHanbook ch14 PDFEdsel JavellanaNo ratings yet
- Fitt 2 Handout 2022 2023Document22 pagesFitt 2 Handout 2022 2023patriciaperenal19No ratings yet
- Articulo Salud PublicaDocument18 pagesArticulo Salud PublicaCatherinne Quiñonez GutierrezNo ratings yet
- Effects of A 12-Week Resistive Training Program in The Home Using The Body Bar On Dynamic and Absolute Strength o F Middle-Age Women 'Document8 pagesEffects of A 12-Week Resistive Training Program in The Home Using The Body Bar On Dynamic and Absolute Strength o F Middle-Age Women 'HosseinNo ratings yet
- Special Pops Supplementary MaterialDocument6 pagesSpecial Pops Supplementary MaterialGaby MoraNo ratings yet
- STrength Training PrinciplesDocument31 pagesSTrength Training PrinciplesMai Jewels SagumNo ratings yet
- Water-Versus Land-Based Exercise Effects On Physical Fitness in Older WomenDocument8 pagesWater-Versus Land-Based Exercise Effects On Physical Fitness in Older WomenHONGJY100% (1)
- Predicting Exercise Capacity Through Submaximal Fitness Tests in Persons With Multiple SclerosisDocument8 pagesPredicting Exercise Capacity Through Submaximal Fitness Tests in Persons With Multiple SclerosisNnaemeka NwobodoNo ratings yet
- Fitt 2 Student Handout Ay 2020 2021Document18 pagesFitt 2 Student Handout Ay 2020 2021TRISHA MAE DUMENCELNo ratings yet
- An Introduction To Physical Activity: Study Guide For Module No. 2Document6 pagesAn Introduction To Physical Activity: Study Guide For Module No. 2MC BlancoNo ratings yet
- Kidney Paper 2018Document5 pagesKidney Paper 2018samah hossnyNo ratings yet
- 10 1 1 811 366 PDFDocument7 pages10 1 1 811 366 PDFbookslolNo ratings yet
- Schoenfeld 2015Document9 pagesSchoenfeld 2015GutoGonçalves100% (1)
- Stanton2014 PDFDocument6 pagesStanton2014 PDFPatricio Ávila MuñozNo ratings yet
- A Framework For Exercise Prescription: DOI: 10.1097/TGR.0000000000000011Document23 pagesA Framework For Exercise Prescription: DOI: 10.1097/TGR.0000000000000011Lft Ediel PiñaNo ratings yet
- Fitt 2 HandoutDocument18 pagesFitt 2 Handoutmabangis067No ratings yet
- 7-Progressive Resistance ExerciseDocument64 pages7-Progressive Resistance ExerciseMetin HakkanNo ratings yet
- A Comparison of Community-Based Resistance Exercise and Flexibility Exercise For SeniorsDocument5 pagesA Comparison of Community-Based Resistance Exercise and Flexibility Exercise For SeniorsAlejandraRiveraLondoñoNo ratings yet
- The Stroke Recovery TimelineDocument15 pagesThe Stroke Recovery TimelineLucia NatashaNo ratings yet
- Pe Health 12 Hope 3 q1 Module 3 4Document8 pagesPe Health 12 Hope 3 q1 Module 3 4androgutlay55555No ratings yet
- Exercise Prescription in Primary Care SettingDocument34 pagesExercise Prescription in Primary Care Settingdr.gunturadwiNo ratings yet
- Chap 16. Exercise Prescriptions For Health and FitnessDocument24 pagesChap 16. Exercise Prescriptions For Health and Fitnessghousia shahidNo ratings yet
- Clinical App Worksheet Knee Foot AnkleDocument8 pagesClinical App Worksheet Knee Foot Ankleapi-676469437No ratings yet
- Fitt 2 New Handouts 2023Document11 pagesFitt 2 New Handouts 2023ignaojemarie14No ratings yet
- Endurance, Resistance and Flexibility ExerciseDocument6 pagesEndurance, Resistance and Flexibility ExerciseNicole ReidNo ratings yet
- J Jamda 2019 04 001Document8 pagesJ Jamda 2019 04 001dia putriNo ratings yet
- Seminar OlahragaDocument27 pagesSeminar OlahragaIqlima Khairiyah PutriNo ratings yet
- Exercise Prescription For DisabledDocument51 pagesExercise Prescription For DisabledNaveen KumarNo ratings yet
- Improving Cardiovascular Endurance: Chapter ObjectivesDocument9 pagesImproving Cardiovascular Endurance: Chapter ObjectivesVictor Lopez SueroNo ratings yet
- Basic Concepts in Exercise PhysiologyDocument40 pagesBasic Concepts in Exercise PhysiologyHammad AqibNo ratings yet
- Exercise Guidelines in Pregnancy: New PerspectivesDocument16 pagesExercise Guidelines in Pregnancy: New PerspectivesCarlos VieiraNo ratings yet
- Exercise Therapy AssignmentDocument4 pagesExercise Therapy AssignmentApoorv100% (1)
- Jurnal DiabetesDocument15 pagesJurnal DiabetesJupriadiVillaNo ratings yet
- Full Final ProjectDocument19 pagesFull Final Projectapi-694263947No ratings yet
- Seiler Haugen Kuffel 2007Document8 pagesSeiler Haugen Kuffel 2007luisgarcialcg23No ratings yet
- Fitt 2 ModuleDocument14 pagesFitt 2 ModuleIrish MaeNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) and ExerciseDocument2 pagesChronic Obstructive Pulmonary Disease (COPD) and ExerciseHONGJYNo ratings yet
- Effects of 8 Weeks Equal-Volume Resistance TrainingDocument7 pagesEffects of 8 Weeks Equal-Volume Resistance TrainingChimpompumNo ratings yet
- Exercose Prescription To Reverse FrailtyDocument5 pagesExercose Prescription To Reverse FrailtyMWANKUO KANUNo ratings yet
- The Influence of Direct SupervisionDocument10 pagesThe Influence of Direct SupervisionKennedyOliverNo ratings yet
- CFS 738 WDocument17 pagesCFS 738 WKenneth YapNo ratings yet
- Actividad Fisica de Alta IntensidadDocument10 pagesActividad Fisica de Alta IntensidadyatibaduizaNo ratings yet
- Power Flex Stretching - Super Flexibility and Strength for peak performanceFrom EverandPower Flex Stretching - Super Flexibility and Strength for peak performanceRating: 3 out of 5 stars3/5 (3)
- Basic Facts About ESOPs2Document20 pagesBasic Facts About ESOPs2Quant TradingNo ratings yet
- Copper (RJ-45) SFP: Technical SpecificationsDocument1 pageCopper (RJ-45) SFP: Technical SpecificationsDanielLopezNo ratings yet
- Timber GrowthDocument17 pagesTimber GrowthAbdul Sukur Kamsir100% (3)
- Policy Analysis - Train LawDocument6 pagesPolicy Analysis - Train LawJoyce GemNo ratings yet
- Sala Ta Orn Dam Bill of QuantitiesDocument38 pagesSala Ta Orn Dam Bill of QuantitiesSothearaThengNo ratings yet
- Nameplate PDFDocument8 pagesNameplate PDFobida adailehNo ratings yet
- Reimagining Public SafetyDocument1 pageReimagining Public SafetyWAVE 3 NewsNo ratings yet
- Massive Migration From The Steppe SuppleDocument141 pagesMassive Migration From The Steppe SuppleJonNo ratings yet
- Tle CSS Mod5Document2 pagesTle CSS Mod5john kingNo ratings yet
- Missing Women of PartitionDocument30 pagesMissing Women of PartitionSaya Augustin100% (1)
- Vibration Measurement and Analysis of Rotational Machines: at Makstil Hotplate MillDocument4 pagesVibration Measurement and Analysis of Rotational Machines: at Makstil Hotplate MillMarija PetkovskaNo ratings yet
- Final AYSRH Survey Report - AHC Team - 10th Feb 2017Document135 pagesFinal AYSRH Survey Report - AHC Team - 10th Feb 2017Kadokech SebbyNo ratings yet
- Working Principle of Earth Leakage Circuit Breaker (ELCB), RCD PDFDocument6 pagesWorking Principle of Earth Leakage Circuit Breaker (ELCB), RCD PDFjobpei260% (5)
- Layering With Colored PencilsDocument2 pagesLayering With Colored PencilsfrankcarabanoNo ratings yet
- 2022 Children's ReportDocument3 pages2022 Children's ReportMSWD Camiling100% (2)
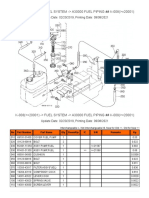
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- Set3 PDFDocument36 pagesSet3 PDFvishwas100% (1)
- Vibrant Yet Under-Resourced: The State of Lesbian, Bisexual, and Queer MovementsDocument44 pagesVibrant Yet Under-Resourced: The State of Lesbian, Bisexual, and Queer MovementsSeres KozmicNo ratings yet
- Case Study Sickle CellDocument2 pagesCase Study Sickle CellAweGooseTreeNo ratings yet
- 2007-Current MaxxForce Engine Breakout Harness Reference (EGES545)Document14 pages2007-Current MaxxForce Engine Breakout Harness Reference (EGES545)Enrrique Lara100% (1)
- Yokogawa RAGN ManualDocument46 pagesYokogawa RAGN ManualJohn AdewaleNo ratings yet
- BM 4 - Bricks & BlocksDocument30 pagesBM 4 - Bricks & BlocksArch Reem AlzyoudNo ratings yet
- Focaccia Bread: IngredientsDocument3 pagesFocaccia Bread: IngredientsJack WillisNo ratings yet
- Vaux CimreplacmentDocument28 pagesVaux CimreplacmentmanutecNo ratings yet
- Cateeeye Speed Breakers and DelineatorsDocument14 pagesCateeeye Speed Breakers and DelineatorsShams KhattakNo ratings yet
- Cells Teachers Guide Discovery EducationDocument38 pagesCells Teachers Guide Discovery EducationKari Kristine Hoskins BarreraNo ratings yet
- Partlist Eq114Document16 pagesPartlist Eq114180976No ratings yet
- Caring For Your African American/Biracial Child's HairDocument32 pagesCaring For Your African American/Biracial Child's Hair4kidslikemeNo ratings yet
- Growth Evaluation and Meat Assessment of Native Pig in Romblon Province, PhilippinesDocument7 pagesGrowth Evaluation and Meat Assessment of Native Pig in Romblon Province, PhilippinesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Prime MX FIRA 6250 2018Document4 pagesPrime MX FIRA 6250 2018hodlab designcoNo ratings yet