Download as pdf or txt
You might also like
- D.O. 221-A - Application Form (New)Document1 pageD.O. 221-A - Application Form (New)Karl Pagz80% (5)
- D.O. 221-A - Application Form (Renewal)Document1 pageD.O. 221-A - Application Form (Renewal)Karl Pagz100% (1)
- Philhealth Online Access Form: Annex ADocument1 pagePhilhealth Online Access Form: Annex ALyyNo ratings yet
- AnnexA POAF PDFDocument1 pageAnnexA POAF PDFjez.lowlifeNo ratings yet
- Philhealth Online Access Form: Annex ADocument1 pagePhilhealth Online Access Form: Annex ACynthia E. Recillo-DayaganonNo ratings yet
- Philhealth Online Access Form: Annex ADocument1 pagePhilhealth Online Access Form: Annex ALyyNo ratings yet
- Poaf 002Document1 pagePoaf 002andrieeya subsNo ratings yet
- Poaf 001 PDFDocument1 pagePoaf 001 PDFTesa GalvezNo ratings yet
- Philhealth Online Access FormDocument1 pagePhilhealth Online Access FormDaisy Ylanan TapaoNo ratings yet
- Philhealth Online Access FormDocument1 pagePhilhealth Online Access FormMa. Lorena MabolocNo ratings yet
- Poaf 001 PDFDocument1 pagePoaf 001 PDFArlyne CreenciaNo ratings yet
- Poaf 001Document1 pagePoaf 001idk.cokNo ratings yet
- Poaf 001 PDFDocument1 pagePoaf 001 PDFTesa GalvezNo ratings yet
- Poaf 001Document1 pagePoaf 001She DNo ratings yet
- OMB Form 2 - Request For Assistance FormDocument1 pageOMB Form 2 - Request For Assistance Formtweety68No ratings yet
- Herf and Ack e KonsultaDocument2 pagesHerf and Ack e KonsultaJanine Constantino CastilloNo ratings yet
- Recruiter Name: Infinite Dragon Life Insurance AgencyDocument17 pagesRecruiter Name: Infinite Dragon Life Insurance Agencybob huli ngalanNo ratings yet
- Desktop Assessment Report: Deemed Not ReadyDocument7 pagesDesktop Assessment Report: Deemed Not ReadyQhsef Karmaveer Jyoteendra VaishnavNo ratings yet
- Personal Account Opening FormDocument4 pagesPersonal Account Opening Formloveleky2No ratings yet
- UAE Bank DocumentsDocument8 pagesUAE Bank DocumentsahmedNo ratings yet
- Philhealth Online Access FormDocument2 pagesPhilhealth Online Access Formallan jhay contaweNo ratings yet
- Eclaims Engagement Form - Annex B - PC 2017-0030 - Rev - 2023Document1 pageEclaims Engagement Form - Annex B - PC 2017-0030 - Rev - 2023Catbalogan Doctors HospitalNo ratings yet
- InnBucks Coperate Account Opening FormDocument12 pagesInnBucks Coperate Account Opening FormkudzaiNo ratings yet
- Philhealth EprsDocument1 pagePhilhealth EprsEqual PrintsNo ratings yet
- POAFDocument1 pagePOAFJune Blossom FernandoNo ratings yet
- New RRF June 2023Document1 pageNew RRF June 2023Jlj ChuaNo ratings yet
- Volunteer Authorisation FormDocument1 pageVolunteer Authorisation Formkhyber khanNo ratings yet
- Freedom of Information Request Form: A. Requesting PartyDocument1 pageFreedom of Information Request Form: A. Requesting PartyLEOPOLDO D VIVERONo ratings yet
- Freedom of Information Request Form: A. Requesting PartyDocument1 pageFreedom of Information Request Form: A. Requesting PartyLEOPOLDO D VIVERONo ratings yet
- Freedom of Information Request Form: A. Requesting PartyDocument1 pageFreedom of Information Request Form: A. Requesting PartyKim FaustinoNo ratings yet
- Freedom of Information Request Form: A. Requesting PartyDocument1 pageFreedom of Information Request Form: A. Requesting PartyLEOPOLDO D VIVERONo ratings yet
- Dormant Activation FormatDocument1 pageDormant Activation FormatBhaumik DaveNo ratings yet
- 1 PHILHEALTH Employer Employee Registration GuideDocument42 pages1 PHILHEALTH Employer Employee Registration GuideRichwell AccountingNo ratings yet
- Authority FormDocument2 pagesAuthority Formrosegr332No ratings yet
- Architects & Engineers Association ThrissurDocument1 pageArchitects & Engineers Association ThrissurStikcon PmcNo ratings yet
- KYC (Know Your Customer) FormDocument2 pagesKYC (Know Your Customer) FormJoseluisNo ratings yet
- Replacement Award ApplicationDocument3 pagesReplacement Award ApplicationPhan-Thanh Bich-HuyenNo ratings yet
- Registration Form: Father/Guardian /spouse DetailsDocument2 pagesRegistration Form: Father/Guardian /spouse Detailspata nahi hai mujeNo ratings yet
- Membership Application FormDocument2 pagesMembership Application Formigga d johnNo ratings yet
- Membership Application Form PDFDocument2 pagesMembership Application Form PDFigga d johnNo ratings yet
- KYC Disclosure FormatDocument1 pageKYC Disclosure FormatBalajiNo ratings yet
- Bcif Front PartnershipDocument1 pageBcif Front PartnershipASDFNo ratings yet
- BCIF - Ver7 With DPA - 02052018 PDFDocument1 pageBCIF - Ver7 With DPA - 02052018 PDFJon Colinares50% (2)
- Egov Account Enrollment FormDocument1 pageEgov Account Enrollment FormEdrick GalangNo ratings yet
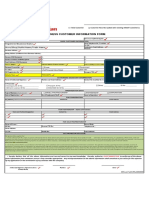
- Business Customer Information Form: Registered Business Name: Store/Shop/Outlet Name/Trade NameDocument3 pagesBusiness Customer Information Form: Registered Business Name: Store/Shop/Outlet Name/Trade NameRodelLaborNo ratings yet
- BCIF - Ver9 With DPA and Bill Delivery Agreement - 02022022Document1 pageBCIF - Ver9 With DPA and Bill Delivery Agreement - 02022022Tegnap Nehj100% (1)
- BCIF Ver9 CorpDocument1 pageBCIF Ver9 Corpher.princelouie100% (1)
- Distriphil Cif FormDocument3 pagesDistriphil Cif Formjimabil ramirezNo ratings yet
- KYC New - DELDocument3 pagesKYC New - DELd13bvenNo ratings yet
- Business Customer Information FormDocument2 pagesBusiness Customer Information FormWalter O BrianNo ratings yet
- Company Subsidized Account/ Sole Proprietorship Company Managed AccountDocument1 pageCompany Subsidized Account/ Sole Proprietorship Company Managed AccountJhello SabinoNo ratings yet
- Loan Agents Information Sheet - New BLANKDocument1 pageLoan Agents Information Sheet - New BLANKBernadette EusteNo ratings yet
- 221 A Application Form NewDocument1 page221 A Application Form NewAaron Chavez0% (1)
- Revised Customer Information Sheet July 2023 1Document1 pageRevised Customer Information Sheet July 2023 1emzthineNo ratings yet
- NEW ACCOUNT - OPENING - FORM - IndiaDocument2 pagesNEW ACCOUNT - OPENING - FORM - IndiaDeepak PanghalNo ratings yet
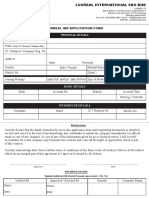
- Luxreal Malaysia Membership FormDocument1 pageLuxreal Malaysia Membership Formkalai arasanNo ratings yet
- Business Customer Information Form: Registered Business Name: Store/Shop/Outlet Name/Trade NameDocument2 pagesBusiness Customer Information Form: Registered Business Name: Store/Shop/Outlet Name/Trade Namelhuk banaag100% (2)
- Global Dominion APPLICATION FORM May 4, 2021Document2 pagesGlobal Dominion APPLICATION FORM May 4, 2021Erwin Dela CruzNo ratings yet
- How To Structure Your Business For Success: Everything You Need To Know To Get Started Building Business CreditFrom EverandHow To Structure Your Business For Success: Everything You Need To Know To Get Started Building Business CreditNo ratings yet