Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- McKinsey Solve Game Ecosystem Building Free Excel TemplateDocument35 pagesMcKinsey Solve Game Ecosystem Building Free Excel TemplatePrakash GiriNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CARIOLOGYDocument77 pagesCARIOLOGYteklay100% (3)
- University of Colorado School of Medicine University of Colorado School of Medicine and Children's Hospital ColoradoDocument2 pagesUniversity of Colorado School of Medicine University of Colorado School of Medicine and Children's Hospital ColoradoashwiniNo ratings yet
- Amniotic Fluid EmbolismDocument22 pagesAmniotic Fluid EmbolismashwiniNo ratings yet
- SWASTHIK - Sale - 13954Document1 pageSWASTHIK - Sale - 13954ashwiniNo ratings yet
- Anatomy and Embryology UterusDocument65 pagesAnatomy and Embryology UterusashwiniNo ratings yet
- 1 s2.0 S1083318820303703Document6 pages1 s2.0 S1083318820303703ashwiniNo ratings yet
- Antepartum Fetal Surveillance Tests and AbnormalityDocument22 pagesAntepartum Fetal Surveillance Tests and AbnormalityashwiniNo ratings yet
- Antepartum Fetal Surveillance - SpoorthiDocument20 pagesAntepartum Fetal Surveillance - SpoorthiashwiniNo ratings yet
- Antepartum HemorrhageDocument43 pagesAntepartum HemorrhageashwiniNo ratings yet
- Discuss The Principles and Complications of The Various Sling Surgeries For Nulliparous Prolapse?Document14 pagesDiscuss The Principles and Complications of The Various Sling Surgeries For Nulliparous Prolapse?ashwiniNo ratings yet
- Review: Zebrafish (Danio Rerio) Sebagai Model Obesitas Dan Diabetes Melitus Tipe 2Document12 pagesReview: Zebrafish (Danio Rerio) Sebagai Model Obesitas Dan Diabetes Melitus Tipe 2GREESTYNo ratings yet
- Ebook Cultural Anthropology Canadian 2Nd Edition Robbins Test Bank Full Chapter PDFDocument34 pagesEbook Cultural Anthropology Canadian 2Nd Edition Robbins Test Bank Full Chapter PDFengagerscotsmangk9jt100% (9)
- Structure and Reproduction of FungiDocument5 pagesStructure and Reproduction of FungiJiyahnBayNo ratings yet
- Sectra Education Portal - EN - Medical SimulatorDocument4 pagesSectra Education Portal - EN - Medical SimulatorPol Enrique Trigoso EchaizNo ratings yet
- Community and Environmental HealthDocument26 pagesCommunity and Environmental HealthMary Grace AgueteNo ratings yet
- Evaluation of The Performance of Sysmex XN-3100 Automated Hematology Analyzer Regarding The Sysmex XE-2100 and Microscopic ExaminationDocument9 pagesEvaluation of The Performance of Sysmex XN-3100 Automated Hematology Analyzer Regarding The Sysmex XE-2100 and Microscopic ExaminationbalkisNo ratings yet
- Insectopia CompendiumDocument53 pagesInsectopia Compendiumnaruto hyuga67% (3)
- 2014 MBAA Chris White Yeast ManagementDocument30 pages2014 MBAA Chris White Yeast ManagementAdrián LampazziNo ratings yet
- Stainning 2019Document29 pagesStainning 2019Almoatazbellah AbdallahNo ratings yet
- Ecosystem Processes Litter Breakdown Patterns in Mediterranean and Black Sea Transitional WatersDocument5 pagesEcosystem Processes Litter Breakdown Patterns in Mediterranean and Black Sea Transitional WaterstrifsilviaNo ratings yet
- BSC Hons Zoology 2016-17 - 23 - 7 - 18Document45 pagesBSC Hons Zoology 2016-17 - 23 - 7 - 18DHUVADU JAGANATHAMNo ratings yet
- Natural Regeneration: Don Minore Robert J. LaackeDocument26 pagesNatural Regeneration: Don Minore Robert J. LaackeAngela Marie AlducenteNo ratings yet
- Psychic DevelopmentDocument13 pagesPsychic DevelopmentCult of Amon Ra100% (2)
- Homeostasis Activity - MARY SHESHIRADocument3 pagesHomeostasis Activity - MARY SHESHIRASheshira Reddy YeruvaNo ratings yet
- Latest Affiliation Rules University of SargodhaDocument10 pagesLatest Affiliation Rules University of SargodhaShahid Ahmed HeeraNo ratings yet
- The History of GarlicDocument1 pageThe History of GarlicZehranur QuliyevaNo ratings yet
- MacMillan Science Library - Animal Sciences Vol. 3 - Hab-PepDocument240 pagesMacMillan Science Library - Animal Sciences Vol. 3 - Hab-PepBLUECOMANCHE50% (2)
- What Has Modern Ecosystem Theory To Offer To Cleaner Production, Industrial Ecology and Society The Views of An EcologistDocument15 pagesWhat Has Modern Ecosystem Theory To Offer To Cleaner Production, Industrial Ecology and Society The Views of An EcologistMilenoNo ratings yet
- Human Health & DiseaseDocument25 pagesHuman Health & DiseaseShiva PrabhakarNo ratings yet
- Pratibha 01 08 2020Document1 pagePratibha 01 08 2020R MedipalliNo ratings yet
- Nanotechnology Optical Tweezers ReportDocument13 pagesNanotechnology Optical Tweezers ReportDaria RomanNo ratings yet
- Case Study 7B For HS 103 Week 8Document7 pagesCase Study 7B For HS 103 Week 8Rijane Tabonoc OmlangNo ratings yet
- Advances in Prostaglandin, Leukotriene, and Other Bioactive Lipid ResearchDocument243 pagesAdvances in Prostaglandin, Leukotriene, and Other Bioactive Lipid ResearchCarmen PopaNo ratings yet
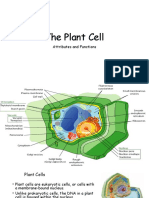
- The Plant CellDocument30 pagesThe Plant CellMichael GentilesNo ratings yet
- Choosing The Raw Materials For FPJ: Agricultural Training Institute Managing Editor and Layout Artist EditorsDocument2 pagesChoosing The Raw Materials For FPJ: Agricultural Training Institute Managing Editor and Layout Artist EditorsRONALD PACOLNo ratings yet
- JurnalDocument5 pagesJurnalQorin Diin ArifniNo ratings yet
- Anatomy of Male Genital System in StallionDocument15 pagesAnatomy of Male Genital System in StallionbaitongrstNo ratings yet
- General Biology - Chapter IDocument10 pagesGeneral Biology - Chapter IG.k. Vinnan Rao100% (2)