Download as docx, pdf, or txt
You might also like
- OCANZ Sept 2007 Paper 1Document4 pagesOCANZ Sept 2007 Paper 1Ben Joon50% (2)
- Oral Health ProgramDocument6 pagesOral Health ProgramPoohlarica UyNo ratings yet
- 100 Case Histories in Clinical Medicine For MRCP by Jypee (PART 1) PDFDocument352 pages100 Case Histories in Clinical Medicine For MRCP by Jypee (PART 1) PDFmuntaser67% (3)
- Cephalopelvic Disproportion (CPD)Document20 pagesCephalopelvic Disproportion (CPD)Natukunda Dianah100% (4)
- Critical Decisions in Periodontology 4th Ed. 2003 - Hall (BC DECKER) PDFDocument378 pagesCritical Decisions in Periodontology 4th Ed. 2003 - Hall (BC DECKER) PDFkharida100% (1)
- Pressure SoreDocument3 pagesPressure SoreGhadaNo ratings yet
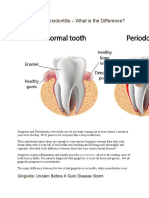
- What Is The Definition of Periodontitis?Document3 pagesWhat Is The Definition of Periodontitis?Sakshi RanaNo ratings yet
- Periodontics: PeriodontitisDocument6 pagesPeriodontics: PeriodontitismarkoNo ratings yet
- By Mayo Clinic Staff: Click To EnlargeDocument4 pagesBy Mayo Clinic Staff: Click To EnlargeLexie DvrelsNo ratings yet
- HTTPDocument7 pagesHTTPErvic SitjarNo ratings yet
- Chapter Seven: Periodontal DiseasesDocument51 pagesChapter Seven: Periodontal DiseasesPande Ari Merdana PutraNo ratings yet
- Oral Health: What Are Periodontal Diseases?Document3 pagesOral Health: What Are Periodontal Diseases?ZeLia Scofield LiverpudlianNo ratings yet
- Periodontal Diseases: Presented By: Syeda Zeenat Raza Maryam Naem Amrit Mir Humera LiaquatDocument21 pagesPeriodontal Diseases: Presented By: Syeda Zeenat Raza Maryam Naem Amrit Mir Humera LiaquatibrahimddgsNo ratings yet
- Highlights Symptoms of Periodontal DiseaseDocument12 pagesHighlights Symptoms of Periodontal DiseaseTriana Wahyu SaputriNo ratings yet
- Periodontitis (Gum Disease) Causes, Symptoms, and Treatment 3Document1 pagePeriodontitis (Gum Disease) Causes, Symptoms, and Treatment 3tdyg96cxkhNo ratings yet
- 3210 Gingivitis: Calcium Channel Blockers (Drugs Used To Treat High Blood Pressure) Can Also Induce GingivitisDocument2 pages3210 Gingivitis: Calcium Channel Blockers (Drugs Used To Treat High Blood Pressure) Can Also Induce GingivitisSriLestariFajerinNo ratings yet
- Iwst10 IktDocument6 pagesIwst10 Ikt9bgnyshtbhNo ratings yet
- A4 UK TeethDocument4 pagesA4 UK TeethkeluargaNo ratings yet
- Pericoronitis PDFDocument2 pagesPericoronitis PDFLourdes RodriguezNo ratings yet
- 4 Tema 5 Notion About Periodontal Diseases Classification-78026Document48 pages4 Tema 5 Notion About Periodontal Diseases Classification-78026Salameh Abu MUSSANo ratings yet
- Gum DiseaseDocument13 pagesGum DiseaseThaer ZabenNo ratings yet
- Gingivitis Vs PeriodontitisDocument2 pagesGingivitis Vs Periodontitisandreas kevinNo ratings yet
- GingivitisDocument2 pagesGingivitisPatricia MedeirosNo ratings yet
- Periodontal Changes in Ortho Treatment / Orthodontic Courses by Indian Dental AcademyDocument81 pagesPeriodontal Changes in Ortho Treatment / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Gingivitis A Silent Disease PDFDocument4 pagesGingivitis A Silent Disease PDFPragita Ayu SaputriNo ratings yet
- Perio Paper FinalDocument6 pagesPerio Paper Finalapi-546518451No ratings yet
- 2 - 5242358943157590113 Seminar PeriodonticDocument23 pages2 - 5242358943157590113 Seminar PeriodonticHhNo ratings yet
- Periodontal DiseasesDocument15 pagesPeriodontal DiseasesNatalia TenggonoNo ratings yet
- GINGIVITISDocument43 pagesGINGIVITISRamyaNo ratings yet
- Dental Plaque: Dental Diseases and Risk of Coronary Heart Disease and MortalityDocument54 pagesDental Plaque: Dental Diseases and Risk of Coronary Heart Disease and MortalityNabilah ZulkiflyNo ratings yet
- What Is A Dental Abscess?Document3 pagesWhat Is A Dental Abscess?Nabila RizkikaNo ratings yet
- Dental Presentation: Created by CharlesDocument8 pagesDental Presentation: Created by CharlesDiana DeeDee LimNo ratings yet
- Periodontal DiseaseDocument4 pagesPeriodontal DiseaseAndika SulistianNo ratings yet
- Toothache and InfectionDocument31 pagesToothache and Infectionishaaadam114No ratings yet
- Presentation 1. Treatment Planning For The Immediate Denture 2. The Patient With Periodontal DiseaseDocument19 pagesPresentation 1. Treatment Planning For The Immediate Denture 2. The Patient With Periodontal DiseaseNika Permata DelaNo ratings yet
- Oral Hygiene Patient EducationDocument32 pagesOral Hygiene Patient EducationAsma AnjumNo ratings yet
- GingivitisDocument9 pagesGingivitisAraceli Margarita Carmona PeraltaNo ratings yet
- EndodonticsDocument6 pagesEndodonticsBilly Joe VillanuevaNo ratings yet
- Scaling and Root Planing: Dental Scaling Is Routinely Performed ToDocument3 pagesScaling and Root Planing: Dental Scaling Is Routinely Performed ToCharlie McdonnellNo ratings yet
- Singh BrijendraDocument5 pagesSingh BrijendraAfianti SulastriNo ratings yet
- Definition GingivitisDocument7 pagesDefinition GingivitisverenNo ratings yet
- ADA PatientSmart Preventing Perio PDFDocument4 pagesADA PatientSmart Preventing Perio PDFJoe WattimenaNo ratings yet
- Scaling and Root Planing Stud 1-241481Document2 pagesScaling and Root Planing Stud 1-241481Adelina FrunzeNo ratings yet
- Introduction To Periodontics: Dr. Abeer HamdounahDocument32 pagesIntroduction To Periodontics: Dr. Abeer HamdounahNowf AlturkiNo ratings yet
- RECESSION by Hamza NadeemDocument18 pagesRECESSION by Hamza NadeemHamza NadeemNo ratings yet
- Gingivitis PerioDocument2 pagesGingivitis PerioFeyza ÇETİNNo ratings yet
- Perio AssiDocument9 pagesPerio AssiKarim Mohamed Fayez Farahat MahmoudNo ratings yet
- Oral Hygiene TipsDocument3 pagesOral Hygiene Tipsdr parveen bathlaNo ratings yet
- Understanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsFrom EverandUnderstanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsNo ratings yet
- Periodontal Gum DiseaseDocument9 pagesPeriodontal Gum DiseaseazifattahNo ratings yet
- Periodontal DiseasesDocument20 pagesPeriodontal DiseasesĐỗ Thành KhangNo ratings yet
- Prevention of Periodontal Disease HandoutDocument13 pagesPrevention of Periodontal Disease HandoutShady AnwarNo ratings yet
- Unit 4. Calculus CaseDocument13 pagesUnit 4. Calculus CasehariyaniNo ratings yet
- PeriodontalDocument3 pagesPeriodontalP?TR�NJEI BOGDAN- ALEXANDRUNo ratings yet
- Definition:: GingivitisDocument6 pagesDefinition:: GingivitisEimhie Lee CasiNo ratings yet
- What Is Gingivitis?Document5 pagesWhat Is Gingivitis?Ayesha AwanNo ratings yet
- Dental AbscessDocument14 pagesDental Abscessvinnu kalyanNo ratings yet
- 1.structure of The TeethDocument5 pages1.structure of The TeethCălin PavelNo ratings yet
- PerioDocument1 pagePerioSarah LewisNo ratings yet
- Management of Deep Caries LesionDocument14 pagesManagement of Deep Caries LesionCah YaniNo ratings yet
- What Is Dental PlaqueDocument9 pagesWhat Is Dental PlaqueHesham100% (1)
- Lec 5Document65 pagesLec 5abdulrazaqNo ratings yet
- Effectiveness of Interdental and Toothbrush Aids in The Reduction of GingivitisDocument9 pagesEffectiveness of Interdental and Toothbrush Aids in The Reduction of Gingivitisjwguan94No ratings yet
- Dokumen - Tips 4 Epidemiology of Periodontal Diseases 1pptDocument22 pagesDokumen - Tips 4 Epidemiology of Periodontal Diseases 1pptHimanshu GargNo ratings yet
- ProDentim Review - How To Cure Gum Disease ?: How To Cure Tooth Decay Naturally....!!From EverandProDentim Review - How To Cure Gum Disease ?: How To Cure Tooth Decay Naturally....!!No ratings yet
- 109 - Obstructive Lung DiseasesDocument8 pages109 - Obstructive Lung DiseasesCharisa Antonette HuelvaNo ratings yet
- Endocarditis (Vegetations) : Non-InfectiveDocument18 pagesEndocarditis (Vegetations) : Non-InfectiveRakesh jhaNo ratings yet
- Entamoeba HistolyticaDocument5 pagesEntamoeba HistolyticaiqraNo ratings yet
- Ascariasis Presenting As Acute Abdomen - A Case ReportDocument3 pagesAscariasis Presenting As Acute Abdomen - A Case ReportSuryooNo ratings yet
- 10 1182@asheducation-2012 1 7Document6 pages10 1182@asheducation-2012 1 7nurdiansyahNo ratings yet
- Abstract ESPRMDocument1 pageAbstract ESPRMAdy LunguNo ratings yet
- dsm5 Neurocognitivedisorders JesteDocument49 pagesdsm5 Neurocognitivedisorders Jesteapi-216587414No ratings yet
- Uk007 2223 006609Document3 pagesUk007 2223 006609Arpit KumarNo ratings yet
- CU5Document13 pagesCU5kuu faal100% (3)
- CHN Q&aDocument14 pagesCHN Q&aMonchikitowNo ratings yet
- CCA Final Exam Review 06 - 02Document4 pagesCCA Final Exam Review 06 - 02Stephen_haslundNo ratings yet
- Measures of MorbidityDocument25 pagesMeasures of MorbiditySaluja Chettri PradhanNo ratings yet
- Cot-Problem and SolutionDocument47 pagesCot-Problem and SolutionYnan Esteron HernandezNo ratings yet
- Renal TumorsDocument50 pagesRenal TumorseuromonNo ratings yet
- Loa LoaDocument22 pagesLoa LoaphilmonNo ratings yet
- Bipolar Disorder in Postpartum Women - Epidemiology, Clinical Features, Assessment, and Diagnosis PDFDocument14 pagesBipolar Disorder in Postpartum Women - Epidemiology, Clinical Features, Assessment, and Diagnosis PDFdreamingNo ratings yet
- LFT (Liver Function Test) : Biological Reference Results Units Test NameDocument4 pagesLFT (Liver Function Test) : Biological Reference Results Units Test Namemetepraju0210No ratings yet
- Meningismus Vs MeningitisDocument19 pagesMeningismus Vs MeningitisRanna HertenizaNo ratings yet
- Expanded Newborn Screening BrochureDocument2 pagesExpanded Newborn Screening BrochureKRISTINE ANGELIE PANESNo ratings yet
- Kaoshiki BenefitsDocument1 pageKaoshiki BenefitsABRACADABRA_1234No ratings yet
- APA - DSM5 - Severity Measure For Separation Anxiety Disorder Adult PDFDocument3 pagesAPA - DSM5 - Severity Measure For Separation Anxiety Disorder Adult PDFMelissandreNo ratings yet
- Ceftriaxone-Induced Fatal Anaphylaxis Shock at An Emergency Department: A Case ReportDocument3 pagesCeftriaxone-Induced Fatal Anaphylaxis Shock at An Emergency Department: A Case ReportHeLena NukaNo ratings yet
- OET Test 1 Listening Answers - Part A and BDocument6 pagesOET Test 1 Listening Answers - Part A and Bjeet meharNo ratings yet
- "Contagion" Film Analysis Name: Diestro, Angela Mae Section: BSN 1 BDocument4 pages"Contagion" Film Analysis Name: Diestro, Angela Mae Section: BSN 1 Bangela Mae Diestro50% (2)
- Test Bank Pathophysiology Introductory Concepts and Clinical Perspectives 2nd Edition CapriottiDocument16 pagesTest Bank Pathophysiology Introductory Concepts and Clinical Perspectives 2nd Edition Capriottidaniellediazmdgoefakyn100% (18)