Download as docx, pdf, or txt
You might also like
- Working Together in Clinical SupervisionDocument28 pagesWorking Together in Clinical SupervisionCharleneKronstedt100% (1)
- Annex 1a GlobalRoamer Locations and Mobile Network CoverageDocument34 pagesAnnex 1a GlobalRoamer Locations and Mobile Network CoverageHilmi FuadNo ratings yet
- AdvHumBiol 2016 6 3 112 195316Document9 pagesAdvHumBiol 2016 6 3 112 195316yunitaananda39No ratings yet
- Non-Syndromic Supernumerary Premolars, A Literature Review and A Report of Two CasesDocument5 pagesNon-Syndromic Supernumerary Premolars, A Literature Review and A Report of Two CasesNaji Z. ArandiNo ratings yet
- Supernumerary Teeth: A Review On A Critical Endodontic ChallengeDocument6 pagesSupernumerary Teeth: A Review On A Critical Endodontic ChallengeNaji Z. ArandiNo ratings yet
- The Epidemiology of Supernumerary Teeth and The Associated Molecular MechanismDocument21 pagesThe Epidemiology of Supernumerary Teeth and The Associated Molecular MechanismCalvintNo ratings yet
- Multiple Impacted Permanent and Supernumerary Teeth in The Anterior Mandible of Nonsyndromic Case: A..Document6 pagesMultiple Impacted Permanent and Supernumerary Teeth in The Anterior Mandible of Nonsyndromic Case: A..Zita AprilliaNo ratings yet
- Pattern and Causes of Tooth Extraction in Patients Reporting To A Teaching Dental HospitalDocument6 pagesPattern and Causes of Tooth Extraction in Patients Reporting To A Teaching Dental HospitalAnye PutriNo ratings yet
- Dracula ToothDocument3 pagesDracula ToothLjubomirErdoglijaNo ratings yet
- Tongue Crenation Scalloped Tongue - Case Report PDFDocument4 pagesTongue Crenation Scalloped Tongue - Case Report PDFRiri GustiawarmanNo ratings yet
- Interventions in Management of Dental Fluorosis AnDocument6 pagesInterventions in Management of Dental Fluorosis Ankhalisha salsabilaNo ratings yet
- Literature Review Dental FluorosisDocument5 pagesLiterature Review Dental Fluorosisafmzfmeeavndqe100% (1)
- Abrasi DLLDocument9 pagesAbrasi DLLDiana Gita MentariNo ratings yet
- A Review On Non-Syndromic Tooth Agenesis Associated With PAX9 MutationsDocument7 pagesA Review On Non-Syndromic Tooth Agenesis Associated With PAX9 Mutationssümeyra akkoçNo ratings yet
- Tongue Crenation Scalloped Tongue - Case ReportDocument4 pagesTongue Crenation Scalloped Tongue - Case Reportceceu nahhNo ratings yet
- Tooth Surface Loss Revisited: Classification, Etiology, and ManagementDocument9 pagesTooth Surface Loss Revisited: Classification, Etiology, and Managementkhalida iftikharNo ratings yet
- Jos 10 17Document7 pagesJos 10 17Thibaut BossuytNo ratings yet
- Rare and Common Variants Conferring Risk of Tooth Agenesis: Research Reports: ClinicalDocument9 pagesRare and Common Variants Conferring Risk of Tooth Agenesis: Research Reports: ClinicalMellati Dian utamiNo ratings yet
- Forensics in Pediatric DentistryDocument4 pagesForensics in Pediatric DentistrySurbhi SinghNo ratings yet
- Periodontal ExodontiaDocument5 pagesPeriodontal ExodontiaDARKS_EDSNo ratings yet
- Extraction of Primary Teeth in Children: An Observational StudyDocument6 pagesExtraction of Primary Teeth in Children: An Observational StudyhayiarNo ratings yet
- Odontology Literature ReviewDocument6 pagesOdontology Literature Reviewafmzxhvgfvprhm100% (1)
- 2020 Article 237Document21 pages2020 Article 237Tsaniya KamilahNo ratings yet
- Immediate Post-Operative Rehabilitation After Decoronation. A Systematic ReviewDocument21 pagesImmediate Post-Operative Rehabilitation After Decoronation. A Systematic ReviewAb DouNo ratings yet
- Prevalence, Characteristic Features, and Complications Associated With The Occurrence of Unerupted Permanent IncisorsDocument14 pagesPrevalence, Characteristic Features, and Complications Associated With The Occurrence of Unerupted Permanent IncisorsebecerraNo ratings yet
- Effect of Fluoride-Releasing Resin Composite in White Spot Lesions Prevention: A Single-Centre, Split-Mouth, Randomized Controlled TrialDocument7 pagesEffect of Fluoride-Releasing Resin Composite in White Spot Lesions Prevention: A Single-Centre, Split-Mouth, Randomized Controlled TrialXIID 67No ratings yet
- Periodontal Accelerated Osteogenic Orthodontics Technique For RapidDocument10 pagesPeriodontal Accelerated Osteogenic Orthodontics Technique For RapidATZIRI CHAVEZ PORTILLONo ratings yet
- JIndianAcadOralMedRadiol26142-2602347 071343Document4 pagesJIndianAcadOralMedRadiol26142-2602347 071343Jihad Abu LawiNo ratings yet
- Merged 2022 11 15 11-05-10Document31 pagesMerged 2022 11 15 11-05-10DTM FHKNo ratings yet
- Shih 2016Document6 pagesShih 2016fatimahNo ratings yet
- Prevalence and Risk Factors of Tooth Erosion in ChildrenDocument9 pagesPrevalence and Risk Factors of Tooth Erosion in Childrenrosely23001No ratings yet
- Tongue Crenation Scalloped Tongue - Case ReportDocument4 pagesTongue Crenation Scalloped Tongue - Case ReportCleverys Qisthi PhiennaNo ratings yet
- Oral Surgery Research PaperDocument7 pagesOral Surgery Research Paperugmhvdulg100% (1)
- Forensic Odontology A Review.20141212073749Document8 pagesForensic Odontology A Review.20141212073749Apri DhaliwalNo ratings yet
- Acondicionamiento, Adhesión y Cementado de Aparatología Ortodóncica en Dientes Con Alteraciones Del Esmalte. Revisión de LiteraturaDocument10 pagesAcondicionamiento, Adhesión y Cementado de Aparatología Ortodóncica en Dientes Con Alteraciones Del Esmalte. Revisión de Literaturaruqoyah022No ratings yet
- DistomolerDocument5 pagesDistomolerMukarram FaridiNo ratings yet
- Ghitu Florentina 1Document7 pagesGhitu Florentina 1Eduard Gabriel GavrilăNo ratings yet
- Management of Supernumerary Teeth in Children: A Narrative Overview of Published LiteratureDocument8 pagesManagement of Supernumerary Teeth in Children: A Narrative Overview of Published LiteraturePucho Gregorio Caballero PonceNo ratings yet
- Prevalensi Anomali Jumlah Gigi Ditinjau Dari Radiografi Panoramik Di RSGM UNHAS MakassarDocument6 pagesPrevalensi Anomali Jumlah Gigi Ditinjau Dari Radiografi Panoramik Di RSGM UNHAS MakassarImaniar FitriatasyaVWNo ratings yet
- Multiple Unerupted Permanent Teeth Associated With Noonan SyndromeDocument5 pagesMultiple Unerupted Permanent Teeth Associated With Noonan Syndromevighanesh kadamNo ratings yet
- IndianJDentSci93141-465093 125509Document7 pagesIndianJDentSci93141-465093 125509Naji Z. ArandiNo ratings yet
- Jurnal Endo PerioDocument10 pagesJurnal Endo PerioElly ZaiNo ratings yet
- ArticlesDocument7 pagesArticlesAnukrity PathakNo ratings yet
- Analysis of Enamel Rod End Pattern For Personal IdentificationDocument6 pagesAnalysis of Enamel Rod End Pattern For Personal IdentificationNaneunBaboNo ratings yet
- 0.8 Dental Implants in Children - A Multidisciplinary Perspective For Long-Term SuccessDocument8 pages0.8 Dental Implants in Children - A Multidisciplinary Perspective For Long-Term Success2223217No ratings yet
- Outcomes and Prognostic Factors That Influence The SuccessDocument20 pagesOutcomes and Prognostic Factors That Influence The SuccessdwNo ratings yet
- Oral and Dental Alterations and Growth Disruption Following Chemotherapy in Long-Term Survivors of Childhood MalignanciesDocument9 pagesOral and Dental Alterations and Growth Disruption Following Chemotherapy in Long-Term Survivors of Childhood MalignanciesGeorgia.annaNo ratings yet
- De Sousa APBR - in Vitro Tooth Reattachment Technique PDFDocument23 pagesDe Sousa APBR - in Vitro Tooth Reattachment Technique PDFPatricia JesikaNo ratings yet
- Dental Implants in Children: A Multidisciplinary Perspective For Long-Term SuccessDocument5 pagesDental Implants in Children: A Multidisciplinary Perspective For Long-Term SuccessfghdhmdkhNo ratings yet
- Reasons For Extraction of Primary Teeth in Jordan-A Study.: August 2013Document5 pagesReasons For Extraction of Primary Teeth in Jordan-A Study.: August 2013Mutia KumalasariNo ratings yet
- Awareness and Behavior Related To Orthodontic Trea PDFDocument7 pagesAwareness and Behavior Related To Orthodontic Trea PDFAnnisa FadilasariNo ratings yet
- Bushabu CHINA 2016 DIENTES IMPACTADOSDocument7 pagesBushabu CHINA 2016 DIENTES IMPACTADOSPamela CelisNo ratings yet
- Prevalence of Dental Anomalies Among 7 - To 35-Year-Old People in HamadanDocument7 pagesPrevalence of Dental Anomalies Among 7 - To 35-Year-Old People in HamadanPamela CelisNo ratings yet
- 1.miu - Orthodontics For Undergtaduate 6th Edition On CDDocument219 pages1.miu - Orthodontics For Undergtaduate 6th Edition On CDahmedsyNo ratings yet
- Dissertation Topics in Oral and Maxillofacial SurgeryDocument7 pagesDissertation Topics in Oral and Maxillofacial SurgeryWritingPaperHelpProvoNo ratings yet
- Paroliaetal JIDDocument12 pagesParoliaetal JIDHaris KrnicNo ratings yet
- Clinical Exp Dental Res - 2022 - Fekonja - Evaluation of The Eruption of Permanent Teeth and Their Association WithDocument7 pagesClinical Exp Dental Res - 2022 - Fekonja - Evaluation of The Eruption of Permanent Teeth and Their Association WithSarra TekayaNo ratings yet
- Comm Dent Oral Epid - 2006 - Fejerskov - Concepts of Dental Caries and Their Consequences For Understanding The DiseaseDocument9 pagesComm Dent Oral Epid - 2006 - Fejerskov - Concepts of Dental Caries and Their Consequences For Understanding The DiseaseDian MartínezNo ratings yet
- Ne 3Document8 pagesNe 3Zaid DewachiNo ratings yet
- Tooth Mortality: An Analysis of Reasons Underlying The Extraction of Permanent TeethDocument5 pagesTooth Mortality: An Analysis of Reasons Underlying The Extraction of Permanent TeethAlya RosyadaNo ratings yet
- Management of Children With Special Health Care Needs (SHCN) in The Dental Office PDFDocument6 pagesManagement of Children With Special Health Care Needs (SHCN) in The Dental Office PDFNabil AlkaffNo ratings yet
- Safety of Microneedles For Transdermal Drug DeliveryDocument2 pagesSafety of Microneedles For Transdermal Drug DeliveryHiep X NguyenNo ratings yet
- Answer Part 1Document1 pageAnswer Part 1jovelyn bolingetNo ratings yet
- Planificare Engleza 0Document7 pagesPlanificare Engleza 0danielasiposNo ratings yet
- 11 JMSCRDocument6 pages11 JMSCRWuppuluri Jayanth Kumar SharmaNo ratings yet
- Utility Experiment Verifies Destructive Nature of VLF HIPOT Withstand TestingDocument4 pagesUtility Experiment Verifies Destructive Nature of VLF HIPOT Withstand Testingapricot2009No ratings yet
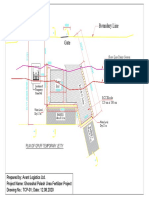
- Boundary Line: Plan of Gpuff Temporary JettyDocument1 pageBoundary Line: Plan of Gpuff Temporary Jettyshafiq_05No ratings yet
- 2024 NM Consultative Meeting For PMNP MPMOsDocument31 pages2024 NM Consultative Meeting For PMNP MPMOssribaccayNo ratings yet
- Issuance of Insanity 2Document278 pagesIssuance of Insanity 2Jonatha B SantosNo ratings yet
- Pengelolaan Kualitas Lingkungan Dengan Pemanfaatan Limbah Cair Dari Industri Tahu Sebagai BiogasDocument17 pagesPengelolaan Kualitas Lingkungan Dengan Pemanfaatan Limbah Cair Dari Industri Tahu Sebagai BiogasMuhammad Sadiqul ImanNo ratings yet
- 2.biological Techniques Procedures and MethodsDocument33 pages2.biological Techniques Procedures and MethodsRheane Joyce CastroNo ratings yet
- Road Safety Training DocumentsDocument25 pagesRoad Safety Training DocumentsAbdullah Al BakyNo ratings yet
- Igneous RocksDocument7 pagesIgneous RocksHamzaBaigNo ratings yet
- Crab Lab ReportDocument2 pagesCrab Lab Reportapi-397859183No ratings yet
- Declaration Good Health Form PDFDocument2 pagesDeclaration Good Health Form PDFMurali SiddarthNo ratings yet
- Traffic SignDocument18 pagesTraffic SignMaria Virginia FernandezNo ratings yet
- Phytochemical Screening and Antimicrobial Assay of Various SeedsDocument9 pagesPhytochemical Screening and Antimicrobial Assay of Various SeedsWendy FXNo ratings yet
- Notice No.34Document2 pagesNotice No.34LuciferNo ratings yet
- Package Dimension (Qcc8C) : WWW - Datasheet.Co - KR WWW - Datasheet.Co - KRDocument3 pagesPackage Dimension (Qcc8C) : WWW - Datasheet.Co - KR WWW - Datasheet.Co - KRindustronicaNo ratings yet
- Swimming Pool BoqDocument5 pagesSwimming Pool Boqfelix sowah-laryeaNo ratings yet
- Conceptual Design For Leachate Treatment Plant (LTP)Document19 pagesConceptual Design For Leachate Treatment Plant (LTP)Akyas M100% (1)
- MET135 Lesson 3 Atmopsheric Moisture and StabilityDocument21 pagesMET135 Lesson 3 Atmopsheric Moisture and StabilityMalik ForbesNo ratings yet
- Morphology McqsDocument8 pagesMorphology McqsHiba Shah100% (2)
- Zagreb-Miler Qualitative Tests Presentation PDFDocument36 pagesZagreb-Miler Qualitative Tests Presentation PDFFernando CruzNo ratings yet
- Physico-Chemical and Microbiological Analysis of Textile Dyeing EffluentsDocument5 pagesPhysico-Chemical and Microbiological Analysis of Textile Dyeing EffluentsIOSRjournalNo ratings yet
- Giant Consumer Product: This Study Resource WasDocument5 pagesGiant Consumer Product: This Study Resource WasKhushbooNo ratings yet
- Torque Values RTJ (B16.5)Document3 pagesTorque Values RTJ (B16.5)ariyamanjulaNo ratings yet
- A Study On Customer Satisfaction Towards Herbal Products Dr. K. S. Kavitha & T. Anish FathimaDocument4 pagesA Study On Customer Satisfaction Towards Herbal Products Dr. K. S. Kavitha & T. Anish Fathimasangeetha0% (1)
- Patella TendonitisDocument43 pagesPatella Tendonitisvijkris1985100% (2)