
Placentitis Abortion Caused by Chlamydia Psittaci Origin: Histological
Placentitis Abortion Caused by Chlamydia Psittaci Origin: Histological
You might also like
- MLS ASCP Exam Recall Questions Flashcards - QuizletDocument8 pagesMLS ASCP Exam Recall Questions Flashcards - Quizletyeliz kurt100% (3)
- Histology Questions USMLE 2017Document13 pagesHistology Questions USMLE 2017Jahanzeb AhmedNo ratings yet
- Case Studies For FinalDocument6 pagesCase Studies For FinalAnh NguyenNo ratings yet
- STD Comparison ChartDocument5 pagesSTD Comparison ChartIvy Tee100% (2)
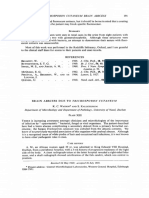
- Tnchosporon Cutaneum Brain Abscess: ClinDocument4 pagesTnchosporon Cutaneum Brain Abscess: ClinIqbal AbdillahNo ratings yet
- NEW EDITABLE New Format New HighDocument434 pagesNEW EDITABLE New Format New Highdrsaimasaeed2No ratings yet
- The Pathology of Abortion Caused by The Infectious Bovine RhinotracheitisDocument11 pagesThe Pathology of Abortion Caused by The Infectious Bovine RhinotracheitisAwker FurtNo ratings yet
- Adult Hypertrophic Pyloric Stenosis Case ReportDocument2 pagesAdult Hypertrophic Pyloric Stenosis Case Reportmaina_luis6031No ratings yet
- J Clin Pathol 1980 Brook 1099 101Document4 pagesJ Clin Pathol 1980 Brook 1099 101ysh_girlNo ratings yet
- Peptostreptococcus Asaccharolyticus: 2001 107 E11 Veronica A. Mas Casullo, Edward Bottone and Betsy C. HeroldDocument6 pagesPeptostreptococcus Asaccharolyticus: 2001 107 E11 Veronica A. Mas Casullo, Edward Bottone and Betsy C. HeroldCarolina Cabrera CernaNo ratings yet
- Tropical Immersion Foot2Document1 pageTropical Immersion Foot2Fenni OktoberryNo ratings yet
- Case 1: Recurrent Pneumonia in A 15-Year-Old Girl: Article Figures & Data Info & Metrics CommentsDocument7 pagesCase 1: Recurrent Pneumonia in A 15-Year-Old Girl: Article Figures & Data Info & Metrics CommentsJoshua MendozaNo ratings yet
- Human Atherosclerotic Plaque Contains Viable InvasiveActinobacillus ActinomycetemcomitansDocument6 pagesHuman Atherosclerotic Plaque Contains Viable InvasiveActinobacillus ActinomycetemcomitansRoza NafilahNo ratings yet
- Structural Changes in Endometrial Basal Glands During MenstruationDocument11 pagesStructural Changes in Endometrial Basal Glands During MenstruationWahab RopekNo ratings yet
- 159 FullDocument19 pages159 FullMina BekNo ratings yet
- Pólipo Vesical 2022Document4 pagesPólipo Vesical 2022ntytapNo ratings yet
- 201 203 AbdominalDocument3 pages201 203 AbdominalManal Salah DorghammNo ratings yet
- Case report intus Draft 20-03-23Document3 pagesCase report intus Draft 20-03-23Sravan JsNo ratings yet
- Embriologi DIKUMPUL!!!Document7 pagesEmbriologi DIKUMPUL!!!Laila Kurnia PramonoNo ratings yet
- 3 Aulia Putri Utoma 3Document4 pages3 Aulia Putri Utoma 3zaki ahmadNo ratings yet
- Cap Polyposis in Children: Case Report and Literature ReviewDocument6 pagesCap Polyposis in Children: Case Report and Literature ReviewLuis ArrietaNo ratings yet
- Hipertensão PulmonarDocument10 pagesHipertensão PulmonarAnnelise GretherNo ratings yet
- American J Rep Immunol - Altered Transcriptional Regulation of Cytokines Growth Factors and ApoptoticDocument9 pagesAmerican J Rep Immunol - Altered Transcriptional Regulation of Cytokines Growth Factors and ApoptoticMenachem FederNo ratings yet
- 1 s2.0 S0015028211027579 MainDocument6 pages1 s2.0 S0015028211027579 Mainvantrung_liNo ratings yet
- 10 1016@j Cvex 2020 01 005Document15 pages10 1016@j Cvex 2020 01 005Ophelia de VosNo ratings yet
- Endocervical Adenocarcinoma in Situ Presenting in Fundal Endometrial Polyp: The Mother of All Skip LesionsDocument4 pagesEndocervical Adenocarcinoma in Situ Presenting in Fundal Endometrial Polyp: The Mother of All Skip LesionsAnonymous YyLSRdNo ratings yet
- Colo-Uterine Fistula, A Rare Complication of Diverticular Disease of The Colon, Case Report and Literature ReviewDocument8 pagesColo-Uterine Fistula, A Rare Complication of Diverticular Disease of The Colon, Case Report and Literature ReviewRandy SaputraNo ratings yet
- Vet Pathol-1990-Barr-354-61Document9 pagesVet Pathol-1990-Barr-354-61Leah DayNo ratings yet
- Picture of The Month: What Is Amniotic Fluid Sludge'?Document6 pagesPicture of The Month: What Is Amniotic Fluid Sludge'?Luis InostrozaNo ratings yet
- Caille AdenovursDocument4 pagesCaille AdenovursSoufian CherkiNo ratings yet
- Goodwin, M. A, Multisystemic Adenovirus Infection in Broiler ChicksDocument4 pagesGoodwin, M. A, Multisystemic Adenovirus Infection in Broiler ChicksAmitNo ratings yet
- Benign Familial HematuriaDocument6 pagesBenign Familial Hematuriasiska_mariannaNo ratings yet
- Pathologic Quiz Case: Residents' PageDocument4 pagesPathologic Quiz Case: Residents' Pagejeka222No ratings yet
- Micro Q Final 2Document45 pagesMicro Q Final 2Rashed Aiman Sameer Alsayyed AlalqamawiNo ratings yet
- Klinefelter Genital AnomaliDocument6 pagesKlinefelter Genital AnomaliPratita Jati PermatasariNo ratings yet
- CMV - Cazuri CliniceDocument5 pagesCMV - Cazuri CliniceMinerva StanciuNo ratings yet
- AmzVLR PathakDocument3 pagesAmzVLR PathakValian IndrianyNo ratings yet
- tmp3D85 TMPDocument6 pagestmp3D85 TMPFrontiersNo ratings yet
- Primary Peritonitis in Children and Adults: T. G. Armitage R. C. Williamson M.B., CH.B., F.R.C.S.Ed. F.R.C.SDocument4 pagesPrimary Peritonitis in Children and Adults: T. G. Armitage R. C. Williamson M.B., CH.B., F.R.C.S.Ed. F.R.C.SAnastasia KvashninaNo ratings yet
- Hepatitis Cronica CaninaDocument19 pagesHepatitis Cronica CaninaAndres Luna MendezNo ratings yet
- Caso 2Document1 pageCaso 2Karina Fischer SigelNo ratings yet
- Fatal Neonatal Septicaemia and Meningitis Due To Haemophilus Influenzae AcquiredDocument2 pagesFatal Neonatal Septicaemia and Meningitis Due To Haemophilus Influenzae AcquiredEden AparicioNo ratings yet
- Emerg 3 168Document2 pagesEmerg 3 168Randy SaputraNo ratings yet
- JVC 36 2 116Document3 pagesJVC 36 2 116baongantran2122002No ratings yet
- Early-Onset Listeriosis in Prematurity: A Case ReportDocument3 pagesEarly-Onset Listeriosis in Prematurity: A Case ReportAzizan HakimNo ratings yet
- JCM 11 05684 v2Document13 pagesJCM 11 05684 v2Qwerty AsdfghNo ratings yet
- Spontaneous Perforated Pyometra With An Intrauterine Device in Menopause: A Case ReportDocument2 pagesSpontaneous Perforated Pyometra With An Intrauterine Device in Menopause: A Case ReportTomy SaputraNo ratings yet
- 104063870001200209Document3 pages104063870001200209Kent Solis VicenteNo ratings yet
- Paediatric Empyema: A Case Report and Literature ReviewDocument5 pagesPaediatric Empyema: A Case Report and Literature ReviewphobicmdNo ratings yet
- Discussion: Meigs' Syndrome and Pseudo-Meigs' SyndromeDocument3 pagesDiscussion: Meigs' Syndrome and Pseudo-Meigs' SyndromeFlapianne SimenceriauNo ratings yet
- Congenital Ovarian CystDocument4 pagesCongenital Ovarian CystSastra SinagaNo ratings yet
- Superior Vesical Fissure: Variant Classical Bladder ExstrophyDocument3 pagesSuperior Vesical Fissure: Variant Classical Bladder ExstrophyChindia BungaNo ratings yet
- AaaaaaaDocument4 pagesAaaaaaaGeorgi GugicevNo ratings yet
- Haemophillus ParainfluenzaeDocument7 pagesHaemophillus ParainfluenzaeAndriucFlaviaNo ratings yet
- Chronic Malabsorption Due Child With Immunoglobulin DeficiencyDocument3 pagesChronic Malabsorption Due Child With Immunoglobulin DeficiencyCentro De Copiado Luna RtNo ratings yet
- Times,: KaufmanDocument2 pagesTimes,: KaufmanBembie PurwonoNo ratings yet
- First Trimester Sonographic Diagnosis of Limb-Body Wall Defect Associating Both Cephalic and Thoraco-Abdominal Defects - A Case Report and Literature UpdateDocument3 pagesFirst Trimester Sonographic Diagnosis of Limb-Body Wall Defect Associating Both Cephalic and Thoraco-Abdominal Defects - A Case Report and Literature UpdateIvan DavrayNo ratings yet
- Cervical Insufficiency A New Issue For Guidelines On Prevention of Perinatal Group B Streptococcal DiseaseDocument6 pagesCervical Insufficiency A New Issue For Guidelines On Prevention of Perinatal Group B Streptococcal Diseaseatika sgrtNo ratings yet
- Indian Journal of Human Genetics: A Case of Kartagener's Syndrome: Importance of Early Diagnosis and TreatmentDocument8 pagesIndian Journal of Human Genetics: A Case of Kartagener's Syndrome: Importance of Early Diagnosis and TreatmentHendra SusantoNo ratings yet
- Blue Nevus of The Uterine CervixDocument8 pagesBlue Nevus of The Uterine CervixNoel YuanNo ratings yet
- Pathology BDocument5 pagesPathology Bttdjhg2p6kNo ratings yet
- Communicable Disease Control in Complex EmergenciesDocument14 pagesCommunicable Disease Control in Complex EmergenciesDika Agustinus AndikaNo ratings yet
- DR Auladi Halim Umar Lubis - MALARIADocument37 pagesDR Auladi Halim Umar Lubis - MALARIAAuladi Lubis ∑No ratings yet
- Non Specific and Specific Host Defense MechanismDocument7 pagesNon Specific and Specific Host Defense Mechanismcheskhadomingo33No ratings yet
- JPCC January - March 2016 PDFDocument70 pagesJPCC January - March 2016 PDFseema sharmaNo ratings yet
- Cows Milk Protein AllergyDocument9 pagesCows Milk Protein Allergymrs raamNo ratings yet
- Blood Group Incompatibility RH DiseaseDocument35 pagesBlood Group Incompatibility RH DiseaseRay SadisNo ratings yet
- OsteomyelitisDocument29 pagesOsteomyelitisPramod N KNo ratings yet
- INFECTION CONTROL 2nd YearDocument12 pagesINFECTION CONTROL 2nd YearAmy LalringhluaniNo ratings yet
- Ethiopia Consolidated ART Guideline 2014Document165 pagesEthiopia Consolidated ART Guideline 2014TayeNo ratings yet
- Communicable DiseaseDocument193 pagesCommunicable DiseaseLuvastranger Auger100% (2)
- Bilateral Acute Tibial Osteomyelitis in A Patient Without An Underlying Disease: A Case ReportDocument4 pagesBilateral Acute Tibial Osteomyelitis in A Patient Without An Underlying Disease: A Case ReportIfal JakNo ratings yet
- Mapeh Pamphlet8Document4 pagesMapeh Pamphlet8Yethelesia XIINo ratings yet
- NATURAL IMMUNItY-Why Not VaccinateDocument11 pagesNATURAL IMMUNItY-Why Not Vaccinatemonika_boskovic_1No ratings yet
- Laporan 27 April 2021 NewDocument1,166 pagesLaporan 27 April 2021 NewRahmatul Fittri yulizarNo ratings yet
- Immunology: Cells and Organs of The Immune SystemDocument54 pagesImmunology: Cells and Organs of The Immune SystemTheComNo ratings yet
- Nephritic SyndromeDocument19 pagesNephritic SyndromesangheetaNo ratings yet
- Manoj Visitor Pass (C26796)Document11 pagesManoj Visitor Pass (C26796)TRISTAR TEKZONENo ratings yet
- Fitzpatricks Dermatology 9th Edition 3124Document1 pageFitzpatricks Dermatology 9th Edition 3124DennisSujayaNo ratings yet
- Sema4 COVID 19 FAQDocument2 pagesSema4 COVID 19 FAQEduardo MongeNo ratings yet
- HIV Based On Harrison's Principles of Medicine 21 EdDocument4 pagesHIV Based On Harrison's Principles of Medicine 21 EdBatch V Med 2 SY 21-22No ratings yet
- P-Form Weekly Idsp Alert - Week 05 BANASKANTHA PALANPURDocument10 pagesP-Form Weekly Idsp Alert - Week 05 BANASKANTHA PALANPURPankaj ModhNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsAlif HazmiNo ratings yet
- Antibodies and AntigensDocument1 pageAntibodies and AntigensKaty DonNo ratings yet
- Immunization Programme in NepalDocument13 pagesImmunization Programme in Nepalrina dutta100% (1)
- UTI Treatment Algorithm - Sharp Mesa Vista 2Document3 pagesUTI Treatment Algorithm - Sharp Mesa Vista 2Fitri 1997No ratings yet
- Diagnostic Report: Patient Name: Rohan ROHAM01089680 0080UD005726Document2 pagesDiagnostic Report: Patient Name: Rohan ROHAM01089680 0080UD005726tusharNo ratings yet
- Assignment2 PDFDocument4 pagesAssignment2 PDFJavier GonzalezNo ratings yet
- OnchocerciasisDocument5 pagesOnchocerciasislordbennett505No ratings yet






















































































Download as pdf or txt
You might also like
- MLS ASCP Exam Recall Questions Flashcards - QuizletDocument8 pagesMLS ASCP Exam Recall Questions Flashcards - Quizletyeliz kurt100% (3)
- Histology Questions USMLE 2017Document13 pagesHistology Questions USMLE 2017Jahanzeb AhmedNo ratings yet
- Case Studies For FinalDocument6 pagesCase Studies For FinalAnh NguyenNo ratings yet
- STD Comparison ChartDocument5 pagesSTD Comparison ChartIvy Tee100% (2)
- Tnchosporon Cutaneum Brain Abscess: ClinDocument4 pagesTnchosporon Cutaneum Brain Abscess: ClinIqbal AbdillahNo ratings yet
- NEW EDITABLE New Format New HighDocument434 pagesNEW EDITABLE New Format New Highdrsaimasaeed2No ratings yet
- The Pathology of Abortion Caused by The Infectious Bovine RhinotracheitisDocument11 pagesThe Pathology of Abortion Caused by The Infectious Bovine RhinotracheitisAwker FurtNo ratings yet
- Adult Hypertrophic Pyloric Stenosis Case ReportDocument2 pagesAdult Hypertrophic Pyloric Stenosis Case Reportmaina_luis6031No ratings yet
- J Clin Pathol 1980 Brook 1099 101Document4 pagesJ Clin Pathol 1980 Brook 1099 101ysh_girlNo ratings yet
- Peptostreptococcus Asaccharolyticus: 2001 107 E11 Veronica A. Mas Casullo, Edward Bottone and Betsy C. HeroldDocument6 pagesPeptostreptococcus Asaccharolyticus: 2001 107 E11 Veronica A. Mas Casullo, Edward Bottone and Betsy C. HeroldCarolina Cabrera CernaNo ratings yet
- Tropical Immersion Foot2Document1 pageTropical Immersion Foot2Fenni OktoberryNo ratings yet
- Case 1: Recurrent Pneumonia in A 15-Year-Old Girl: Article Figures & Data Info & Metrics CommentsDocument7 pagesCase 1: Recurrent Pneumonia in A 15-Year-Old Girl: Article Figures & Data Info & Metrics CommentsJoshua MendozaNo ratings yet
- Human Atherosclerotic Plaque Contains Viable InvasiveActinobacillus ActinomycetemcomitansDocument6 pagesHuman Atherosclerotic Plaque Contains Viable InvasiveActinobacillus ActinomycetemcomitansRoza NafilahNo ratings yet
- Structural Changes in Endometrial Basal Glands During MenstruationDocument11 pagesStructural Changes in Endometrial Basal Glands During MenstruationWahab RopekNo ratings yet
- 159 FullDocument19 pages159 FullMina BekNo ratings yet
- Pólipo Vesical 2022Document4 pagesPólipo Vesical 2022ntytapNo ratings yet
- 201 203 AbdominalDocument3 pages201 203 AbdominalManal Salah DorghammNo ratings yet
- Case report intus Draft 20-03-23Document3 pagesCase report intus Draft 20-03-23Sravan JsNo ratings yet
- Embriologi DIKUMPUL!!!Document7 pagesEmbriologi DIKUMPUL!!!Laila Kurnia PramonoNo ratings yet
- 3 Aulia Putri Utoma 3Document4 pages3 Aulia Putri Utoma 3zaki ahmadNo ratings yet
- Cap Polyposis in Children: Case Report and Literature ReviewDocument6 pagesCap Polyposis in Children: Case Report and Literature ReviewLuis ArrietaNo ratings yet
- Hipertensão PulmonarDocument10 pagesHipertensão PulmonarAnnelise GretherNo ratings yet
- American J Rep Immunol - Altered Transcriptional Regulation of Cytokines Growth Factors and ApoptoticDocument9 pagesAmerican J Rep Immunol - Altered Transcriptional Regulation of Cytokines Growth Factors and ApoptoticMenachem FederNo ratings yet
- 1 s2.0 S0015028211027579 MainDocument6 pages1 s2.0 S0015028211027579 Mainvantrung_liNo ratings yet
- 10 1016@j Cvex 2020 01 005Document15 pages10 1016@j Cvex 2020 01 005Ophelia de VosNo ratings yet
- Endocervical Adenocarcinoma in Situ Presenting in Fundal Endometrial Polyp: The Mother of All Skip LesionsDocument4 pagesEndocervical Adenocarcinoma in Situ Presenting in Fundal Endometrial Polyp: The Mother of All Skip LesionsAnonymous YyLSRdNo ratings yet
- Colo-Uterine Fistula, A Rare Complication of Diverticular Disease of The Colon, Case Report and Literature ReviewDocument8 pagesColo-Uterine Fistula, A Rare Complication of Diverticular Disease of The Colon, Case Report and Literature ReviewRandy SaputraNo ratings yet
- Vet Pathol-1990-Barr-354-61Document9 pagesVet Pathol-1990-Barr-354-61Leah DayNo ratings yet
- Picture of The Month: What Is Amniotic Fluid Sludge'?Document6 pagesPicture of The Month: What Is Amniotic Fluid Sludge'?Luis InostrozaNo ratings yet
- Caille AdenovursDocument4 pagesCaille AdenovursSoufian CherkiNo ratings yet
- Goodwin, M. A, Multisystemic Adenovirus Infection in Broiler ChicksDocument4 pagesGoodwin, M. A, Multisystemic Adenovirus Infection in Broiler ChicksAmitNo ratings yet
- Benign Familial HematuriaDocument6 pagesBenign Familial Hematuriasiska_mariannaNo ratings yet
- Pathologic Quiz Case: Residents' PageDocument4 pagesPathologic Quiz Case: Residents' Pagejeka222No ratings yet
- Micro Q Final 2Document45 pagesMicro Q Final 2Rashed Aiman Sameer Alsayyed AlalqamawiNo ratings yet
- Klinefelter Genital AnomaliDocument6 pagesKlinefelter Genital AnomaliPratita Jati PermatasariNo ratings yet
- CMV - Cazuri CliniceDocument5 pagesCMV - Cazuri CliniceMinerva StanciuNo ratings yet
- AmzVLR PathakDocument3 pagesAmzVLR PathakValian IndrianyNo ratings yet
- tmp3D85 TMPDocument6 pagestmp3D85 TMPFrontiersNo ratings yet
- Primary Peritonitis in Children and Adults: T. G. Armitage R. C. Williamson M.B., CH.B., F.R.C.S.Ed. F.R.C.SDocument4 pagesPrimary Peritonitis in Children and Adults: T. G. Armitage R. C. Williamson M.B., CH.B., F.R.C.S.Ed. F.R.C.SAnastasia KvashninaNo ratings yet
- Hepatitis Cronica CaninaDocument19 pagesHepatitis Cronica CaninaAndres Luna MendezNo ratings yet
- Caso 2Document1 pageCaso 2Karina Fischer SigelNo ratings yet
- Fatal Neonatal Septicaemia and Meningitis Due To Haemophilus Influenzae AcquiredDocument2 pagesFatal Neonatal Septicaemia and Meningitis Due To Haemophilus Influenzae AcquiredEden AparicioNo ratings yet
- Emerg 3 168Document2 pagesEmerg 3 168Randy SaputraNo ratings yet
- JVC 36 2 116Document3 pagesJVC 36 2 116baongantran2122002No ratings yet
- Early-Onset Listeriosis in Prematurity: A Case ReportDocument3 pagesEarly-Onset Listeriosis in Prematurity: A Case ReportAzizan HakimNo ratings yet
- JCM 11 05684 v2Document13 pagesJCM 11 05684 v2Qwerty AsdfghNo ratings yet
- Spontaneous Perforated Pyometra With An Intrauterine Device in Menopause: A Case ReportDocument2 pagesSpontaneous Perforated Pyometra With An Intrauterine Device in Menopause: A Case ReportTomy SaputraNo ratings yet
- 104063870001200209Document3 pages104063870001200209Kent Solis VicenteNo ratings yet
- Paediatric Empyema: A Case Report and Literature ReviewDocument5 pagesPaediatric Empyema: A Case Report and Literature ReviewphobicmdNo ratings yet
- Discussion: Meigs' Syndrome and Pseudo-Meigs' SyndromeDocument3 pagesDiscussion: Meigs' Syndrome and Pseudo-Meigs' SyndromeFlapianne SimenceriauNo ratings yet
- Congenital Ovarian CystDocument4 pagesCongenital Ovarian CystSastra SinagaNo ratings yet
- Superior Vesical Fissure: Variant Classical Bladder ExstrophyDocument3 pagesSuperior Vesical Fissure: Variant Classical Bladder ExstrophyChindia BungaNo ratings yet
- AaaaaaaDocument4 pagesAaaaaaaGeorgi GugicevNo ratings yet
- Haemophillus ParainfluenzaeDocument7 pagesHaemophillus ParainfluenzaeAndriucFlaviaNo ratings yet
- Chronic Malabsorption Due Child With Immunoglobulin DeficiencyDocument3 pagesChronic Malabsorption Due Child With Immunoglobulin DeficiencyCentro De Copiado Luna RtNo ratings yet
- Times,: KaufmanDocument2 pagesTimes,: KaufmanBembie PurwonoNo ratings yet
- First Trimester Sonographic Diagnosis of Limb-Body Wall Defect Associating Both Cephalic and Thoraco-Abdominal Defects - A Case Report and Literature UpdateDocument3 pagesFirst Trimester Sonographic Diagnosis of Limb-Body Wall Defect Associating Both Cephalic and Thoraco-Abdominal Defects - A Case Report and Literature UpdateIvan DavrayNo ratings yet
- Cervical Insufficiency A New Issue For Guidelines On Prevention of Perinatal Group B Streptococcal DiseaseDocument6 pagesCervical Insufficiency A New Issue For Guidelines On Prevention of Perinatal Group B Streptococcal Diseaseatika sgrtNo ratings yet
- Indian Journal of Human Genetics: A Case of Kartagener's Syndrome: Importance of Early Diagnosis and TreatmentDocument8 pagesIndian Journal of Human Genetics: A Case of Kartagener's Syndrome: Importance of Early Diagnosis and TreatmentHendra SusantoNo ratings yet
- Blue Nevus of The Uterine CervixDocument8 pagesBlue Nevus of The Uterine CervixNoel YuanNo ratings yet
- Pathology BDocument5 pagesPathology Bttdjhg2p6kNo ratings yet
- Communicable Disease Control in Complex EmergenciesDocument14 pagesCommunicable Disease Control in Complex EmergenciesDika Agustinus AndikaNo ratings yet
- DR Auladi Halim Umar Lubis - MALARIADocument37 pagesDR Auladi Halim Umar Lubis - MALARIAAuladi Lubis ∑No ratings yet
- Non Specific and Specific Host Defense MechanismDocument7 pagesNon Specific and Specific Host Defense Mechanismcheskhadomingo33No ratings yet
- JPCC January - March 2016 PDFDocument70 pagesJPCC January - March 2016 PDFseema sharmaNo ratings yet
- Cows Milk Protein AllergyDocument9 pagesCows Milk Protein Allergymrs raamNo ratings yet
- Blood Group Incompatibility RH DiseaseDocument35 pagesBlood Group Incompatibility RH DiseaseRay SadisNo ratings yet
- OsteomyelitisDocument29 pagesOsteomyelitisPramod N KNo ratings yet
- INFECTION CONTROL 2nd YearDocument12 pagesINFECTION CONTROL 2nd YearAmy LalringhluaniNo ratings yet
- Ethiopia Consolidated ART Guideline 2014Document165 pagesEthiopia Consolidated ART Guideline 2014TayeNo ratings yet
- Communicable DiseaseDocument193 pagesCommunicable DiseaseLuvastranger Auger100% (2)
- Bilateral Acute Tibial Osteomyelitis in A Patient Without An Underlying Disease: A Case ReportDocument4 pagesBilateral Acute Tibial Osteomyelitis in A Patient Without An Underlying Disease: A Case ReportIfal JakNo ratings yet
- Mapeh Pamphlet8Document4 pagesMapeh Pamphlet8Yethelesia XIINo ratings yet
- NATURAL IMMUNItY-Why Not VaccinateDocument11 pagesNATURAL IMMUNItY-Why Not Vaccinatemonika_boskovic_1No ratings yet
- Laporan 27 April 2021 NewDocument1,166 pagesLaporan 27 April 2021 NewRahmatul Fittri yulizarNo ratings yet
- Immunology: Cells and Organs of The Immune SystemDocument54 pagesImmunology: Cells and Organs of The Immune SystemTheComNo ratings yet
- Nephritic SyndromeDocument19 pagesNephritic SyndromesangheetaNo ratings yet
- Manoj Visitor Pass (C26796)Document11 pagesManoj Visitor Pass (C26796)TRISTAR TEKZONENo ratings yet
- Fitzpatricks Dermatology 9th Edition 3124Document1 pageFitzpatricks Dermatology 9th Edition 3124DennisSujayaNo ratings yet
- Sema4 COVID 19 FAQDocument2 pagesSema4 COVID 19 FAQEduardo MongeNo ratings yet
- HIV Based On Harrison's Principles of Medicine 21 EdDocument4 pagesHIV Based On Harrison's Principles of Medicine 21 EdBatch V Med 2 SY 21-22No ratings yet
- P-Form Weekly Idsp Alert - Week 05 BANASKANTHA PALANPURDocument10 pagesP-Form Weekly Idsp Alert - Week 05 BANASKANTHA PALANPURPankaj ModhNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsAlif HazmiNo ratings yet
- Antibodies and AntigensDocument1 pageAntibodies and AntigensKaty DonNo ratings yet
- Immunization Programme in NepalDocument13 pagesImmunization Programme in Nepalrina dutta100% (1)
- UTI Treatment Algorithm - Sharp Mesa Vista 2Document3 pagesUTI Treatment Algorithm - Sharp Mesa Vista 2Fitri 1997No ratings yet
- Diagnostic Report: Patient Name: Rohan ROHAM01089680 0080UD005726Document2 pagesDiagnostic Report: Patient Name: Rohan ROHAM01089680 0080UD005726tusharNo ratings yet
- Assignment2 PDFDocument4 pagesAssignment2 PDFJavier GonzalezNo ratings yet
- OnchocerciasisDocument5 pagesOnchocerciasislordbennett505No ratings yet