Download as pdf or txt
You might also like
- Introversion and Extroversion: Implications For Depression and SuicidalityDocument7 pagesIntroversion and Extroversion: Implications For Depression and SuicidalityHusni FaridNo ratings yet
- Classification of The MeansDocument5 pagesClassification of The Meanserichamilt0n100% (2)
- PIIS0002937822000412Document14 pagesPIIS0002937822000412Andrés Gaviria CNo ratings yet
- Prenatal Diagnosis of 24 Cases of Microduplication 22q11.2: An Investigation of Phenotype-Genotype CorrelationsDocument23 pagesPrenatal Diagnosis of 24 Cases of Microduplication 22q11.2: An Investigation of Phenotype-Genotype CorrelationsBenyam ZenebeNo ratings yet
- Screening For 22q11 2 Deletion With Ultrasound Non Invasive Prenatal TestingDocument2 pagesScreening For 22q11 2 Deletion With Ultrasound Non Invasive Prenatal Testingbashir019No ratings yet
- Daffos Et AlDocument4 pagesDaffos Et AlEmese NagyNo ratings yet
- 2019 Chromosomal Microarray vs. NIPS Analysis of 5541 Low-Risk PregnanciesDocument6 pages2019 Chromosomal Microarray vs. NIPS Analysis of 5541 Low-Risk PregnanciesAhmed H. Ali ElbestaweyNo ratings yet
- Reliable Detection of Subchromosomal Deletions and Duplications Using Cell Based Noninvasive Prenatal TestingDocument10 pagesReliable Detection of Subchromosomal Deletions and Duplications Using Cell Based Noninvasive Prenatal TestingCavin PengNo ratings yet
- Endovaginal Ultrasound and Doppler Findings After First-Trimester Abortion (Journal of Diagnostic Medical Sonography, Vol. 9, Issue 2) (1993)Document1 pageEndovaginal Ultrasound and Doppler Findings After First-Trimester Abortion (Journal of Diagnostic Medical Sonography, Vol. 9, Issue 2) (1993)Orchid LandNo ratings yet
- Non-Invasive Prenatal Tests (NIPT) : Review Article: Maged MN, Mohamed MN, Lamia H.ShehataDocument6 pagesNon-Invasive Prenatal Tests (NIPT) : Review Article: Maged MN, Mohamed MN, Lamia H.Shehatazahra rahmaNo ratings yet
- Genetic Causes of Congenital Diaphragmatic Hernia Wynn2014Document7 pagesGenetic Causes of Congenital Diaphragmatic Hernia Wynn2014Raul A UrbinaNo ratings yet
- 20 - Prenatal Diagnosis by Chromosomal Microarray AnalysisDocument24 pages20 - Prenatal Diagnosis by Chromosomal Microarray AnalysisEgnilton RamosNo ratings yet
- The Current Landscape of Genetic Testing in Cardiovascular Malformations: Opportunities and ChallengesDocument11 pagesThe Current Landscape of Genetic Testing in Cardiovascular Malformations: Opportunities and ChallengesGlauce L TrevisanNo ratings yet
- Genetic - Down SyndromeDocument11 pagesGenetic - Down Syndromelightning proNo ratings yet
- Young 2021Document9 pagesYoung 2021itzmanveshNo ratings yet
- Down Syndrome - Genetics PDFDocument6 pagesDown Syndrome - Genetics PDFHartotok VipnetNo ratings yet
- NEJMoa012113 Genetic TestingDocument9 pagesNEJMoa012113 Genetic TestingRifqi Hamdani PasaribuNo ratings yet
- Cog NTDocument11 pagesCog NTFabiolaQuijaiteNo ratings yet
- E200032 FullDocument13 pagesE200032 FullAlice MaulisovaNo ratings yet
- (10920684 - Neurosurgical Focus) Predictors of Outcome of Subdural Empyema in ChildrenDocument6 pages(10920684 - Neurosurgical Focus) Predictors of Outcome of Subdural Empyema in ChildrenFatima RamirezNo ratings yet
- Nanopore Sequencing of Clonal IGH Rearrangements in Cell-Free DNA As A Biomarker For Acute Lymphoblastic LeukemiaDocument13 pagesNanopore Sequencing of Clonal IGH Rearrangements in Cell-Free DNA As A Biomarker For Acute Lymphoblastic Leukemiapacbi0logyNo ratings yet
- Genetic Diagnostic Methods For Inherited Eye DiseaDocument6 pagesGenetic Diagnostic Methods For Inherited Eye Diseaputri dwi nofrianiNo ratings yet
- Trusight Software Brochure 1070 2020 001 Single PageDocument12 pagesTrusight Software Brochure 1070 2020 001 Single PageDaiane Armstrong FukuyiNo ratings yet
- ADN-CITOMETRIA de FLUJO-cking Et Al-2004-Cancer CytopathologyDocument14 pagesADN-CITOMETRIA de FLUJO-cking Et Al-2004-Cancer Cytopathologycarmen lopezNo ratings yet
- NonInvasive Single Gene Testing 2019Document7 pagesNonInvasive Single Gene Testing 2019MCuk2606No ratings yet
- The Delphi Definition For Selective Fetal Growth Restriction May Not Improve Detection of Pathologic Growth Discordance in Monochorionic TwinsDocument10 pagesThe Delphi Definition For Selective Fetal Growth Restriction May Not Improve Detection of Pathologic Growth Discordance in Monochorionic TwinsAngela FernandezNo ratings yet
- Fped 09 801955Document9 pagesFped 09 801955YandiNo ratings yet
- Fgene 13 842092 PDFDocument8 pagesFgene 13 842092 PDFDang Tran HoangNo ratings yet
- Báo AI TrisomyDocument7 pagesBáo AI TrisomyXuân Trường PhạmNo ratings yet
- 3 - Evolution of Genetic Testing Supports Precision Medicine For Caring Alzheimer's Disease PatientsDocument6 pages3 - Evolution of Genetic Testing Supports Precision Medicine For Caring Alzheimer's Disease Patientsveidamororo17No ratings yet
- 2011 Article 9608Document17 pages2011 Article 9608exome.unipathNo ratings yet
- Single-Nucleotide Polymorphism of The UMOD Promoter Is Associated With The Outcome of Chronic Kidney Disease PatientsDocument5 pagesSingle-Nucleotide Polymorphism of The UMOD Promoter Is Associated With The Outcome of Chronic Kidney Disease Patientssylvi293No ratings yet
- Fced GenetikDocument33 pagesFced GenetikyosuanugrahapratamaNo ratings yet
- Detection of Deletions at 7q11.23 in Williams-BeurenDocument6 pagesDetection of Deletions at 7q11.23 in Williams-BeurenAmisadai ArévaloNo ratings yet
- 2016 Xu Juanjuan-Xeoxat InclusDocument6 pages2016 Xu Juanjuan-Xeoxat InclusivanaNo ratings yet
- Investigating The Child With Intellectual Disability: Review ArticleDocument5 pagesInvestigating The Child With Intellectual Disability: Review ArticleCristinaNo ratings yet
- 3 回顾性病例对照研究 改善IVF临床结局Document7 pages3 回顾性病例对照研究 改善IVF临床结局zjuwindNo ratings yet
- ACOG Practice Bulletin No 99 Management of 39 PDFDocument26 pagesACOG Practice Bulletin No 99 Management of 39 PDFhkdawnwongNo ratings yet
- 2016 Hussein MolCytogenetDocument13 pages2016 Hussein MolCytogenetEduardo PasteneNo ratings yet
- 182 FullDocument15 pages182 FullSonia BalintNo ratings yet
- FullDocument6 pagesFullamarNo ratings yet
- Nejm 199804093381503Document6 pagesNejm 199804093381503Syafrial BarawasNo ratings yet
- Circgen 121 003635Document8 pagesCircgen 121 003635szumutku fanniNo ratings yet
- 10 5858 - Arpa 2022-0225-OaDocument7 pages10 5858 - Arpa 2022-0225-OaSamanthaNo ratings yet
- AgenesiaDocument15 pagesAgenesiametteoroNo ratings yet
- Pulse Oximetry Screening To Detect Critical Congenital Heart Diseases in Asymptomatic NeonatesDocument6 pagesPulse Oximetry Screening To Detect Critical Congenital Heart Diseases in Asymptomatic Neonatesdebbie_rose89No ratings yet
- Chronic Granulomatous DiseaseDocument2 pagesChronic Granulomatous Diseaseyousrazeidan1979No ratings yet
- I Jos 201129Document9 pagesI Jos 201129jklhjNo ratings yet
- The Genetic Landscape of Autism Spectrum Disorders: Developmental Medicine & Child Neurology ReviewDocument7 pagesThe Genetic Landscape of Autism Spectrum Disorders: Developmental Medicine & Child Neurology ReviewNaeem BukhariNo ratings yet
- 646 FullDocument5 pages646 FulljimakosjpNo ratings yet
- WM-1249-EN-001 PrenaTest Key Paper Summary PMCF-StudyDocument2 pagesWM-1249-EN-001 PrenaTest Key Paper Summary PMCF-StudytcNo ratings yet
- Paper NGS LeukemiaDocument15 pagesPaper NGS LeukemiaNatalia SandovalNo ratings yet
- How Far Should We Explore Hypospadias? Next-Generation Sequencing Applied To A Large Cohort of Hypospadiac PatientsDocument9 pagesHow Far Should We Explore Hypospadias? Next-Generation Sequencing Applied To A Large Cohort of Hypospadiac Patientsddd gdhNo ratings yet
- VDR Gene Single Nucleotide Polymorphisms and Their: Association With Risk of Oral Cavity CarcinomaDocument4 pagesVDR Gene Single Nucleotide Polymorphisms and Their: Association With Risk of Oral Cavity CarcinomaFrancine Rossetti DelboniNo ratings yet
- Genes 12 00398Document11 pagesGenes 12 00398Dr LocumsNo ratings yet
- Glaucoma American Journal of OphtalmologyDocument7 pagesGlaucoma American Journal of OphtalmologyListya NormalitaNo ratings yet
- Increased Detection of High Grade CIN, When UsingDocument5 pagesIncreased Detection of High Grade CIN, When Usingggdsnzwbn7No ratings yet
- Impact of Carrier Status Determination For DuchenneDocument5 pagesImpact of Carrier Status Determination For Duchennernnr2159No ratings yet
- Family History and Seizure PendukungDocument5 pagesFamily History and Seizure PendukungBrillyant S RaintamaNo ratings yet
- 2006 - JacquemontDocument8 pages2006 - JacquemontCarlosNo ratings yet
- Krantz 1997Document7 pagesKrantz 1997Ambiguu MihaiNo ratings yet
- Fast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseFrom EverandFast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseNo ratings yet
- Tmi 13078Document10 pagesTmi 13078Husni FaridNo ratings yet
- Study of Socio-Demographic Factors Affecting Preva PDFDocument5 pagesStudy of Socio-Demographic Factors Affecting Preva PDFHusni FaridNo ratings yet
- PJMS 34 959Document5 pagesPJMS 34 959Husni FaridNo ratings yet
- The Modern Day Baby Book: Enacting Good Mothering and Stewarding Privacy On FacebookDocument11 pagesThe Modern Day Baby Book: Enacting Good Mothering and Stewarding Privacy On FacebookHusni FaridNo ratings yet
- 14201Document7 pages14201Husni FaridNo ratings yet
- Human Papillomaviruses: 1. Exposure DataDocument60 pagesHuman Papillomaviruses: 1. Exposure DataHusni FaridNo ratings yet
- TTDocument15 pagesTTHusni FaridNo ratings yet
- Potential Role of Phospholipases in Virulence and Fungal PathogenesisDocument22 pagesPotential Role of Phospholipases in Virulence and Fungal PathogenesisHusni FaridNo ratings yet
- Hubungan Trombositopenia Dengan Manifestasi Klinis Perdarahan Pada Pasien Demam Berdarah Dengue AnakDocument7 pagesHubungan Trombositopenia Dengan Manifestasi Klinis Perdarahan Pada Pasien Demam Berdarah Dengue AnakHusni FaridNo ratings yet
- NIH Public Access: Sleep and Women's HealthDocument31 pagesNIH Public Access: Sleep and Women's HealthHusni FaridNo ratings yet
- Problem Based Learning Lesson PlanDocument3 pagesProblem Based Learning Lesson Planapi-242018367100% (3)
- LP2 2022 YboaDocument30 pagesLP2 2022 Yboalai.creates4uNo ratings yet
- Carla Hernandez 100Document4 pagesCarla Hernandez 100JhunnieEy ReyesNo ratings yet
- CalciumsDocument5 pagesCalciums786lailaNo ratings yet
- NEET UG Biology Biomolecules-2Document20 pagesNEET UG Biology Biomolecules-2VyjayanthiNo ratings yet
- Experiment 3 An O-Toluidine Method For Blood Glucose DeterminationDocument9 pagesExperiment 3 An O-Toluidine Method For Blood Glucose DeterminationAlmas MalikNo ratings yet
- Principles of Medical Technology Practice 1 Midterm TranseesDocument19 pagesPrinciples of Medical Technology Practice 1 Midterm TranseesSean Rafael LedesmaNo ratings yet
- Heredity Class 10Document40 pagesHeredity Class 10ChaithraNo ratings yet
- Microbial Fuel Cells-Challenges and Applications: ArticleDocument10 pagesMicrobial Fuel Cells-Challenges and Applications: ArticleObande OrinyaNo ratings yet
- Studying Human Sexuality: Presented By: Roxan Benlot Magaling Bsed Ii - Social StudiesDocument36 pagesStudying Human Sexuality: Presented By: Roxan Benlot Magaling Bsed Ii - Social StudiesROXAN magalingNo ratings yet
- Biophysical Chemistry of The Ageing Eye Lens.: Proquest Document LinkDocument5 pagesBiophysical Chemistry of The Ageing Eye Lens.: Proquest Document Linkmau tauNo ratings yet
- Full Download Thermodynamics For Engineers Si Edition 1st Edition Kroos Solutions ManualDocument29 pagesFull Download Thermodynamics For Engineers Si Edition 1st Edition Kroos Solutions Manualonodaalipory100% (22)
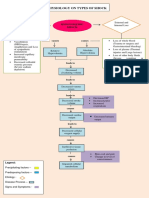
- Pathophysiology On Types of ShockDocument4 pagesPathophysiology On Types of ShockJessa Mae Alforque AsentistaNo ratings yet
- Spring 2004 The Survivior Newsletter Desert SurvivorsDocument32 pagesSpring 2004 The Survivior Newsletter Desert SurvivorsDesert SurvivorsNo ratings yet
- Diversity of Butterflies - Lepidoptera Insecta - From New Nagzira Wildlife Sanctuary Zone III in NNTR, Maharashtra, IndiaDocument6 pagesDiversity of Butterflies - Lepidoptera Insecta - From New Nagzira Wildlife Sanctuary Zone III in NNTR, Maharashtra, IndiaESSENCE - International Journal for Environmental Rehabilitation and ConservaionNo ratings yet
- Broad Aspects of Chemotherapeutic mRNADocument5 pagesBroad Aspects of Chemotherapeutic mRNAInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pedigree Lesson PlanDocument3 pagesPedigree Lesson Planapi-517763318No ratings yet
- Potter S Notion of BioethicsDocument26 pagesPotter S Notion of BioethicsJahiberAlférezNo ratings yet
- Rev Fish Biology and FisheriesDocument17 pagesRev Fish Biology and Fisherieserlin dewiNo ratings yet
- 4 - Teacher Resource 9.4 - Final Model RubricDocument2 pages4 - Teacher Resource 9.4 - Final Model RubricDefault AccountNo ratings yet
- Anatomy of Urinary Tract Systems - 20240117 - 125604 - 0000Document44 pagesAnatomy of Urinary Tract Systems - 20240117 - 125604 - 0000Sneha ThiagarajanNo ratings yet
- Mock 3R - Biology - QDocument4 pagesMock 3R - Biology - QRafael SaldivarNo ratings yet
- Navarro College Medical Laboratory Technology Degree PlanDocument1 pageNavarro College Medical Laboratory Technology Degree PlanNavarro CollegeNo ratings yet
- Zoology ExamDocument4 pagesZoology Examgabriel omliNo ratings yet
- ISUOG Miscarriage and PUVDocument20 pagesISUOG Miscarriage and PUValdo susenoNo ratings yet
- Virtual Herbarium, Documentation and KeysDocument12 pagesVirtual Herbarium, Documentation and KeysVibha TyagiNo ratings yet
- Effect of Mcconnell Taping On Pain, Rom & Grip Strength in Patients With Triangular Fibrocartilage Complex InjuryDocument9 pagesEffect of Mcconnell Taping On Pain, Rom & Grip Strength in Patients With Triangular Fibrocartilage Complex InjuryDr. Krishna N. SharmaNo ratings yet
- Bach Remedy MimulusDocument4 pagesBach Remedy MimulusVaradharajan RNo ratings yet
- Environmental and Forest Biology: Robin W. KimmererDocument16 pagesEnvironmental and Forest Biology: Robin W. KimmererAnonymous 2ZLy5amNo ratings yet