Download as pdf or txt
You might also like
- The Physician ProjectDocument122 pagesThe Physician ProjectRobin SiaNo ratings yet
- Coding Cheat Sheet For Residents in Outpatient MedicineDocument3 pagesCoding Cheat Sheet For Residents in Outpatient MedicineRayCTsai86% (21)
- All Obgyn Osce (2) Good Book For OsceDocument75 pagesAll Obgyn Osce (2) Good Book For OsceMohamed Hassan91% (47)
- Strategies for the MCCQE Part II: Mastering the Clinical Skills Exam in CanadaFrom EverandStrategies for the MCCQE Part II: Mastering the Clinical Skills Exam in CanadaNo ratings yet
- USMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyRating: 5 out of 5 stars5/5 (2)
- Assignment 1Document2 pagesAssignment 1Tang Voon HaoNo ratings yet
- PMDC NEB Exam Medical FormatDocument6 pagesPMDC NEB Exam Medical FormatShawn Parker57% (7)
- LMCC II Compilation Most RecentDocument118 pagesLMCC II Compilation Most RecentEmad Mergan100% (4)
- Oral Board Exam AudioDocument64 pagesOral Board Exam AudioMahjong SirenNo ratings yet
- Chapter 1Document38 pagesChapter 1synap5esNo ratings yet
- DVW Series Error CodesDocument4 pagesDVW Series Error Codeswfaachannel8No ratings yet
- King Abdulaziz Medical Cities (National Guard Hospitals) : Generic Clinical Checklist Area - EmergencyDocument4 pagesKing Abdulaziz Medical Cities (National Guard Hospitals) : Generic Clinical Checklist Area - EmergencyZhary AzarNo ratings yet
- Antepartum-Haemorrhage APHDocument9 pagesAntepartum-Haemorrhage APHAjoy DasNo ratings yet
- Generic Clinical Checklist Area - Labour & DeliveryDocument3 pagesGeneric Clinical Checklist Area - Labour & DeliveryMigz CortesNo ratings yet
- (New) Case Study FormatDocument7 pages(New) Case Study FormatSophia Sweet SantosNo ratings yet
- General Assessment TemplateDocument8 pagesGeneral Assessment TemplateBob HopeNo ratings yet
- Medical Surgical Nursing (1) Clinical TrainingDocument21 pagesMedical Surgical Nursing (1) Clinical TrainingAya ElgharbawyNo ratings yet
- Head and Neck PDFDocument274 pagesHead and Neck PDFRakesh Jadhav100% (1)
- Clinical Portfolio Name: Armeen Amin ENROLLMENT NO. 4-4/2019/001 BSCN Year Ii Group A Faculty Name: Ms. Roma JosephDocument15 pagesClinical Portfolio Name: Armeen Amin ENROLLMENT NO. 4-4/2019/001 BSCN Year Ii Group A Faculty Name: Ms. Roma JosephArmeen AminNo ratings yet
- ESMO Prostate 2023Document75 pagesESMO Prostate 2023shokoNo ratings yet
- 5th Mbbs Med Osce 2014... KeshDocument29 pages5th Mbbs Med Osce 2014... Keshaboje ochekwuNo ratings yet
- End of 4 Year OSCE - SurgeryDocument53 pagesEnd of 4 Year OSCE - SurgerySyed Irfan ArifNo ratings yet
- Pre Operative Preparation and Optimization of Cardiac SurgicalDocument40 pagesPre Operative Preparation and Optimization of Cardiac SurgicalNeethu ANo ratings yet
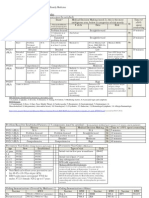
- Thoracic Surgery ManualDocument63 pagesThoracic Surgery ManualAhmed Abd El HamedNo ratings yet
- Diana Pefbrianti, S.Kep., NS., M.KepDocument33 pagesDiana Pefbrianti, S.Kep., NS., M.KepMursidah faNo ratings yet
- Fex 2007.1Document18 pagesFex 2007.1j.jk.jk.17No ratings yet
- Acute Back Pain: Evidence Based ApproachDocument23 pagesAcute Back Pain: Evidence Based ApproachOmar MidaniNo ratings yet
- 2008 High Risk Ob Us GuidelinesDocument15 pages2008 High Risk Ob Us GuidelinesCristina DruzianNo ratings yet
- Book-for - A دوسية من دكتور المقاصدDocument63 pagesBook-for - A دوسية من دكتور المقاصدAli Toma HmedatNo ratings yet
- 5 OSCE-IV-2009 كفاءةDocument7 pages5 OSCE-IV-2009 كفاءةBayan MohammedNo ratings yet
- Internal Medicine - Promotion Exam Blueprint v.2Document6 pagesInternal Medicine - Promotion Exam Blueprint v.2Naz Al-ShahraniNo ratings yet
- Final Part 3 Topic ListDocument11 pagesFinal Part 3 Topic ListHenrietta OlogoNo ratings yet
- l1 - Primary Eye CareDocument6 pagesl1 - Primary Eye Careteamtruth50No ratings yet
- 50 Cases in CardiologyDocument253 pages50 Cases in CardiologyEleonora DraganNo ratings yet
- فحوصات تمريض حلوان مارس ٢٤Document92 pagesفحوصات تمريض حلوان مارس ٢٤hussineNo ratings yet
- OMD411T - Oral Medicine 1Document117 pagesOMD411T - Oral Medicine 1Noura Rihan100% (1)
- Question Paper GroupsDocument3 pagesQuestion Paper GroupsAlpha DevilNo ratings yet
- Program Pendidikan Ilmu Kesehatan AnakDocument16 pagesProgram Pendidikan Ilmu Kesehatan AnakAndaNo ratings yet
- Congenital CataractsDocument123 pagesCongenital CataractsRizqy AbdullahNo ratings yet
- Year 4 - Clinical Skills Sign-Off Sheet PDFDocument2 pagesYear 4 - Clinical Skills Sign-Off Sheet PDFShandev IndoiNo ratings yet
- NCLEX ExamDocument26 pagesNCLEX ExamNaufal Fadli AmzarNo ratings yet
- Womens Health Blighted OvumDocument20 pagesWomens Health Blighted OvumherlinaNo ratings yet
- Natural History and Outcome of Optic Pathway Gliomas in ChildrenDocument7 pagesNatural History and Outcome of Optic Pathway Gliomas in ChildrenCamilo Benavides BurbanoNo ratings yet
- Liver Diseases by SlidesgoDocument74 pagesLiver Diseases by SlidesgoKennie RamirezNo ratings yet
- 002OSCE SlideShowDocument113 pages002OSCE SlideShowkbNo ratings yet
- Fex 2007.2Document15 pagesFex 2007.2j.jk.jk.17No ratings yet
- Quality Control in Endoscopy Unit: Safety Considerations For The PatientDocument13 pagesQuality Control in Endoscopy Unit: Safety Considerations For The PatientPamela PampamNo ratings yet
- UEMS 2013.18 Annex 1 ETR Anaesthesiology SyllabusDocument31 pagesUEMS 2013.18 Annex 1 ETR Anaesthesiology SyllabusAndradaLavricNo ratings yet
- Part 1Document58 pagesPart 1Abdulrahman KatibNo ratings yet
- PediaDocument6 pagesPediaAaron Joshua PobreNo ratings yet
- دمج1 mergedDocument94 pagesدمج1 mergedChew2020No ratings yet
- FamilyDocument2 pagesFamilyAmitShettyNo ratings yet
- DocumentDocument8 pagesDocumentSakinah NuridaNo ratings yet
- Heath Day 4 Care Plan 3Document12 pagesHeath Day 4 Care Plan 3api-639508852No ratings yet
- Orientation, History Taking and ExaminationDocument77 pagesOrientation, History Taking and ExaminationMuhammad AwaisNo ratings yet
- Paediatrics: Lab Medicineincluding Imaging Misc - Derma, Pub Health, ResearchDocument3 pagesPaediatrics: Lab Medicineincluding Imaging Misc - Derma, Pub Health, ResearchSohail KhanNo ratings yet
- Paediatric Examination Handbook 2015Document66 pagesPaediatric Examination Handbook 2015Ulfa Rahmadanti SetiawanNo ratings yet
- MCQ MRCSDocument181 pagesMCQ MRCSAmr Sameer100% (16)
- 03 OSCE SlideShowDocument113 pages03 OSCE SlideShowMohamed FlefelNo ratings yet
- Guide to Pediatric Urology and Surgery in Clinical PracticeFrom EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNo ratings yet
- Qual Res ProposalDocument1 pageQual Res ProposalDME LUMHSNo ratings yet
- Qual Res AdvertisemnetDocument2 pagesQual Res AdvertisemnetDME LUMHSNo ratings yet
- UHS - Proposed New CurriculumDocument4 pagesUHS - Proposed New CurriculumDME LUMHSNo ratings yet
- Workplace Based Assessment - Tools To Assess Competencies in A CliDocument6 pagesWorkplace Based Assessment - Tools To Assess Competencies in A CliDME LUMHSNo ratings yet
- January 2022Document25 pagesJanuary 2022Athula Dias NagahawatteNo ratings yet
- Layeredchristmastreeornament FordownloadDocument2 pagesLayeredchristmastreeornament FordownloadPilar Urendes VílchezNo ratings yet
- Ale Jan 2023 - ScheduleDocument6 pagesAle Jan 2023 - ScheduleBenjie LatrizNo ratings yet
- Topic Test Series: Physics 2021-2022Document28 pagesTopic Test Series: Physics 2021-2022Priyanka SomkuwarNo ratings yet
- Appendix 2D Major Equipment ListDocument7 pagesAppendix 2D Major Equipment ListftriwahyudiNo ratings yet
- BSMLS2A - Candelasa - Activity 2 - BiochemistryDocument3 pagesBSMLS2A - Candelasa - Activity 2 - BiochemistryJohn CandelasaNo ratings yet
- Input Devices PresentationDocument34 pagesInput Devices PresentationDjohn SmithNo ratings yet
- 2018SU B.SC Chemistry SyllabusDocument22 pages2018SU B.SC Chemistry Syllabussachin81185No ratings yet
- Weld Crawler BrochureDocument2 pagesWeld Crawler BrochureEdgardo José Tamaronis LeonettNo ratings yet
- Drug Study (Simvastatin)Document2 pagesDrug Study (Simvastatin)Julianne Jeaven Bumanglag LimNo ratings yet
- DFT Study of CO2 and H2O Co-Adsorption On CarbonDocument17 pagesDFT Study of CO2 and H2O Co-Adsorption On CarbonRafael Ricardo Celin ManceraNo ratings yet
- Cromatografi e TextDocument8 pagesCromatografi e TextRaunciucGianinaNo ratings yet
- Style Guidelines - Powered by GameSparks PDFDocument20 pagesStyle Guidelines - Powered by GameSparks PDFJosé María RomeroNo ratings yet
- Halong Bay and Hanoi 5 Days PDFDocument3 pagesHalong Bay and Hanoi 5 Days PDFmaheshnavamiNo ratings yet
- Bridon Oil and GasDocument48 pagesBridon Oil and GasmkccmNo ratings yet
- Case StudyDocument3 pagesCase Study-No ratings yet
- 2006 2008 Cbf1000 A 10 Clutch Starter ClutchDocument34 pages2006 2008 Cbf1000 A 10 Clutch Starter ClutchMurariu IonutNo ratings yet
- Pashu Prahari April To June MagzineDocument129 pagesPashu Prahari April To June MagzinesumNo ratings yet
- CRG Ambhit CapitalDocument25 pagesCRG Ambhit Capitalsidhanti26No ratings yet
- Lichfield Sutton Coldfield Birmingham Long Bridge RedditchDocument4 pagesLichfield Sutton Coldfield Birmingham Long Bridge RedditchLouisMichaelNo ratings yet
- Chpro Instructions NaDocument1 pageChpro Instructions NaBrandon León ArroyoNo ratings yet
- Profile Radiography Article Estimationof CorrosionDocument10 pagesProfile Radiography Article Estimationof Corrosioncoolguy12345No ratings yet
- cfd1 IntroDocument6 pagescfd1 IntrowhateverNo ratings yet
- Complete Block DesignsDocument80 pagesComplete Block DesignsTaddese GashawNo ratings yet
- Workover Well Control Rev 1 PDFDocument197 pagesWorkover Well Control Rev 1 PDFmoussa mrzgNo ratings yet
- Pro Tip Catalogue 4 07Document28 pagesPro Tip Catalogue 4 07notengofffNo ratings yet
- Office Automation LabDocument36 pagesOffice Automation Labvidyanjali collegeNo ratings yet
- Pharmaceutical Analysis (Lab) Bulk/Tap/Apparent Density and Angle of ReposeDocument17 pagesPharmaceutical Analysis (Lab) Bulk/Tap/Apparent Density and Angle of ReposemasorNo ratings yet