
Tian Chan
Tian Chan
You might also like
- Thời gian làm bài: 60 phút không kể thời gian phát đềDocument11 pagesThời gian làm bài: 60 phút không kể thời gian phát đềLan Anh TạNo ratings yet
- PAPER (ENG) - Stimulation of Sucking and Swallowing To Promote Oral Feeding in Premature InfantsDocument3 pagesPAPER (ENG) - Stimulation of Sucking and Swallowing To Promote Oral Feeding in Premature InfantsAldo Hip NaranjoNo ratings yet
- Chain Conveyors 150508Document16 pagesChain Conveyors 150508MarcNo ratings yet
- The Effectiveness of An Oral Sensorimotor Stimulation Protocol For The Early Achievement of Exclusive Oral Feeding in Premature Infants A RandomizedDocument14 pagesThe Effectiveness of An Oral Sensorimotor Stimulation Protocol For The Early Achievement of Exclusive Oral Feeding in Premature Infants A RandomizedJUAN CARLOSNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument5 pagesInternational Journal of Pediatric OtorhinolaryngologyFarah PramestyNo ratings yet
- RCT Deepa Negi Et AlDocument6 pagesRCT Deepa Negi Et Alnadya gratiaNo ratings yet
- BBLR 2Document6 pagesBBLR 2refiNo ratings yet
- The Effects of Premature Infant Oral Motor Intervention (PIOMI) On Oral Feeding of Preterm Infants - A Randomized Clinical TrialDocument8 pagesThe Effects of Premature Infant Oral Motor Intervention (PIOMI) On Oral Feeding of Preterm Infants - A Randomized Clinical TrialAndreas Arie WidiadiaksaNo ratings yet
- Fucileetal 02Document7 pagesFucileetal 02iimNo ratings yet
- Effect NeurosensoryDocument5 pagesEffect NeurosensoryDwi Suci AsrianiNo ratings yet
- 1 s20 s0022347602000732 MainDocument7 pages1 s20 s0022347602000732 MainThainaNo ratings yet
- The Effect of Preoperative Fasting To Postoperative NauseaDocument7 pagesThe Effect of Preoperative Fasting To Postoperative NauseasantiNo ratings yet
- Cho 2016Document9 pagesCho 2016Irfan FauziNo ratings yet
- 1 s2.0 S1875957222000195 MainDocument7 pages1 s2.0 S1875957222000195 MainElenaNo ratings yet
- EJHC Volume 13 Issue 3 Pages 1322-1334Document13 pagesEJHC Volume 13 Issue 3 Pages 1322-1334Andi SulvanNo ratings yet
- Intervencion Temprana SuccionDocument13 pagesIntervencion Temprana Succionjulianamd87No ratings yet
- Jurnal A ComparisonDocument8 pagesJurnal A ComparisonAgatha GeraldyneNo ratings yet
- Manajemen NyeriDocument8 pagesManajemen Nyeriagung yulisaputraNo ratings yet
- The Effectiveness of Quarter Turn From Prone in Maintaining Respiratory Function in Premature InfantsDocument7 pagesThe Effectiveness of Quarter Turn From Prone in Maintaining Respiratory Function in Premature InfantsAkmal ThariqNo ratings yet
- A Quasi Experimental Study To Evaluate The Effect of Prefeeding Oral Stimulation Program On Oral Feeding Skills Among Preterm Infants in Selected Hospitals, PunjabDocument29 pagesA Quasi Experimental Study To Evaluate The Effect of Prefeeding Oral Stimulation Program On Oral Feeding Skills Among Preterm Infants in Selected Hospitals, PunjabEditor IJTSRD100% (1)
- Assess The Effectiveness of Sensory Nursing Interventions On Neonatal Reflex and Reactivity Among Preterm Infants in Selected Setting, Nagercoil, K.K. DistrictDocument12 pagesAssess The Effectiveness of Sensory Nursing Interventions On Neonatal Reflex and Reactivity Among Preterm Infants in Selected Setting, Nagercoil, K.K. DistrictImpact JournalsNo ratings yet
- Jurnal NeonatusDocument41 pagesJurnal NeonatusDesmiyati AdoeNo ratings yet
- Chantal. Management of Oral Feeding Challenges in Neonatal Intensive Care Units NICUs A National Survey in ChinaDocument7 pagesChantal. Management of Oral Feeding Challenges in Neonatal Intensive Care Units NICUs A National Survey in ChinaJAVIERA BELEN ROMERO DURANNo ratings yet
- The Effect of Feeding Rules To Weigh Changing in Childrent: DiscussionDocument1 pageThe Effect of Feeding Rules To Weigh Changing in Childrent: DiscussionsugengNo ratings yet
- JOHOE - Volume 5 - Issue 1 - Pages 13-16Document4 pagesJOHOE - Volume 5 - Issue 1 - Pages 13-16Tô ThuỷNo ratings yet
- 14, Yuni .1111@ijn.12911Document9 pages14, Yuni .1111@ijn.12911Mastifa HanasitaNo ratings yet
- Journal of Pediatric Nursing: Burcu Aykanat Girgin, Duygu GözenDocument7 pagesJournal of Pediatric Nursing: Burcu Aykanat Girgin, Duygu GözenFarah PramestyNo ratings yet
- 30111-Article Text-56479-2-10-20191126Document14 pages30111-Article Text-56479-2-10-20191126RahmidamiliyntNo ratings yet
- Menoufia Med J 2021 34 1 226 230 EngDocument5 pagesMenoufia Med J 2021 34 1 226 230 EngAndi SulvanNo ratings yet
- Sezer 2020Document1 pageSezer 2020KarlaPadrelananNo ratings yet
- Midwifery: SciencedirectDocument10 pagesMidwifery: SciencedirectFarin MauliaNo ratings yet
- 56 1-Gunay Original 10 2Document9 pages56 1-Gunay Original 10 2Mbah AbuNo ratings yet
- Efectos Del MasageDocument6 pagesEfectos Del MasageIsis SanzNo ratings yet
- Role of Gastric Lavage in Newborn With Meconium Stained Amniotic Fluid:a Randomized Controlled TrailDocument3 pagesRole of Gastric Lavage in Newborn With Meconium Stained Amniotic Fluid:a Randomized Controlled TrailtriaanggareniNo ratings yet
- Effect of CupDocument9 pagesEffect of CupInés Valero ArredondoNo ratings yet
- Clinical Outcomes of Snuggle Up Position Using Positioning Aids For Preterm (27-32 Weeks) InfantsDocument6 pagesClinical Outcomes of Snuggle Up Position Using Positioning Aids For Preterm (27-32 Weeks) InfantsMastifa HanasitaNo ratings yet
- DescargaDocument5 pagesDescargavaleria posadaNo ratings yet
- CONFINEMENTDocument12 pagesCONFINEMENTfyzazilaNo ratings yet
- Fucile2018 Ver WordDocument8 pagesFucile2018 Ver WordAries CamiNo ratings yet
- Journal Club PresentationDocument15 pagesJournal Club PresentationAGERI PUSHPALATHANo ratings yet
- Nonnutritive Sucking Evaluation in Preterm Newborns and The Start of OralDocument5 pagesNonnutritive Sucking Evaluation in Preterm Newborns and The Start of Oralgisell buenoNo ratings yet
- Yuni Girgin2018Document9 pagesYuni Girgin2018Mastifa HanasitaNo ratings yet
- International Journal of Gynecology and ObstetricsDocument4 pagesInternational Journal of Gynecology and ObstetricslisavalentinsNo ratings yet
- Effect of Back Massage On Lactation Amon PDFDocument9 pagesEffect of Back Massage On Lactation Amon PDFfemyNo ratings yet
- Research Article Skin-to-Skin Care by Mother vs. Father For Preterm Neonatal Pain: A Randomized Control Trial (ENVIRON Trial)Document6 pagesResearch Article Skin-to-Skin Care by Mother vs. Father For Preterm Neonatal Pain: A Randomized Control Trial (ENVIRON Trial)nadia kurniaNo ratings yet
- (2021) Effects of Swallowing Training and Follow-Up On The Problems Associated WithDocument13 pages(2021) Effects of Swallowing Training and Follow-Up On The Problems Associated With王宇萱No ratings yet
- 1 s2.0 S0163638313000775 MainDocument8 pages1 s2.0 S0163638313000775 MaindrorgarbiNo ratings yet
- Application of Puerperal Healthy of Optimization of Postpartum Mother Knowledges That Given Effleurage Relaxation MassageDocument4 pagesApplication of Puerperal Healthy of Optimization of Postpartum Mother Knowledges That Given Effleurage Relaxation MassageInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- DBF and AKUPDocument10 pagesDBF and AKUPwidad syairoziNo ratings yet
- Issues Related To Breastfeeding in The First Six Months of Life in An Urban Tertiary Care HospitalDocument7 pagesIssues Related To Breastfeeding in The First Six Months of Life in An Urban Tertiary Care HospitalVanyaNo ratings yet
- Niu 2022Document12 pagesNiu 2022Javiera Abigail Espinoza AlvarezNo ratings yet
- Hartati 2019 J. Phys. Conf. Ser. 1351 012091Document7 pagesHartati 2019 J. Phys. Conf. Ser. 1351 012091Derison MarsinovaNo ratings yet
- Effect of Yoga On Duration of The Second Stage of Labor and Perineal Rupture in Primigravida MothersDocument5 pagesEffect of Yoga On Duration of The Second Stage of Labor and Perineal Rupture in Primigravida MothersDellaTaurusNo ratings yet
- ProneDocument8 pagesPronesophiaNo ratings yet
- 2633-Article Text-21183-2-10-20201019Document4 pages2633-Article Text-21183-2-10-20201019ariani khikmatul mazidahNo ratings yet
- Swinging, Sucking (5S'S) Terhadap Skala Nyeri DanDocument7 pagesSwinging, Sucking (5S'S) Terhadap Skala Nyeri DanMakhrufi M.A.S. ArdiantoNo ratings yet
- ABSTRACTDocument1 pageABSTRACTHarrison RumeNo ratings yet
- Oral Stimulation Techniques in Preterm IDocument7 pagesOral Stimulation Techniques in Preterm ITrisialdilla RevaniaNo ratings yet
- YanyanDocument7 pagesYanyansigitdwimulyoNo ratings yet
- Digestive and Liver DiseaseDocument5 pagesDigestive and Liver DiseasexwingmanNo ratings yet
- Nurturing a Healthy Generation of Children: Research Gaps and Opportunities: 91st Nestlé Nutrition Institute Workshop, Manila, March 2018From EverandNurturing a Healthy Generation of Children: Research Gaps and Opportunities: 91st Nestlé Nutrition Institute Workshop, Manila, March 2018No ratings yet
- Protein in Neonatal and Infant Nutrition: Recent Updates: 86th Nestlé Nutrition Institute Workshop, Beijing, May 2015From EverandProtein in Neonatal and Infant Nutrition: Recent Updates: 86th Nestlé Nutrition Institute Workshop, Beijing, May 2015No ratings yet
- JurnalDocument12 pagesJurnalTrisi Aldilla RevaniaNo ratings yet
- Zoster Virus Dalam Nelsen Textbook of Pediatrics 18: Daftar PustakaDocument1 pageZoster Virus Dalam Nelsen Textbook of Pediatrics 18: Daftar PustakaTrisi Aldilla RevaniaNo ratings yet
- Rujukan: Universitas Sumatera UtaraDocument2 pagesRujukan: Universitas Sumatera UtaraTrisi Aldilla RevaniaNo ratings yet
- Primary Care: Whispered Voice Test For Screening For Hearing Impairment in Adults and Children: Systematic ReviewDocument5 pagesPrimary Care: Whispered Voice Test For Screening For Hearing Impairment in Adults and Children: Systematic ReviewTrisi Aldilla RevaniaNo ratings yet
- Lamont Et Al-2011-BJOG An International Journal of Obstetrics & GynaecologyDocument6 pagesLamont Et Al-2011-BJOG An International Journal of Obstetrics & GynaecologyTrisi Aldilla RevaniaNo ratings yet
- Download-Fullpapers-2. Skoring Dvi 1Document8 pagesDownload-Fullpapers-2. Skoring Dvi 1Trisi Aldilla RevaniaNo ratings yet
- Review ArticleDocument10 pagesReview ArticleTrisi Aldilla RevaniaNo ratings yet
- Health Equity: Fury MaulinaDocument15 pagesHealth Equity: Fury MaulinaTrisi Aldilla RevaniaNo ratings yet
- FM 8900 SDocument136 pagesFM 8900 SRomeish KelaartNo ratings yet
- Pamantasan NG Lungsod NG Maynila Intramuros, ManilaDocument2 pagesPamantasan NG Lungsod NG Maynila Intramuros, ManilaWacko AsahanNo ratings yet
- Designing Unstable Landscapes Improvisational Dance Within Cognitive Systems by Marlon Barrios SolanoDocument12 pagesDesigning Unstable Landscapes Improvisational Dance Within Cognitive Systems by Marlon Barrios SolanoMarlon Barrios SolanoNo ratings yet
- Barcenas Et Al 2011 Molecular Systematics of CactaceaeDocument20 pagesBarcenas Et Al 2011 Molecular Systematics of CactaceaeAndrés FrankowNo ratings yet
- L7042GSI: VHP Series Gas Engine Extender SeriesDocument2 pagesL7042GSI: VHP Series Gas Engine Extender SeriesferyNo ratings yet
- Junos Release Notes 12.3r11 PDFDocument390 pagesJunos Release Notes 12.3r11 PDFHellman Roman Pinzon GarciaNo ratings yet
- Catia Important Interview QuestionsDocument40 pagesCatia Important Interview QuestionsHarshwardhan Singh0% (1)
- Grobs Basic Electronics 13Th Edition Mitchel E Schultz Full ChapterDocument51 pagesGrobs Basic Electronics 13Th Edition Mitchel E Schultz Full Chapterbrandon.henderson521100% (8)
- Lesson Plan - Sexual ReproductionDocument3 pagesLesson Plan - Sexual ReproductionHazael Jane BalaisNo ratings yet
- Safety Data Sheet: Section 1. IdentificationDocument11 pagesSafety Data Sheet: Section 1. IdentificationRam1zNo ratings yet
- Molykote P40 Grease For Marine IndustryDocument1 pageMolykote P40 Grease For Marine IndustryProject Sales CorpNo ratings yet
- Eco Comport AmDocument10 pagesEco Comport AmIHNo ratings yet
- Marine Propulsion System Failures-A Review: Marine Science and EngineeringDocument14 pagesMarine Propulsion System Failures-A Review: Marine Science and EngineeringDavid NuñezNo ratings yet
- Modified GCC Fillers in Printing Paper ProductionDocument7 pagesModified GCC Fillers in Printing Paper ProductionPenkinNo ratings yet
- Say NO To PVC Concrete Spacers PDFDocument1 pageSay NO To PVC Concrete Spacers PDFSOURAV RANJAN KHANRANo ratings yet
- Xpert R410a Onoff Ar Na 230613Document62 pagesXpert R410a Onoff Ar Na 230613Wilson Segovia CarrascoNo ratings yet
- Green Sustainable Airports The Deployment of RenewDocument5 pagesGreen Sustainable Airports The Deployment of Renewcandra trimandokoNo ratings yet
- Stochastic ProcessDocument610 pagesStochastic ProcesshopanzNo ratings yet
- Seamo Paper - F - 2021Document8 pagesSeamo Paper - F - 2021Bá PhongNo ratings yet
- Lo3. Provide Information and Advice On A Destination, Product or Services Available at The DestinationDocument14 pagesLo3. Provide Information and Advice On A Destination, Product or Services Available at The Destinationverirowena28No ratings yet
- MP 12th Five Year PlanDocument599 pagesMP 12th Five Year Planphilodog100% (2)
- Romeo and Juliet Movie ComparisonDocument2 pagesRomeo and Juliet Movie Comparisonameanie68100% (2)
- BEYOND THE CD: How SACD Won The WarDocument76 pagesBEYOND THE CD: How SACD Won The WarenergiculNo ratings yet
- Gasni Kaloriferi RoburDocument32 pagesGasni Kaloriferi RoburMarkoni MarkonicNo ratings yet
- Theory and Application For The Scanning Tunneling MicroscopeDocument4 pagesTheory and Application For The Scanning Tunneling MicroscopeIgor LukacevicNo ratings yet
- The Keystone Triad: I. Anatomy, Phylogenetics, and Clinical ReferencesDocument21 pagesThe Keystone Triad: I. Anatomy, Phylogenetics, and Clinical ReferencesSelvaArockiamNo ratings yet
- Alternating Current and Direct Current PDFDocument5 pagesAlternating Current and Direct Current PDFHafiz HamzaNo ratings yet
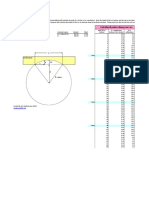
- Arc Layout Calculator: Calculated Points Along Your Arc Enter These ValuesDocument1 pageArc Layout Calculator: Calculated Points Along Your Arc Enter These ValuesPaco PacoNo ratings yet

































































































Download as pdf or txt
You might also like
- Thời gian làm bài: 60 phút không kể thời gian phát đềDocument11 pagesThời gian làm bài: 60 phút không kể thời gian phát đềLan Anh TạNo ratings yet
- PAPER (ENG) - Stimulation of Sucking and Swallowing To Promote Oral Feeding in Premature InfantsDocument3 pagesPAPER (ENG) - Stimulation of Sucking and Swallowing To Promote Oral Feeding in Premature InfantsAldo Hip NaranjoNo ratings yet
- Chain Conveyors 150508Document16 pagesChain Conveyors 150508MarcNo ratings yet
- The Effectiveness of An Oral Sensorimotor Stimulation Protocol For The Early Achievement of Exclusive Oral Feeding in Premature Infants A RandomizedDocument14 pagesThe Effectiveness of An Oral Sensorimotor Stimulation Protocol For The Early Achievement of Exclusive Oral Feeding in Premature Infants A RandomizedJUAN CARLOSNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument5 pagesInternational Journal of Pediatric OtorhinolaryngologyFarah PramestyNo ratings yet
- RCT Deepa Negi Et AlDocument6 pagesRCT Deepa Negi Et Alnadya gratiaNo ratings yet
- BBLR 2Document6 pagesBBLR 2refiNo ratings yet
- The Effects of Premature Infant Oral Motor Intervention (PIOMI) On Oral Feeding of Preterm Infants - A Randomized Clinical TrialDocument8 pagesThe Effects of Premature Infant Oral Motor Intervention (PIOMI) On Oral Feeding of Preterm Infants - A Randomized Clinical TrialAndreas Arie WidiadiaksaNo ratings yet
- Fucileetal 02Document7 pagesFucileetal 02iimNo ratings yet
- Effect NeurosensoryDocument5 pagesEffect NeurosensoryDwi Suci AsrianiNo ratings yet
- 1 s20 s0022347602000732 MainDocument7 pages1 s20 s0022347602000732 MainThainaNo ratings yet
- The Effect of Preoperative Fasting To Postoperative NauseaDocument7 pagesThe Effect of Preoperative Fasting To Postoperative NauseasantiNo ratings yet
- Cho 2016Document9 pagesCho 2016Irfan FauziNo ratings yet
- 1 s2.0 S1875957222000195 MainDocument7 pages1 s2.0 S1875957222000195 MainElenaNo ratings yet
- EJHC Volume 13 Issue 3 Pages 1322-1334Document13 pagesEJHC Volume 13 Issue 3 Pages 1322-1334Andi SulvanNo ratings yet
- Intervencion Temprana SuccionDocument13 pagesIntervencion Temprana Succionjulianamd87No ratings yet
- Jurnal A ComparisonDocument8 pagesJurnal A ComparisonAgatha GeraldyneNo ratings yet
- Manajemen NyeriDocument8 pagesManajemen Nyeriagung yulisaputraNo ratings yet
- The Effectiveness of Quarter Turn From Prone in Maintaining Respiratory Function in Premature InfantsDocument7 pagesThe Effectiveness of Quarter Turn From Prone in Maintaining Respiratory Function in Premature InfantsAkmal ThariqNo ratings yet
- A Quasi Experimental Study To Evaluate The Effect of Prefeeding Oral Stimulation Program On Oral Feeding Skills Among Preterm Infants in Selected Hospitals, PunjabDocument29 pagesA Quasi Experimental Study To Evaluate The Effect of Prefeeding Oral Stimulation Program On Oral Feeding Skills Among Preterm Infants in Selected Hospitals, PunjabEditor IJTSRD100% (1)
- Assess The Effectiveness of Sensory Nursing Interventions On Neonatal Reflex and Reactivity Among Preterm Infants in Selected Setting, Nagercoil, K.K. DistrictDocument12 pagesAssess The Effectiveness of Sensory Nursing Interventions On Neonatal Reflex and Reactivity Among Preterm Infants in Selected Setting, Nagercoil, K.K. DistrictImpact JournalsNo ratings yet
- Jurnal NeonatusDocument41 pagesJurnal NeonatusDesmiyati AdoeNo ratings yet
- Chantal. Management of Oral Feeding Challenges in Neonatal Intensive Care Units NICUs A National Survey in ChinaDocument7 pagesChantal. Management of Oral Feeding Challenges in Neonatal Intensive Care Units NICUs A National Survey in ChinaJAVIERA BELEN ROMERO DURANNo ratings yet
- The Effect of Feeding Rules To Weigh Changing in Childrent: DiscussionDocument1 pageThe Effect of Feeding Rules To Weigh Changing in Childrent: DiscussionsugengNo ratings yet
- JOHOE - Volume 5 - Issue 1 - Pages 13-16Document4 pagesJOHOE - Volume 5 - Issue 1 - Pages 13-16Tô ThuỷNo ratings yet
- 14, Yuni .1111@ijn.12911Document9 pages14, Yuni .1111@ijn.12911Mastifa HanasitaNo ratings yet
- Journal of Pediatric Nursing: Burcu Aykanat Girgin, Duygu GözenDocument7 pagesJournal of Pediatric Nursing: Burcu Aykanat Girgin, Duygu GözenFarah PramestyNo ratings yet
- 30111-Article Text-56479-2-10-20191126Document14 pages30111-Article Text-56479-2-10-20191126RahmidamiliyntNo ratings yet
- Menoufia Med J 2021 34 1 226 230 EngDocument5 pagesMenoufia Med J 2021 34 1 226 230 EngAndi SulvanNo ratings yet
- Sezer 2020Document1 pageSezer 2020KarlaPadrelananNo ratings yet
- Midwifery: SciencedirectDocument10 pagesMidwifery: SciencedirectFarin MauliaNo ratings yet
- 56 1-Gunay Original 10 2Document9 pages56 1-Gunay Original 10 2Mbah AbuNo ratings yet
- Efectos Del MasageDocument6 pagesEfectos Del MasageIsis SanzNo ratings yet
- Role of Gastric Lavage in Newborn With Meconium Stained Amniotic Fluid:a Randomized Controlled TrailDocument3 pagesRole of Gastric Lavage in Newborn With Meconium Stained Amniotic Fluid:a Randomized Controlled TrailtriaanggareniNo ratings yet
- Effect of CupDocument9 pagesEffect of CupInés Valero ArredondoNo ratings yet
- Clinical Outcomes of Snuggle Up Position Using Positioning Aids For Preterm (27-32 Weeks) InfantsDocument6 pagesClinical Outcomes of Snuggle Up Position Using Positioning Aids For Preterm (27-32 Weeks) InfantsMastifa HanasitaNo ratings yet
- DescargaDocument5 pagesDescargavaleria posadaNo ratings yet
- CONFINEMENTDocument12 pagesCONFINEMENTfyzazilaNo ratings yet
- Fucile2018 Ver WordDocument8 pagesFucile2018 Ver WordAries CamiNo ratings yet
- Journal Club PresentationDocument15 pagesJournal Club PresentationAGERI PUSHPALATHANo ratings yet
- Nonnutritive Sucking Evaluation in Preterm Newborns and The Start of OralDocument5 pagesNonnutritive Sucking Evaluation in Preterm Newborns and The Start of Oralgisell buenoNo ratings yet
- Yuni Girgin2018Document9 pagesYuni Girgin2018Mastifa HanasitaNo ratings yet
- International Journal of Gynecology and ObstetricsDocument4 pagesInternational Journal of Gynecology and ObstetricslisavalentinsNo ratings yet
- Effect of Back Massage On Lactation Amon PDFDocument9 pagesEffect of Back Massage On Lactation Amon PDFfemyNo ratings yet
- Research Article Skin-to-Skin Care by Mother vs. Father For Preterm Neonatal Pain: A Randomized Control Trial (ENVIRON Trial)Document6 pagesResearch Article Skin-to-Skin Care by Mother vs. Father For Preterm Neonatal Pain: A Randomized Control Trial (ENVIRON Trial)nadia kurniaNo ratings yet
- (2021) Effects of Swallowing Training and Follow-Up On The Problems Associated WithDocument13 pages(2021) Effects of Swallowing Training and Follow-Up On The Problems Associated With王宇萱No ratings yet
- 1 s2.0 S0163638313000775 MainDocument8 pages1 s2.0 S0163638313000775 MaindrorgarbiNo ratings yet
- Application of Puerperal Healthy of Optimization of Postpartum Mother Knowledges That Given Effleurage Relaxation MassageDocument4 pagesApplication of Puerperal Healthy of Optimization of Postpartum Mother Knowledges That Given Effleurage Relaxation MassageInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- DBF and AKUPDocument10 pagesDBF and AKUPwidad syairoziNo ratings yet
- Issues Related To Breastfeeding in The First Six Months of Life in An Urban Tertiary Care HospitalDocument7 pagesIssues Related To Breastfeeding in The First Six Months of Life in An Urban Tertiary Care HospitalVanyaNo ratings yet
- Niu 2022Document12 pagesNiu 2022Javiera Abigail Espinoza AlvarezNo ratings yet
- Hartati 2019 J. Phys. Conf. Ser. 1351 012091Document7 pagesHartati 2019 J. Phys. Conf. Ser. 1351 012091Derison MarsinovaNo ratings yet
- Effect of Yoga On Duration of The Second Stage of Labor and Perineal Rupture in Primigravida MothersDocument5 pagesEffect of Yoga On Duration of The Second Stage of Labor and Perineal Rupture in Primigravida MothersDellaTaurusNo ratings yet
- ProneDocument8 pagesPronesophiaNo ratings yet
- 2633-Article Text-21183-2-10-20201019Document4 pages2633-Article Text-21183-2-10-20201019ariani khikmatul mazidahNo ratings yet
- Swinging, Sucking (5S'S) Terhadap Skala Nyeri DanDocument7 pagesSwinging, Sucking (5S'S) Terhadap Skala Nyeri DanMakhrufi M.A.S. ArdiantoNo ratings yet
- ABSTRACTDocument1 pageABSTRACTHarrison RumeNo ratings yet
- Oral Stimulation Techniques in Preterm IDocument7 pagesOral Stimulation Techniques in Preterm ITrisialdilla RevaniaNo ratings yet
- YanyanDocument7 pagesYanyansigitdwimulyoNo ratings yet
- Digestive and Liver DiseaseDocument5 pagesDigestive and Liver DiseasexwingmanNo ratings yet
- Nurturing a Healthy Generation of Children: Research Gaps and Opportunities: 91st Nestlé Nutrition Institute Workshop, Manila, March 2018From EverandNurturing a Healthy Generation of Children: Research Gaps and Opportunities: 91st Nestlé Nutrition Institute Workshop, Manila, March 2018No ratings yet
- Protein in Neonatal and Infant Nutrition: Recent Updates: 86th Nestlé Nutrition Institute Workshop, Beijing, May 2015From EverandProtein in Neonatal and Infant Nutrition: Recent Updates: 86th Nestlé Nutrition Institute Workshop, Beijing, May 2015No ratings yet
- JurnalDocument12 pagesJurnalTrisi Aldilla RevaniaNo ratings yet
- Zoster Virus Dalam Nelsen Textbook of Pediatrics 18: Daftar PustakaDocument1 pageZoster Virus Dalam Nelsen Textbook of Pediatrics 18: Daftar PustakaTrisi Aldilla RevaniaNo ratings yet
- Rujukan: Universitas Sumatera UtaraDocument2 pagesRujukan: Universitas Sumatera UtaraTrisi Aldilla RevaniaNo ratings yet
- Primary Care: Whispered Voice Test For Screening For Hearing Impairment in Adults and Children: Systematic ReviewDocument5 pagesPrimary Care: Whispered Voice Test For Screening For Hearing Impairment in Adults and Children: Systematic ReviewTrisi Aldilla RevaniaNo ratings yet
- Lamont Et Al-2011-BJOG An International Journal of Obstetrics & GynaecologyDocument6 pagesLamont Et Al-2011-BJOG An International Journal of Obstetrics & GynaecologyTrisi Aldilla RevaniaNo ratings yet
- Download-Fullpapers-2. Skoring Dvi 1Document8 pagesDownload-Fullpapers-2. Skoring Dvi 1Trisi Aldilla RevaniaNo ratings yet
- Review ArticleDocument10 pagesReview ArticleTrisi Aldilla RevaniaNo ratings yet
- Health Equity: Fury MaulinaDocument15 pagesHealth Equity: Fury MaulinaTrisi Aldilla RevaniaNo ratings yet
- FM 8900 SDocument136 pagesFM 8900 SRomeish KelaartNo ratings yet
- Pamantasan NG Lungsod NG Maynila Intramuros, ManilaDocument2 pagesPamantasan NG Lungsod NG Maynila Intramuros, ManilaWacko AsahanNo ratings yet
- Designing Unstable Landscapes Improvisational Dance Within Cognitive Systems by Marlon Barrios SolanoDocument12 pagesDesigning Unstable Landscapes Improvisational Dance Within Cognitive Systems by Marlon Barrios SolanoMarlon Barrios SolanoNo ratings yet
- Barcenas Et Al 2011 Molecular Systematics of CactaceaeDocument20 pagesBarcenas Et Al 2011 Molecular Systematics of CactaceaeAndrés FrankowNo ratings yet
- L7042GSI: VHP Series Gas Engine Extender SeriesDocument2 pagesL7042GSI: VHP Series Gas Engine Extender SeriesferyNo ratings yet
- Junos Release Notes 12.3r11 PDFDocument390 pagesJunos Release Notes 12.3r11 PDFHellman Roman Pinzon GarciaNo ratings yet
- Catia Important Interview QuestionsDocument40 pagesCatia Important Interview QuestionsHarshwardhan Singh0% (1)
- Grobs Basic Electronics 13Th Edition Mitchel E Schultz Full ChapterDocument51 pagesGrobs Basic Electronics 13Th Edition Mitchel E Schultz Full Chapterbrandon.henderson521100% (8)
- Lesson Plan - Sexual ReproductionDocument3 pagesLesson Plan - Sexual ReproductionHazael Jane BalaisNo ratings yet
- Safety Data Sheet: Section 1. IdentificationDocument11 pagesSafety Data Sheet: Section 1. IdentificationRam1zNo ratings yet
- Molykote P40 Grease For Marine IndustryDocument1 pageMolykote P40 Grease For Marine IndustryProject Sales CorpNo ratings yet
- Eco Comport AmDocument10 pagesEco Comport AmIHNo ratings yet
- Marine Propulsion System Failures-A Review: Marine Science and EngineeringDocument14 pagesMarine Propulsion System Failures-A Review: Marine Science and EngineeringDavid NuñezNo ratings yet
- Modified GCC Fillers in Printing Paper ProductionDocument7 pagesModified GCC Fillers in Printing Paper ProductionPenkinNo ratings yet
- Say NO To PVC Concrete Spacers PDFDocument1 pageSay NO To PVC Concrete Spacers PDFSOURAV RANJAN KHANRANo ratings yet
- Xpert R410a Onoff Ar Na 230613Document62 pagesXpert R410a Onoff Ar Na 230613Wilson Segovia CarrascoNo ratings yet
- Green Sustainable Airports The Deployment of RenewDocument5 pagesGreen Sustainable Airports The Deployment of Renewcandra trimandokoNo ratings yet
- Stochastic ProcessDocument610 pagesStochastic ProcesshopanzNo ratings yet
- Seamo Paper - F - 2021Document8 pagesSeamo Paper - F - 2021Bá PhongNo ratings yet
- Lo3. Provide Information and Advice On A Destination, Product or Services Available at The DestinationDocument14 pagesLo3. Provide Information and Advice On A Destination, Product or Services Available at The Destinationverirowena28No ratings yet
- MP 12th Five Year PlanDocument599 pagesMP 12th Five Year Planphilodog100% (2)
- Romeo and Juliet Movie ComparisonDocument2 pagesRomeo and Juliet Movie Comparisonameanie68100% (2)
- BEYOND THE CD: How SACD Won The WarDocument76 pagesBEYOND THE CD: How SACD Won The WarenergiculNo ratings yet
- Gasni Kaloriferi RoburDocument32 pagesGasni Kaloriferi RoburMarkoni MarkonicNo ratings yet
- Theory and Application For The Scanning Tunneling MicroscopeDocument4 pagesTheory and Application For The Scanning Tunneling MicroscopeIgor LukacevicNo ratings yet
- The Keystone Triad: I. Anatomy, Phylogenetics, and Clinical ReferencesDocument21 pagesThe Keystone Triad: I. Anatomy, Phylogenetics, and Clinical ReferencesSelvaArockiamNo ratings yet
- Alternating Current and Direct Current PDFDocument5 pagesAlternating Current and Direct Current PDFHafiz HamzaNo ratings yet
- Arc Layout Calculator: Calculated Points Along Your Arc Enter These ValuesDocument1 pageArc Layout Calculator: Calculated Points Along Your Arc Enter These ValuesPaco PacoNo ratings yet