Download as pdf or txt
You might also like
- 5-Day Split Lean Gain Program PDFDocument7 pages5-Day Split Lean Gain Program PDFNishant Kumar83% (6)
- Assignment - Medicines Development Process and Good Clinical PracticeDocument2 pagesAssignment - Medicines Development Process and Good Clinical PracticeZornicaBorisovaNo ratings yet
- Ent Exam IsmDocument266 pagesEnt Exam IsmAmit BhadhanaNo ratings yet
- Contemporary Diagnosis and Management of Dental ErosionDocument10 pagesContemporary Diagnosis and Management of Dental ErosionAndreea AddaNo ratings yet
- CV Jenn Sunday 2022Document13 pagesCV Jenn Sunday 2022api-549348346No ratings yet
- Module 4 PROBLEM ORIENTED MEDICAL RECORDDocument15 pagesModule 4 PROBLEM ORIENTED MEDICAL RECORDdarius bautistaNo ratings yet
- Odent, Michel - The Fetus Ejection ReflexDocument2 pagesOdent, Michel - The Fetus Ejection ReflexvicentecarneroNo ratings yet
- Trauma From Occlusion - Periodontal TraumatismDocument14 pagesTrauma From Occlusion - Periodontal TraumatismGrestyasanti WimasanNo ratings yet
- Ebp Head Up 30Document9 pagesEbp Head Up 30La fazaNo ratings yet
- MedicinusDocument64 pagesMedicinusJuandri Pia TorocozzickNo ratings yet
- Oral Surg. Lec.1 (Maxillofacial Trauma)Document39 pagesOral Surg. Lec.1 (Maxillofacial Trauma)ريام الموسويNo ratings yet
- Credit Proposal of Konnect AttapurDocument7 pagesCredit Proposal of Konnect AttapurGavin MathewNo ratings yet
- Risk Factors For Periodontal Diseases 2022Document13 pagesRisk Factors For Periodontal Diseases 2022SnowNo ratings yet
- Controversies in Periodontology PDFDocument2 pagesControversies in Periodontology PDFSrivani PeriNo ratings yet
- 6 MIKROTIA Ade - Unpad Full TextDocument23 pages6 MIKROTIA Ade - Unpad Full TextfakhrenaNo ratings yet
- Persistent and Chronic Diarrhea and Malabsorption - ESPGHAN PDFDocument6 pagesPersistent and Chronic Diarrhea and Malabsorption - ESPGHAN PDFMoises RiveraNo ratings yet
- Antagonistic Effects of Plant Growth Promoting Bacteria Against Bacterial Diseases of Black GramDocument5 pagesAntagonistic Effects of Plant Growth Promoting Bacteria Against Bacterial Diseases of Black GramAcademic JournalNo ratings yet
- Cattle Cheek InfectionDocument10 pagesCattle Cheek InfectionAiaNo ratings yet
- Erythema MultiformeDocument3 pagesErythema MultiformeLindar Rin リンNo ratings yet
- Open Retromuscular Sublay Mesh Repair Versus Laparoscopic Intraperitoneal Onlay Mesh Repair For Ventral Hernias A Randomized Control TrialDocument7 pagesOpen Retromuscular Sublay Mesh Repair Versus Laparoscopic Intraperitoneal Onlay Mesh Repair For Ventral Hernias A Randomized Control TrialAthenaeum Scientific PublishersNo ratings yet
- GCF FinalDocument76 pagesGCF FinalNishtha BaralNo ratings yet
- Full Occlusal Protection - Theory and Practice of Occlusal TherapyDocument10 pagesFull Occlusal Protection - Theory and Practice of Occlusal TherapyHuong KamNo ratings yet
- Imaging of Intracranial InfectionsDocument12 pagesImaging of Intracranial Infectionsrafael rocha novaesNo ratings yet
- Contact Lens Related Complications A Review-1Document20 pagesContact Lens Related Complications A Review-1Astri Dwi ParamitaNo ratings yet
- Haad June 13 2Document14 pagesHaad June 13 2MMdrNo ratings yet
- Microleakage in EndodonticsDocument10 pagesMicroleakage in EndodonticsJAYASOORYAN S P M.D.S. CONSERVATIVE DENTISTRY AND ENDODONTICSNo ratings yet
- TrismusDocument6 pagesTrismusAdityaEdoNo ratings yet
- Cranial Nerve Disorders: Ernest E. WangDocument13 pagesCranial Nerve Disorders: Ernest E. Wangirsyad tsaniNo ratings yet
- Evidence-Based Guidelines MMDocument8 pagesEvidence-Based Guidelines MMAna Luiza ToldoNo ratings yet
- Black Pigmentation in Primary Dentition Case Report and Literature ReviewDocument5 pagesBlack Pigmentation in Primary Dentition Case Report and Literature ReviewlaloNo ratings yet
- Declerck 2011Document4 pagesDeclerck 2011ortodoncia 2022No ratings yet
- Macrophage ICDocument10 pagesMacrophage ICchristian lunaNo ratings yet
- New Perio ClassificationDocument8 pagesNew Perio ClassificationLauraNo ratings yet
- 9789386478122Document15 pages9789386478122ruacondungmanhNo ratings yet
- Oral Path CramDocument10 pagesOral Path CramHarjotBrarNo ratings yet
- Medicine and Dentistry - ALLDocument279 pagesMedicine and Dentistry - ALLKabiru Jega UmarNo ratings yet
- Operkulektomi Herlambang, Devina, Asya, AlinDocument3 pagesOperkulektomi Herlambang, Devina, Asya, AlinHerlambang PrasetyoNo ratings yet
- BIRADS Lexicon and Its Histopathological Corroboration in The Diagnosis of Breast LesionsDocument7 pagesBIRADS Lexicon and Its Histopathological Corroboration in The Diagnosis of Breast LesionsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- PROSTHODONTIC MANAGEMENT OF GERIATRIC PATIENTS (Autosaved) (Autosaved)Document35 pagesPROSTHODONTIC MANAGEMENT OF GERIATRIC PATIENTS (Autosaved) (Autosaved)Shilpa SomanNo ratings yet
- Abstracts From The Global Embolization Sympo 2021 Journal of Vascular and inDocument21 pagesAbstracts From The Global Embolization Sympo 2021 Journal of Vascular and infreedy freedyNo ratings yet
- Nursing Home Vaccine Order 1-19-22Document3 pagesNursing Home Vaccine Order 1-19-22WXYZ-TV Channel 7 DetroitNo ratings yet
- Gingival and Periodontal Indices: January 2021Document44 pagesGingival and Periodontal Indices: January 2021husnul khatimahNo ratings yet
- Case Report On Oral Leukoplakia With Superadded FuDocument3 pagesCase Report On Oral Leukoplakia With Superadded FuR Handi BramantoNo ratings yet
- Periodontal Chart Dan Periodontal Risk AssessmentDocument8 pagesPeriodontal Chart Dan Periodontal Risk AssessmentIndah VitasariNo ratings yet
- Sensors: /CAM Digital Impressions With Fferent Intraoral Scanner ParametersDocument9 pagesSensors: /CAM Digital Impressions With Fferent Intraoral Scanner ParametersbuccalNo ratings yet
- Osteonecrosis of The JawDocument47 pagesOsteonecrosis of The JawSamueal DurairajNo ratings yet
- Principles of Management of Impacted Teeth: LarryDocument30 pagesPrinciples of Management of Impacted Teeth: LarryRHMK11. BÙI BẢO TRUNGNo ratings yet
- JD Fs Papilla Preservation FlapDocument7 pagesJD Fs Papilla Preservation FlapReshmaa RajendranNo ratings yet
- P ProphylaxisDocument5 pagesP ProphylaxisLeticia Quiñonez VivasNo ratings yet
- Failure FPDDocument7 pagesFailure FPDArjun NarangNo ratings yet
- IndianJDentSci92126-1778286 045622Document8 pagesIndianJDentSci92126-1778286 045622Debora NatalynaNo ratings yet
- 2.heart Rate - An Emerging Risk Factor in CVDDocument49 pages2.heart Rate - An Emerging Risk Factor in CVDAkhil SharmaNo ratings yet
- CA Prostate by Dr. Musaib MushtaqDocument71 pagesCA Prostate by Dr. Musaib MushtaqDr. Musaib MushtaqNo ratings yet
- Gerodontology BaruDocument53 pagesGerodontology BaruHappy Septianto S100% (1)
- Pulp Protection CorrectedDocument22 pagesPulp Protection CorrectedSilky GroverNo ratings yet
- Diagnosis Dan Tatalaksana Dislokasi Lensa Intraokular Ke Posterior Dengan Prosedur IOL Exchange To Iris Claw Retropupillary - Siti AisyahDocument13 pagesDiagnosis Dan Tatalaksana Dislokasi Lensa Intraokular Ke Posterior Dengan Prosedur IOL Exchange To Iris Claw Retropupillary - Siti Aisyahmemmuse95No ratings yet
- AppenDocument54 pagesAppenmoqtadirNo ratings yet
- 4.radiolucent Inflammatory Jaw Lesions A TwentyyearDocument7 pages4.radiolucent Inflammatory Jaw Lesions A TwentyyearMihaela TuculinaNo ratings yet
- Topical Fluoride PrintDocument45 pagesTopical Fluoride PrintAmal ANo ratings yet
- Comparative Evaluation of Microleakage of Newer Generation of Dentin Bonding Agents in Class V Cavity: A Dye Penetration StudyDocument5 pagesComparative Evaluation of Microleakage of Newer Generation of Dentin Bonding Agents in Class V Cavity: A Dye Penetration StudyIJAR JOURNALNo ratings yet
- Burning Mouth SyndromeDocument7 pagesBurning Mouth SyndromeRobertoNo ratings yet
- Burning Mouth Syndrome: A Brief ReviewDocument6 pagesBurning Mouth Syndrome: A Brief ReviewIOSRjournalNo ratings yet
- Zborowski and Konopka - 2022 - Comparison of Clonazepam and Tongue Protector in TDocument15 pagesZborowski and Konopka - 2022 - Comparison of Clonazepam and Tongue Protector in TMémoire StomatodynieNo ratings yet
- Burning Mouth DisorderDocument4 pagesBurning Mouth DisorderMémoire StomatodynieNo ratings yet
- Arbabi-Kalati Et Al. - 2015 - Evaluation of The Efficacy of Low-Level Laser in IDocument4 pagesArbabi-Kalati Et Al. - 2015 - Evaluation of The Efficacy of Low-Level Laser in IMémoire StomatodynieNo ratings yet
- Burning Mouth SyndromeDocument11 pagesBurning Mouth SyndromeMémoire StomatodynieNo ratings yet
- Burning Tongue and Burning Tip The Diagnostic Challenge of The Burning Mouth SyndromeDocument5 pagesBurning Tongue and Burning Tip The Diagnostic Challenge of The Burning Mouth SyndromeMémoire StomatodynieNo ratings yet
- A Pragmatic Evidence-Based Clinical Management Algorithm For Burning Mouth SyndromeDocument6 pagesA Pragmatic Evidence-Based Clinical Management Algorithm For Burning Mouth SyndromeMémoire StomatodynieNo ratings yet
- A Case-Control Study On Etiological Factors Involved in Patients With Burning Mouth SyndromeDocument5 pagesA Case-Control Study On Etiological Factors Involved in Patients With Burning Mouth SyndromeMémoire StomatodynieNo ratings yet
- Acta Sci Dent Sci 2018. Burning Mouth Syndrome - Pathophysiology Investigations Management. A ReviewDocument7 pagesActa Sci Dent Sci 2018. Burning Mouth Syndrome - Pathophysiology Investigations Management. A ReviewMémoire StomatodynieNo ratings yet
- Candida 2Document12 pagesCandida 2Mémoire StomatodynieNo ratings yet
- Amanita MuscariaDocument16 pagesAmanita MuscariaPedro Rodrigues100% (1)
- Biliary Enteric BypassDocument25 pagesBiliary Enteric BypassAlexandru Ferdohleb100% (1)
- Adrenaline (Epinephrine) Nebulised 2016: AlertDocument2 pagesAdrenaline (Epinephrine) Nebulised 2016: AlertnurfitriaNo ratings yet
- Invertebrate Embryology and Reproduction 1St Edition Fatma Mahmoud El Bawab Full ChapterDocument67 pagesInvertebrate Embryology and Reproduction 1St Edition Fatma Mahmoud El Bawab Full Chapterida.drennon798100% (7)
- Hemostasis:: (Stoppage of Blood Flow After Damage)Document5 pagesHemostasis:: (Stoppage of Blood Flow After Damage)raanja2No ratings yet
- Full Download Test Bank For Color Textbook of Histology 3rd Edition Leslie P Gartner PDF Full ChapterDocument36 pagesFull Download Test Bank For Color Textbook of Histology 3rd Edition Leslie P Gartner PDF Full Chaptersouvenir.mutterer.j1rb100% (21)
- Functional Anatomy and Physiology of Airway PDFDocument21 pagesFunctional Anatomy and Physiology of Airway PDFCarolina Sousa DiasNo ratings yet
- Chapter 2. Lecture 4. Human SexualityDocument5 pagesChapter 2. Lecture 4. Human SexualitySmileCaturasNo ratings yet
- Gneral AnsDocument24 pagesGneral Ans39 femina pcNo ratings yet
- NUMS-MBBS Curriculum 1st Year 2020Document108 pagesNUMS-MBBS Curriculum 1st Year 2020nadia100% (1)
- Endocrine Chapter TestDocument4 pagesEndocrine Chapter TestPrince K. TaileyNo ratings yet
- Dragon Genetics WorksheetDocument4 pagesDragon Genetics WorksheetlicservernoidaNo ratings yet
- Introduction To Anatomy and PhysiologyDocument43 pagesIntroduction To Anatomy and Physiologyaarti HingeNo ratings yet
- Abdominal SurgeryDocument166 pagesAbdominal SurgeryIndera VyasNo ratings yet
- Daily Practice Test-04 (Zoology) QuestionsDocument5 pagesDaily Practice Test-04 (Zoology) QuestionsShweta GajbhiyeNo ratings yet
- Max Grow 8 WKDocument63 pagesMax Grow 8 WKFarheen Ashraf100% (1)
- Final OutputDocument16 pagesFinal OutputAnonymous USxVK0No ratings yet
- Subclinical Celiac Disease and Crystal-Induced Kidney Disease Following Kidney TransplantDocument6 pagesSubclinical Celiac Disease and Crystal-Induced Kidney Disease Following Kidney TransplantsigmundmaharajanNo ratings yet
- (Reviews in Mineralogy and Geochemistry'', 54) Patricia M. Dove, James J. de Yoreo, Steve Weiner-Biomineralization-Mineralogical Society of America (2003)Document377 pages(Reviews in Mineralogy and Geochemistry'', 54) Patricia M. Dove, James J. de Yoreo, Steve Weiner-Biomineralization-Mineralogical Society of America (2003)Karlii BasilioNo ratings yet
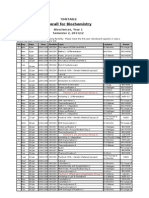
- Semester 2 Biochem TimetableDocument1 pageSemester 2 Biochem TimetablesophiecabNo ratings yet
- Amino Acids and Proteins ReviewerDocument11 pagesAmino Acids and Proteins ReviewerJohn-Karl JimenezNo ratings yet
- Drilling QuestionDocument56 pagesDrilling QuestionMohamad HattaNo ratings yet
- Sci10 Quarter 3 Module 1 NO ANSWER KEYDocument30 pagesSci10 Quarter 3 Module 1 NO ANSWER KEYNiña Miles TabañagNo ratings yet
- Awakened Masculine EbookDocument14 pagesAwakened Masculine EbookBenito OteroNo ratings yet
- AdEasy Adenoviral Vector SystemDocument43 pagesAdEasy Adenoviral Vector SystemDaniel PintoNo ratings yet
- Auto PEEPDocument16 pagesAuto PEEPVishwajith Murthy100% (1)
- Sternocleidomastoid Muscle: OriginDocument1 pageSternocleidomastoid Muscle: OriginBogdan Robert CNo ratings yet
- HUBS1105 Bones and Joints of The Skull and FaceDocument5 pagesHUBS1105 Bones and Joints of The Skull and FaceChloe HeuchanNo ratings yet