Download as pdf or txt
You might also like
- Module I - Introduction To Occupational Health and SafetyDocument13 pagesModule I - Introduction To Occupational Health and Safetyangeh morilloNo ratings yet
- Hazard Communication: OSHA Office of Training and EducationDocument17 pagesHazard Communication: OSHA Office of Training and EducationArdian20No ratings yet
- Guess The Word ActivityDocument28 pagesGuess The Word ActivityChris GarciaNo ratings yet
- Confined SpacesDocument25 pagesConfined SpaceshemanthNo ratings yet
- The American University in Cairo Environmental Health & Safety DepartmentDocument91 pagesThe American University in Cairo Environmental Health & Safety DepartmentBabbooNo ratings yet
- Confine Space Entry (Excavation)Document32 pagesConfine Space Entry (Excavation)Delta akathehuskyNo ratings yet
- Working at HeightDocument6 pagesWorking at HeightAykut KarakavakNo ratings yet
- Arkansas Kraft Division Contractor Safety OrientationDocument63 pagesArkansas Kraft Division Contractor Safety Orientationdavid_stephens_29No ratings yet
- Common Construction Safety Officer Interview QuestionsDocument12 pagesCommon Construction Safety Officer Interview Questionskenedy nuwaherezaNo ratings yet
- 25 - Welding, Cutting and Hot WorkDocument16 pages25 - Welding, Cutting and Hot WorkRicardo DalisayNo ratings yet
- Hazard Identification (Hazid) NO YES: Checklist Analysis Hazop + Checklist AnalysisDocument7 pagesHazard Identification (Hazid) NO YES: Checklist Analysis Hazop + Checklist AnalysisZeroRecoNo ratings yet
- Chapter 1-Introduction To OshaDocument32 pagesChapter 1-Introduction To OshafettaneNo ratings yet
- Safety Data Sheet: Delo Gold Ultra SAE 15W-40Document6 pagesSafety Data Sheet: Delo Gold Ultra SAE 15W-40Nasta Ina RobayasaNo ratings yet
- Personal Protective EquipmentDocument9 pagesPersonal Protective EquipmentMuhammad Abdul RaufNo ratings yet
- Fire - Risk AssessmentDocument14 pagesFire - Risk AssessmentRameeSahiba100% (1)
- IGC1 Element 4 End of Element Questions and Answers Health and Safety Management Systems 3 - PlanningDocument5 pagesIGC1 Element 4 End of Element Questions and Answers Health and Safety Management Systems 3 - PlanningDrmusharraf AnsariNo ratings yet
- 3 Lecture 2 N 3-1 Fundamentals of SafetyDocument29 pages3 Lecture 2 N 3-1 Fundamentals of SafetyArjan GhoshNo ratings yet
- Basics of FireDocument2 pagesBasics of FireMr. X100% (1)
- Safety in Confined SpaceDocument36 pagesSafety in Confined Spacekim nichole mendozaNo ratings yet
- Bosh1103 - 7.0 Chemical Health Risk AssessmentDocument59 pagesBosh1103 - 7.0 Chemical Health Risk AssessmentAddry AlffianNo ratings yet
- Fire Risk Assessment and Emergency Route Decision Analysis Based On Big Data Platform-Example of HuizhouDocument12 pagesFire Risk Assessment and Emergency Route Decision Analysis Based On Big Data Platform-Example of HuizhouPriyanka KilaniyaNo ratings yet
- Ergonomics: 1. PurposeDocument9 pagesErgonomics: 1. Purposevipin2209No ratings yet
- OHS Baseline Risk Assessment - Catering Contract October 2021Document18 pagesOHS Baseline Risk Assessment - Catering Contract October 2021denoiNo ratings yet
- Safety Program (d1)Document21 pagesSafety Program (d1)elvis hidalgoNo ratings yet
- PTW ProcedureDocument3 pagesPTW ProcedureangelaNo ratings yet
- Cabinet Decree (12) of 2006Document63 pagesCabinet Decree (12) of 2006Sumitra BanuNo ratings yet
- EHS AgreementDocument37 pagesEHS AgreementSantosh KumarNo ratings yet
- Intel Construction EHS: Processes and Procedures ManualDocument116 pagesIntel Construction EHS: Processes and Procedures ManualbasshotNo ratings yet
- Nebosh 1gc1Document10 pagesNebosh 1gc1Hari PrasadNo ratings yet
- Project Health Safety and Environmental HSE Plan With All Forms - Method Statement HQDocument3 pagesProject Health Safety and Environmental HSE Plan With All Forms - Method Statement HQsvsrnbNo ratings yet
- PTW - Permit To Work ProcedureDocument3 pagesPTW - Permit To Work ProcedureFOZCANNo ratings yet
- CSHP Checklist 2011Document2 pagesCSHP Checklist 2011JenniferValle0% (1)
- Construction Safety SpecificationDocument12 pagesConstruction Safety Specificationmelantnor_19No ratings yet
- Standard For Old Age PDFDocument65 pagesStandard For Old Age PDFRendani VeleNo ratings yet
- FPS 008 - WeldingREV1Document3 pagesFPS 008 - WeldingREV1grantNo ratings yet
- Riddor: Health and Safety Advice For StonemasonsDocument12 pagesRiddor: Health and Safety Advice For StonemasonsMohammed Illiasuddin100% (1)
- Chemical Hygiene Plan PDFDocument186 pagesChemical Hygiene Plan PDFAnonymous Oqmiu1No ratings yet
- Emergency PlanDocument1 pageEmergency Planapi-285003764No ratings yet
- Safe Work Method For Peb Work: Procedure Possible Hazards Control MeasuresDocument35 pagesSafe Work Method For Peb Work: Procedure Possible Hazards Control Measuressandip patilNo ratings yet
- Project: Field Erection of 15000 Bbls Tank (Ik-2545) : Job Safety Analysis / Safe Work Method Statement-SWMSDocument2 pagesProject: Field Erection of 15000 Bbls Tank (Ik-2545) : Job Safety Analysis / Safe Work Method Statement-SWMSJohn100% (2)
- GC Risk Assessment 1Document2 pagesGC Risk Assessment 1api-464221711No ratings yet
- Hirarc: Made Up From 3 Activities That Consist of Hazard Identification, Risk Assesment and Risk ControlDocument12 pagesHirarc: Made Up From 3 Activities That Consist of Hazard Identification, Risk Assesment and Risk ControlHamizi AzizanNo ratings yet
- Personal Protective Equipment (PPE) at Work: A Brief GuideDocument6 pagesPersonal Protective Equipment (PPE) at Work: A Brief GuideMohamed Omar100% (1)
- Health Safety and Welfare For Construction ManagementDocument23 pagesHealth Safety and Welfare For Construction ManagementOchini Chandrasena100% (2)
- Safety & Health ProgramDocument2 pagesSafety & Health ProgramD.k. PathakNo ratings yet
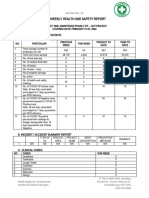
- Hse Weekly Report SampleDocument5 pagesHse Weekly Report SampleGerson Monsanto Jr.No ratings yet
- Module 1 - C - INTRO TO HIRACDocument15 pagesModule 1 - C - INTRO TO HIRACian nel meloNo ratings yet
- Duke University - Facilities Management Department: Ergonomics ProgramDocument4 pagesDuke University - Facilities Management Department: Ergonomics ProgramEdgard Bruno Soto LuqueNo ratings yet
- Module 7 Heirarchy of ControlsDocument56 pagesModule 7 Heirarchy of ControlsDaneNo ratings yet
- Basic Safety PDFDocument69 pagesBasic Safety PDFMichael M. SolivaNo ratings yet
- Reviewer of NeboshDocument22 pagesReviewer of NeboshJie DVNo ratings yet
- 4.2 Unit GC2: Controlling Workplace Hazards: Learning OutcomesDocument18 pages4.2 Unit GC2: Controlling Workplace Hazards: Learning Outcomesnavin100% (2)
- Confined Space - Introduction: Canadian Government Departments Responsible For OH&S Confined Space - ProgramDocument7 pagesConfined Space - Introduction: Canadian Government Departments Responsible For OH&S Confined Space - ProgramAnge JuanNo ratings yet
- Key Elements of Health and Safety Management SystemDocument6 pagesKey Elements of Health and Safety Management SystemGabbar 98No ratings yet
- Tool Box TalkDocument1 pageTool Box TalkBhanu PrakashNo ratings yet
- Chapter 5 - Occupational Health & HygieneDocument19 pagesChapter 5 - Occupational Health & Hygieneheykoolkid0100% (1)
- Hazard Communication and GHS: Al Babtain Hse DepartmentDocument65 pagesHazard Communication and GHS: Al Babtain Hse DepartmentKhalid Mohammed SaudNo ratings yet
- Certified Health And Safety Consultant A Complete Guide - 2020 EditionFrom EverandCertified Health And Safety Consultant A Complete Guide - 2020 EditionNo ratings yet
- Emergency Evacuation Planning for Your Workplace: From Chaos to Life-Saving SolutionsFrom EverandEmergency Evacuation Planning for Your Workplace: From Chaos to Life-Saving SolutionsNo ratings yet
- 15a. First Aid ManualDocument73 pages15a. First Aid ManualchimaraiykeNo ratings yet
- Management SystemsDocument35 pagesManagement SystemschimaraiykeNo ratings yet
- Managing HSE in ContractsDocument16 pagesManaging HSE in ContractschimaraiykeNo ratings yet
- HSE StatisticsDocument13 pagesHSE StatisticschimaraiykeNo ratings yet
- Job Hazard Analysis Awareness TrainingDocument56 pagesJob Hazard Analysis Awareness TrainingchimaraiykeNo ratings yet
- 103 Titan Diesel Plus 15W40Document5 pages103 Titan Diesel Plus 15W40M.TayyabNo ratings yet
- Msds of Methyl ChloroformDocument9 pagesMsds of Methyl Chloroformkerem__22No ratings yet
- Ghs Safety Data Sheet: Section 1 IdentificationDocument5 pagesGhs Safety Data Sheet: Section 1 IdentificationRufinoArturoFranquezPradoNo ratings yet
- Witcher Alchemy - For WebDocument32 pagesWitcher Alchemy - For WebAlkarsilverbladeNo ratings yet
- Safety Assessment of Methanol Extract of Red Dragon Fruit (Hylocereus Polyrhizus) - Acute and Subchronic Toxicity Studies PDFDocument9 pagesSafety Assessment of Methanol Extract of Red Dragon Fruit (Hylocereus Polyrhizus) - Acute and Subchronic Toxicity Studies PDFBiyaya San PedroNo ratings yet
- Guidance For Industry Safety Testing of Drug Metabolites - FDA 2008Document14 pagesGuidance For Industry Safety Testing of Drug Metabolites - FDA 2008Enrica GaNo ratings yet
- SDS-Sodium Metabisulfite Food Grade (E223)Document14 pagesSDS-Sodium Metabisulfite Food Grade (E223)lokeshNo ratings yet
- ThinnerDocument13 pagesThinnerhgfsdeNo ratings yet
- Rustop 274: Material Safety Data SheetDocument4 pagesRustop 274: Material Safety Data SheetYudhveer GrewalNo ratings yet
- Glyeo SDSDocument12 pagesGlyeo SDSquzalbashNo ratings yet
- Hazard Identification and Risk AssessmentDocument4 pagesHazard Identification and Risk AssessmentSyed Haider Abbas KazmiNo ratings yet
- Solcart B SafetydatasheetDocument6 pagesSolcart B SafetydatasheetAditya NugrahaNo ratings yet
- 2.2 INOGATE - Software For Consequence ModellingDocument25 pages2.2 INOGATE - Software For Consequence ModellingVesko IlijaziNo ratings yet
- MSDS Flocon 260 NDocument4 pagesMSDS Flocon 260 NSeguridad TransgroupNo ratings yet
- Isopropyl Alcohol (Ipa) Safety DatasheetDocument4 pagesIsopropyl Alcohol (Ipa) Safety Datasheetaqmar aqeemNo ratings yet
- R20 - Potassium Chromate IndicatorDocument4 pagesR20 - Potassium Chromate IndicatorLaboratorium PT MASNo ratings yet
- Safety Data Sheet: Section 1. IdentificationDocument9 pagesSafety Data Sheet: Section 1. Identificationhunais ali aliNo ratings yet
- Msds Tamol NN 9104Document6 pagesMsds Tamol NN 9104顾云飞No ratings yet
- Máy Nén Khí NXL 3000 PDFDocument16 pagesMáy Nén Khí NXL 3000 PDFQuyên NguyễnNo ratings yet
- Provichem 2202 - MSDSDocument8 pagesProvichem 2202 - MSDSMohamed HalemNo ratings yet
- GE15 - SIM Week 6-7Document4 pagesGE15 - SIM Week 6-7Althea Nicole QuindoNo ratings yet
- Process Design Package: P170 ManualDocument52 pagesProcess Design Package: P170 ManualRashidul Islam MasumNo ratings yet
- Favipiravir Tablet Manual: Please Read The Instructions Carefully and Use Under The Guidance of A PhysicianDocument4 pagesFavipiravir Tablet Manual: Please Read The Instructions Carefully and Use Under The Guidance of A Physicianchard xuNo ratings yet
- Risk Assessment & Process Hazard AnalysisDocument22 pagesRisk Assessment & Process Hazard AnalysisChaudhary KashifNo ratings yet
- Chapter 16. Toxicity Test Against InsectsDocument6 pagesChapter 16. Toxicity Test Against Insects5pn4x4czxnNo ratings yet
- Asam Asetat 3% - MSDS MyDocument6 pagesAsam Asetat 3% - MSDS MyAnnisa Nur JNo ratings yet
- 2-Naphthol Safety SheetDocument8 pages2-Naphthol Safety SheetalonrabNo ratings yet
- Hazardous Waste Definition and ClassificationDocument20 pagesHazardous Waste Definition and ClassificationRobertus Wisnu WijayaNo ratings yet
- SdsDocument13 pagesSdsAgunk IstriNo ratings yet
- Part 2Document127 pagesPart 2Sri PurwaningsihNo ratings yet