
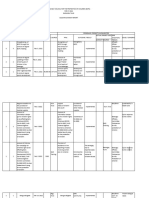
CICL Intake and Referral
CICL Intake and Referral
You might also like
- Income Tax Computation FormatDocument2 pagesIncome Tax Computation Formatrathan50% (4)
- MC 1 Series of 2022 Joint Memo of DILG - DSWD To Support The Program Implementation of Pantawid Pamilya ImplementationDocument8 pagesMC 1 Series of 2022 Joint Memo of DILG - DSWD To Support The Program Implementation of Pantawid Pamilya ImplementationJeshella Roxas100% (1)
- JJWC PDF Flowchart - Ordinance Violation CAR (REV)Document1 pageJJWC PDF Flowchart - Ordinance Violation CAR (REV)ali namla100% (1)
- Lecture On The Barangay Council For The Protection of ChildrenDocument4 pagesLecture On The Barangay Council For The Protection of ChildrenYei S. Joaquin100% (3)
- Lcat Vawc FormDocument1 pageLcat Vawc FormKurt Javier0% (1)
- Intake Sheet For Children in Conflict With The Law (Cicl) and Child at Risk (Car)Document2 pagesIntake Sheet For Children in Conflict With The Law (Cicl) and Child at Risk (Car)Ann Jelaine Noveno100% (4)
- Draft Design - Erpat TraainingDocument2 pagesDraft Design - Erpat TraainingMerry Merry100% (1)
- Certificate of Actual TillerDocument1 pageCertificate of Actual TillerMaria Ailene SantoNo ratings yet
- Narrative Report Re Children's CongressDocument1 pageNarrative Report Re Children's CongressJojirose Anne Bernardo Monding100% (1)
- CFLGA Field Testing - Handbook PDFDocument63 pagesCFLGA Field Testing - Handbook PDFAbe Anshari100% (1)
- BIDADocument1 pageBIDAkim penalbaNo ratings yet
- SGLGB Executive Order GAD GFPs GAD Article 1Document4 pagesSGLGB Executive Order GAD GFPs GAD Article 1Donavel Nodora JojuicoNo ratings yet
- 2022-Bcpc-Minutes-Format Quarterly and SpecialDocument13 pages2022-Bcpc-Minutes-Format Quarterly and SpecialEm Tee AiareeneNo ratings yet
- Accomplishment Report BCPC 2022Document7 pagesAccomplishment Report BCPC 2022Mela BalagotNo ratings yet
- LCPC Indicators Guide With MOVsDocument35 pagesLCPC Indicators Guide With MOVsRhapNo ratings yet
- Activity Report & Photo HCL and Auxiliary Team TrainingDocument3 pagesActivity Report & Photo HCL and Auxiliary Team Trainingbarangay artacho1964 bautistaNo ratings yet
- Sample Eo BhraoDocument1 pageSample Eo BhraoFreduu Langs100% (2)
- BCPC Intake FormDocument2 pagesBCPC Intake FormAileen Labastida Barcenas100% (2)
- Chr-Dilg JMC 2020-01 M&e Tool 1Document5 pagesChr-Dilg JMC 2020-01 M&e Tool 1Relyanz Nisnisan OmandamNo ratings yet
- Barangay ProfileDocument13 pagesBarangay ProfileFredd Sherwin PanimNo ratings yet
- Persons With Disability Affairs Office Annual Accomplishment ReportDocument2 pagesPersons With Disability Affairs Office Annual Accomplishment ReportJoemar CafrancaNo ratings yet
- Barangay Data Capture Form Monitoring of Incidence On Violence Against Children (Vac) During The Covid-19 PandemicDocument1 pageBarangay Data Capture Form Monitoring of Incidence On Violence Against Children (Vac) During The Covid-19 PandemicChristopher Gatdula100% (2)
- Certificate of Common LawDocument7 pagesCertificate of Common LawBarangay AmasNo ratings yet
- VAWC Quarterly ReportDocument1 pageVAWC Quarterly ReportMswdo Talavera0% (1)
- Certification BCPC Child RepresentativeDocument2 pagesCertification BCPC Child RepresentativeAnna Lisa DaguinodNo ratings yet
- Barangay Peace and Order Council (BPOC) Barangay Council For The Protection of Children (BCPC) Violence Against Women (VAW) DeskDocument5 pagesBarangay Peace and Order Council (BPOC) Barangay Council For The Protection of Children (BCPC) Violence Against Women (VAW) DeskDenver DiocaresNo ratings yet
- Republic of The Philippines Province of Masbate City of MasbateDocument2 pagesRepublic of The Philippines Province of Masbate City of MasbateBRGY. BAGUMBAYAN100% (2)
- BCPC Eo-4 2018Document2 pagesBCPC Eo-4 2018JOEL VELASCONo ratings yet
- Form BHERTsDocument1 pageForm BHERTsCasey Del Gallego EnrileNo ratings yet
- Coc Sangguniang BarangayDocument2 pagesCoc Sangguniang BarangayAGrace MercadoNo ratings yet
- Sample Cbjip Book of Barangay Kauswagan 1Document38 pagesSample Cbjip Book of Barangay Kauswagan 1Johana Pinagayao AngkadNo ratings yet
- 2022 Children's ReportDocument3 pages2022 Children's ReportMSWD Camiling100% (2)
- CBJIP Matrix PulilanDocument2 pagesCBJIP Matrix PulilanErickson PinedaNo ratings yet
- Office of The Punong Barangay Executive Order No. 005 Series of 2019Document2 pagesOffice of The Punong Barangay Executive Order No. 005 Series of 2019Meraki PHNo ratings yet
- Ncip Genealogy FormDocument1 pageNcip Genealogy FormIsidro LusantaNo ratings yet
- State of The Childrens Report by DILG 2021Document5 pagesState of The Childrens Report by DILG 2021dr.ariel1979No ratings yet
- Barangay Profile: (BP DCF No. 1 S. 2020)Document4 pagesBarangay Profile: (BP DCF No. 1 S. 2020)Richard Bandong100% (1)
- BOIS Form - Elective Officials Revised 2013Document1 pageBOIS Form - Elective Officials Revised 2013Marilou Maturan100% (1)
- ISABELA Monitoring Template For The HAPAG Project LaunchingDocument5 pagesISABELA Monitoring Template For The HAPAG Project Launchingedrie matiasNo ratings yet
- Sustainability Assessment of The Kalipunan NG Liping Pilipina (KALIPI) Program Implementation in Iligan City and Cagayan de Oro CityDocument12 pagesSustainability Assessment of The Kalipunan NG Liping Pilipina (KALIPI) Program Implementation in Iligan City and Cagayan de Oro CityPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Barangay Anti Drug Abuse CouncilDocument5 pagesBarangay Anti Drug Abuse CouncilANDRELYN PEPENo ratings yet
- LSCR ReportDocument10 pagesLSCR ReportCpu Silang100% (1)
- Eo BNCDocument2 pagesEo BNCMaris Rosabal Nalual100% (1)
- Aksyon Barangay Kontra Dengue (Abkd)Document1 pageAksyon Barangay Kontra Dengue (Abkd)jane franciscoNo ratings yet
- Executive Order Establishing The Barangay Violence Against Women (Vaw) Desk and Designating The Barangay Vaw Desk OfficerDocument2 pagesExecutive Order Establishing The Barangay Violence Against Women (Vaw) Desk and Designating The Barangay Vaw Desk OfficerRobert Tayam, Jr.100% (1)
- 2-A Guide To Answering Badac Self-Assessment and Audit FormDocument3 pages2-A Guide To Answering Badac Self-Assessment and Audit FormSHEENA83% (12)
- Diversion Program of ArtachoDocument2 pagesDiversion Program of ArtachojomarNo ratings yet
- Post Activity ReportDocument3 pagesPost Activity ReportBarangay PalabotanNo ratings yet
- Barangay Literacy EODocument3 pagesBarangay Literacy EOMalvin Dean100% (1)
- VAWC Accomplishment ReportDocument1 pageVAWC Accomplishment ReportBarangay PalabotanNo ratings yet
- Safety Seal Certification ChecklistDocument2 pagesSafety Seal Certification ChecklistHav Cats100% (2)
- Eo VawcDocument1 pageEo VawcJolina Magpali TangalinNo ratings yet
- 2ND Quarter of Clean Up DriveDocument3 pages2ND Quarter of Clean Up DriveBarangay SamputNo ratings yet
- Barangay Resolution BHRACDocument4 pagesBarangay Resolution BHRACChaf Nicole Castro100% (2)
- Office of The Barangay Council Activity DesignedDocument3 pagesOffice of The Barangay Council Activity DesignedCharmain JRazNo ratings yet
- REPORT - Katarungang-PambarangayDocument1 pageREPORT - Katarungang-PambarangayMarc Mendoza100% (1)
- Citizens CharterDocument27 pagesCitizens CharterRolando Tatong100% (1)
- Worksheet 1 Situation of Children in Conflict With The Law and Children at RiskDocument8 pagesWorksheet 1 Situation of Children in Conflict With The Law and Children at RiskGuyam MalakiNo ratings yet
- Unified LCPC MC (Template Form)Document13 pagesUnified LCPC MC (Template Form)Ian Jun GestaNo ratings yet
- Job Application Form - ExecutiveDocument2 pagesJob Application Form - ExecutiveWan Qing NgNo ratings yet
- BIS Personal Applicant FormDocument3 pagesBIS Personal Applicant FormDanny stampNo ratings yet
- Checklist Grant For Wholesale Drug License PDFDocument11 pagesChecklist Grant For Wholesale Drug License PDFShwetank SinghNo ratings yet
- GP Fund Form BDocument2 pagesGP Fund Form BIrfan ArifNo ratings yet
- Invitation - 1Document8 pagesInvitation - 1amaNo ratings yet
- Soroban Exercises P8cRBjsDocument1 pageSoroban Exercises P8cRBjsSilvia OitaNo ratings yet
- Indigo Plantation and EffectsDocument8 pagesIndigo Plantation and Effectstaran vlogsNo ratings yet
- Imperialism: Imperialism Is A Policy or Ideology of Extending The Rule OverDocument32 pagesImperialism: Imperialism Is A Policy or Ideology of Extending The Rule OverSydknee Lie-onNo ratings yet
- STD VIII NOTES CIVICS CH.5 - JudiciaryDocument3 pagesSTD VIII NOTES CIVICS CH.5 - JudiciaryAnshul DessaiNo ratings yet
- Confession Death Guilt Regrets SinsDocument1 pageConfession Death Guilt Regrets SinsLNo ratings yet
- Purnell L. The Purnell Model For Cultural Competence. Journal of Transcultural NursingDocument10 pagesPurnell L. The Purnell Model For Cultural Competence. Journal of Transcultural NursingCengizhan ErNo ratings yet
- InvoiceDocument1 pageInvoicebshari93_918887308No ratings yet
- Combatting Business To Business Fraud Benchmarking Report TR ACFE 2023Document28 pagesCombatting Business To Business Fraud Benchmarking Report TR ACFE 2023Karina ChuzevilleNo ratings yet
- 1 The Contemporary World ReviewDocument44 pages1 The Contemporary World ReviewKim Mariah AndalesNo ratings yet
- Haryana Staff Selection Commission: Reservation DetailsDocument2 pagesHaryana Staff Selection Commission: Reservation DetailsRimmy BhardwajNo ratings yet
- Buytosell Subscription Form FaqDocument3 pagesBuytosell Subscription Form FaqNWELENo ratings yet
- Deed of Absolute SaleDocument2 pagesDeed of Absolute SaleDenee Vem MatorresNo ratings yet
- USE UNLESS (Remove If) Notes by Vijay Salunke SirDocument2 pagesUSE UNLESS (Remove If) Notes by Vijay Salunke Sirdevrarimanish72No ratings yet
- Hong Kong - Salary Survey - 2021Document6 pagesHong Kong - Salary Survey - 2021Nathan SmithNo ratings yet
- Consti2 - Cases AgainDocument13 pagesConsti2 - Cases AgainChaNo ratings yet
- 03 Handout 1Document4 pages03 Handout 1Katelyn Mae SungcangNo ratings yet
- Price List All Models - ASHDocument1 pagePrice List All Models - ASHSia Siaw LangNo ratings yet
- EO 6 S 2021 - Data-Privacy-Officer-DPO-BarangayDocument2 pagesEO 6 S 2021 - Data-Privacy-Officer-DPO-BarangayBARANGAY MOLINO II100% (2)
- PDF Document 6Document8 pagesPDF Document 6Happi TummyNo ratings yet
- Buen VivirDocument36 pagesBuen VivirJúlia GusmãoNo ratings yet
- Decree 25 2013 v31 of The Ministry of National Development On The Amount of The Toll and Toll Roads Effective As of 15092015Document107 pagesDecree 25 2013 v31 of The Ministry of National Development On The Amount of The Toll and Toll Roads Effective As of 15092015MelecaNo ratings yet
- People VS PalijonDocument3 pagesPeople VS PalijonRyannDeLeonNo ratings yet
- 160526AttyFeeMotionPkgRcvdStamped PDFDocument61 pages160526AttyFeeMotionPkgRcvdStamped PDFStephanie RueNo ratings yet
- Cheng vs. SyDocument9 pagesCheng vs. SyRivera Meriem Grace MendezNo ratings yet
- Living Outside BarsDocument10 pagesLiving Outside BarsLea UnderscoreNo ratings yet
- Candidate For Nomination Profile Template - (2016.01.20)Document1 pageCandidate For Nomination Profile Template - (2016.01.20)nasirNo ratings yet
























































































Download as pdf or txt
You might also like
- Income Tax Computation FormatDocument2 pagesIncome Tax Computation Formatrathan50% (4)
- MC 1 Series of 2022 Joint Memo of DILG - DSWD To Support The Program Implementation of Pantawid Pamilya ImplementationDocument8 pagesMC 1 Series of 2022 Joint Memo of DILG - DSWD To Support The Program Implementation of Pantawid Pamilya ImplementationJeshella Roxas100% (1)
- JJWC PDF Flowchart - Ordinance Violation CAR (REV)Document1 pageJJWC PDF Flowchart - Ordinance Violation CAR (REV)ali namla100% (1)
- Lecture On The Barangay Council For The Protection of ChildrenDocument4 pagesLecture On The Barangay Council For The Protection of ChildrenYei S. Joaquin100% (3)
- Lcat Vawc FormDocument1 pageLcat Vawc FormKurt Javier0% (1)
- Intake Sheet For Children in Conflict With The Law (Cicl) and Child at Risk (Car)Document2 pagesIntake Sheet For Children in Conflict With The Law (Cicl) and Child at Risk (Car)Ann Jelaine Noveno100% (4)
- Draft Design - Erpat TraainingDocument2 pagesDraft Design - Erpat TraainingMerry Merry100% (1)
- Certificate of Actual TillerDocument1 pageCertificate of Actual TillerMaria Ailene SantoNo ratings yet
- Narrative Report Re Children's CongressDocument1 pageNarrative Report Re Children's CongressJojirose Anne Bernardo Monding100% (1)
- CFLGA Field Testing - Handbook PDFDocument63 pagesCFLGA Field Testing - Handbook PDFAbe Anshari100% (1)
- BIDADocument1 pageBIDAkim penalbaNo ratings yet
- SGLGB Executive Order GAD GFPs GAD Article 1Document4 pagesSGLGB Executive Order GAD GFPs GAD Article 1Donavel Nodora JojuicoNo ratings yet
- 2022-Bcpc-Minutes-Format Quarterly and SpecialDocument13 pages2022-Bcpc-Minutes-Format Quarterly and SpecialEm Tee AiareeneNo ratings yet
- Accomplishment Report BCPC 2022Document7 pagesAccomplishment Report BCPC 2022Mela BalagotNo ratings yet
- LCPC Indicators Guide With MOVsDocument35 pagesLCPC Indicators Guide With MOVsRhapNo ratings yet
- Activity Report & Photo HCL and Auxiliary Team TrainingDocument3 pagesActivity Report & Photo HCL and Auxiliary Team Trainingbarangay artacho1964 bautistaNo ratings yet
- Sample Eo BhraoDocument1 pageSample Eo BhraoFreduu Langs100% (2)
- BCPC Intake FormDocument2 pagesBCPC Intake FormAileen Labastida Barcenas100% (2)
- Chr-Dilg JMC 2020-01 M&e Tool 1Document5 pagesChr-Dilg JMC 2020-01 M&e Tool 1Relyanz Nisnisan OmandamNo ratings yet
- Barangay ProfileDocument13 pagesBarangay ProfileFredd Sherwin PanimNo ratings yet
- Persons With Disability Affairs Office Annual Accomplishment ReportDocument2 pagesPersons With Disability Affairs Office Annual Accomplishment ReportJoemar CafrancaNo ratings yet
- Barangay Data Capture Form Monitoring of Incidence On Violence Against Children (Vac) During The Covid-19 PandemicDocument1 pageBarangay Data Capture Form Monitoring of Incidence On Violence Against Children (Vac) During The Covid-19 PandemicChristopher Gatdula100% (2)
- Certificate of Common LawDocument7 pagesCertificate of Common LawBarangay AmasNo ratings yet
- VAWC Quarterly ReportDocument1 pageVAWC Quarterly ReportMswdo Talavera0% (1)
- Certification BCPC Child RepresentativeDocument2 pagesCertification BCPC Child RepresentativeAnna Lisa DaguinodNo ratings yet
- Barangay Peace and Order Council (BPOC) Barangay Council For The Protection of Children (BCPC) Violence Against Women (VAW) DeskDocument5 pagesBarangay Peace and Order Council (BPOC) Barangay Council For The Protection of Children (BCPC) Violence Against Women (VAW) DeskDenver DiocaresNo ratings yet
- Republic of The Philippines Province of Masbate City of MasbateDocument2 pagesRepublic of The Philippines Province of Masbate City of MasbateBRGY. BAGUMBAYAN100% (2)
- BCPC Eo-4 2018Document2 pagesBCPC Eo-4 2018JOEL VELASCONo ratings yet
- Form BHERTsDocument1 pageForm BHERTsCasey Del Gallego EnrileNo ratings yet
- Coc Sangguniang BarangayDocument2 pagesCoc Sangguniang BarangayAGrace MercadoNo ratings yet
- Sample Cbjip Book of Barangay Kauswagan 1Document38 pagesSample Cbjip Book of Barangay Kauswagan 1Johana Pinagayao AngkadNo ratings yet
- 2022 Children's ReportDocument3 pages2022 Children's ReportMSWD Camiling100% (2)
- CBJIP Matrix PulilanDocument2 pagesCBJIP Matrix PulilanErickson PinedaNo ratings yet
- Office of The Punong Barangay Executive Order No. 005 Series of 2019Document2 pagesOffice of The Punong Barangay Executive Order No. 005 Series of 2019Meraki PHNo ratings yet
- Ncip Genealogy FormDocument1 pageNcip Genealogy FormIsidro LusantaNo ratings yet
- State of The Childrens Report by DILG 2021Document5 pagesState of The Childrens Report by DILG 2021dr.ariel1979No ratings yet
- Barangay Profile: (BP DCF No. 1 S. 2020)Document4 pagesBarangay Profile: (BP DCF No. 1 S. 2020)Richard Bandong100% (1)
- BOIS Form - Elective Officials Revised 2013Document1 pageBOIS Form - Elective Officials Revised 2013Marilou Maturan100% (1)
- ISABELA Monitoring Template For The HAPAG Project LaunchingDocument5 pagesISABELA Monitoring Template For The HAPAG Project Launchingedrie matiasNo ratings yet
- Sustainability Assessment of The Kalipunan NG Liping Pilipina (KALIPI) Program Implementation in Iligan City and Cagayan de Oro CityDocument12 pagesSustainability Assessment of The Kalipunan NG Liping Pilipina (KALIPI) Program Implementation in Iligan City and Cagayan de Oro CityPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Barangay Anti Drug Abuse CouncilDocument5 pagesBarangay Anti Drug Abuse CouncilANDRELYN PEPENo ratings yet
- LSCR ReportDocument10 pagesLSCR ReportCpu Silang100% (1)
- Eo BNCDocument2 pagesEo BNCMaris Rosabal Nalual100% (1)
- Aksyon Barangay Kontra Dengue (Abkd)Document1 pageAksyon Barangay Kontra Dengue (Abkd)jane franciscoNo ratings yet
- Executive Order Establishing The Barangay Violence Against Women (Vaw) Desk and Designating The Barangay Vaw Desk OfficerDocument2 pagesExecutive Order Establishing The Barangay Violence Against Women (Vaw) Desk and Designating The Barangay Vaw Desk OfficerRobert Tayam, Jr.100% (1)
- 2-A Guide To Answering Badac Self-Assessment and Audit FormDocument3 pages2-A Guide To Answering Badac Self-Assessment and Audit FormSHEENA83% (12)
- Diversion Program of ArtachoDocument2 pagesDiversion Program of ArtachojomarNo ratings yet
- Post Activity ReportDocument3 pagesPost Activity ReportBarangay PalabotanNo ratings yet
- Barangay Literacy EODocument3 pagesBarangay Literacy EOMalvin Dean100% (1)
- VAWC Accomplishment ReportDocument1 pageVAWC Accomplishment ReportBarangay PalabotanNo ratings yet
- Safety Seal Certification ChecklistDocument2 pagesSafety Seal Certification ChecklistHav Cats100% (2)
- Eo VawcDocument1 pageEo VawcJolina Magpali TangalinNo ratings yet
- 2ND Quarter of Clean Up DriveDocument3 pages2ND Quarter of Clean Up DriveBarangay SamputNo ratings yet
- Barangay Resolution BHRACDocument4 pagesBarangay Resolution BHRACChaf Nicole Castro100% (2)
- Office of The Barangay Council Activity DesignedDocument3 pagesOffice of The Barangay Council Activity DesignedCharmain JRazNo ratings yet
- REPORT - Katarungang-PambarangayDocument1 pageREPORT - Katarungang-PambarangayMarc Mendoza100% (1)
- Citizens CharterDocument27 pagesCitizens CharterRolando Tatong100% (1)
- Worksheet 1 Situation of Children in Conflict With The Law and Children at RiskDocument8 pagesWorksheet 1 Situation of Children in Conflict With The Law and Children at RiskGuyam MalakiNo ratings yet
- Unified LCPC MC (Template Form)Document13 pagesUnified LCPC MC (Template Form)Ian Jun GestaNo ratings yet
- Job Application Form - ExecutiveDocument2 pagesJob Application Form - ExecutiveWan Qing NgNo ratings yet
- BIS Personal Applicant FormDocument3 pagesBIS Personal Applicant FormDanny stampNo ratings yet
- Checklist Grant For Wholesale Drug License PDFDocument11 pagesChecklist Grant For Wholesale Drug License PDFShwetank SinghNo ratings yet
- GP Fund Form BDocument2 pagesGP Fund Form BIrfan ArifNo ratings yet
- Invitation - 1Document8 pagesInvitation - 1amaNo ratings yet
- Soroban Exercises P8cRBjsDocument1 pageSoroban Exercises P8cRBjsSilvia OitaNo ratings yet
- Indigo Plantation and EffectsDocument8 pagesIndigo Plantation and Effectstaran vlogsNo ratings yet
- Imperialism: Imperialism Is A Policy or Ideology of Extending The Rule OverDocument32 pagesImperialism: Imperialism Is A Policy or Ideology of Extending The Rule OverSydknee Lie-onNo ratings yet
- STD VIII NOTES CIVICS CH.5 - JudiciaryDocument3 pagesSTD VIII NOTES CIVICS CH.5 - JudiciaryAnshul DessaiNo ratings yet
- Confession Death Guilt Regrets SinsDocument1 pageConfession Death Guilt Regrets SinsLNo ratings yet
- Purnell L. The Purnell Model For Cultural Competence. Journal of Transcultural NursingDocument10 pagesPurnell L. The Purnell Model For Cultural Competence. Journal of Transcultural NursingCengizhan ErNo ratings yet
- InvoiceDocument1 pageInvoicebshari93_918887308No ratings yet
- Combatting Business To Business Fraud Benchmarking Report TR ACFE 2023Document28 pagesCombatting Business To Business Fraud Benchmarking Report TR ACFE 2023Karina ChuzevilleNo ratings yet
- 1 The Contemporary World ReviewDocument44 pages1 The Contemporary World ReviewKim Mariah AndalesNo ratings yet
- Haryana Staff Selection Commission: Reservation DetailsDocument2 pagesHaryana Staff Selection Commission: Reservation DetailsRimmy BhardwajNo ratings yet
- Buytosell Subscription Form FaqDocument3 pagesBuytosell Subscription Form FaqNWELENo ratings yet
- Deed of Absolute SaleDocument2 pagesDeed of Absolute SaleDenee Vem MatorresNo ratings yet
- USE UNLESS (Remove If) Notes by Vijay Salunke SirDocument2 pagesUSE UNLESS (Remove If) Notes by Vijay Salunke Sirdevrarimanish72No ratings yet
- Hong Kong - Salary Survey - 2021Document6 pagesHong Kong - Salary Survey - 2021Nathan SmithNo ratings yet
- Consti2 - Cases AgainDocument13 pagesConsti2 - Cases AgainChaNo ratings yet
- 03 Handout 1Document4 pages03 Handout 1Katelyn Mae SungcangNo ratings yet
- Price List All Models - ASHDocument1 pagePrice List All Models - ASHSia Siaw LangNo ratings yet
- EO 6 S 2021 - Data-Privacy-Officer-DPO-BarangayDocument2 pagesEO 6 S 2021 - Data-Privacy-Officer-DPO-BarangayBARANGAY MOLINO II100% (2)
- PDF Document 6Document8 pagesPDF Document 6Happi TummyNo ratings yet
- Buen VivirDocument36 pagesBuen VivirJúlia GusmãoNo ratings yet
- Decree 25 2013 v31 of The Ministry of National Development On The Amount of The Toll and Toll Roads Effective As of 15092015Document107 pagesDecree 25 2013 v31 of The Ministry of National Development On The Amount of The Toll and Toll Roads Effective As of 15092015MelecaNo ratings yet
- People VS PalijonDocument3 pagesPeople VS PalijonRyannDeLeonNo ratings yet
- 160526AttyFeeMotionPkgRcvdStamped PDFDocument61 pages160526AttyFeeMotionPkgRcvdStamped PDFStephanie RueNo ratings yet
- Cheng vs. SyDocument9 pagesCheng vs. SyRivera Meriem Grace MendezNo ratings yet
- Living Outside BarsDocument10 pagesLiving Outside BarsLea UnderscoreNo ratings yet
- Candidate For Nomination Profile Template - (2016.01.20)Document1 pageCandidate For Nomination Profile Template - (2016.01.20)nasirNo ratings yet