
Medicare Safety Net Registration and Amendment For Couples and Families
Medicare Safety Net Registration and Amendment For Couples and Families
You might also like
- Su717 2004en F PDFDocument5 pagesSu717 2004en F PDFIrene ChrimesNo ratings yet
- Managing Filipino Teams by Mike GroganDocument107 pagesManaging Filipino Teams by Mike GroganglycerilkayeNo ratings yet
- Very Advanced Maternal Age, TOG-2021Document10 pagesVery Advanced Maternal Age, TOG-2021saeed hasan saeedNo ratings yet
- Disabikity Pension Application Form Sa466-2305en-FDocument35 pagesDisabikity Pension Application Form Sa466-2305en-FdaryltoschNo ratings yet
- Topographic Maps: Use The Following Hiking Map From Enchanted Rock To Complete The Following QuestionsDocument3 pagesTopographic Maps: Use The Following Hiking Map From Enchanted Rock To Complete The Following QuestionsVinujah Sukumaran50% (4)
- Application To Copy or Transfer From One Medicare Card To AnotherDocument5 pagesApplication To Copy or Transfer From One Medicare Card To AnotherGabriel JonathanNo ratings yet
- Australian Immunisation Register Ceasing Correspondence and Release of InformationDocument2 pagesAustralian Immunisation Register Ceasing Correspondence and Release of InformationAshlee0% (2)
- Health Insurance Application FormDocument2 pagesHealth Insurance Application FormFrenzy Taher100% (1)
- Medicare Enrolment Form: When To Use This FormDocument13 pagesMedicare Enrolment Form: When To Use This FormMohsen DehghaniNo ratings yet
- Separation Document - Ss293 1707en PDocument13 pagesSeparation Document - Ss293 1707en PMark LordNo ratings yet
- ms004 2004en F PDFDocument13 pagesms004 2004en F PDFDanielWildSheepZaninNo ratings yet
- Medicare Enrolment Form (MS004) PDFDocument13 pagesMedicare Enrolment Form (MS004) PDFDanielWildSheepZaninNo ratings yet
- A Beginner's Guide to Disability Insurance Claims in Canada: How to Apply for and Win Payment of Disability Insurance Benefits, Even After a Denial or Unsuccessful AppealFrom EverandA Beginner's Guide to Disability Insurance Claims in Canada: How to Apply for and Win Payment of Disability Insurance Benefits, Even After a Denial or Unsuccessful AppealNo ratings yet
- Faculty of Commerce Bachelor of CommerceDocument28 pagesFaculty of Commerce Bachelor of CommercemawandeNo ratings yet
- The Gods of Greece PDFDocument224 pagesThe Gods of Greece PDFCiro Formicola100% (2)
- Application To Copy or Transfer From One Medicare Card To AnotherDocument6 pagesApplication To Copy or Transfer From One Medicare Card To AnotherjetNo ratings yet
- Medicare Enrolment Form: When To Use This Form Aboriginal and Torres Strait Islander AustralianDocument13 pagesMedicare Enrolment Form: When To Use This Form Aboriginal and Torres Strait Islander AustralianbibitindrajayaNo ratings yet
- Application To Copy or Transfer From One Medicare Card To AnotherDocument5 pagesApplication To Copy or Transfer From One Medicare Card To AnotherJoanne SunNo ratings yet
- Sa116b 2212en FDocument4 pagesSa116b 2212en FVaccine ScamNo ratings yet
- Medicare Enrolment Application: Applicant(s) Circumstances and Documents Required When To Use This FormDocument6 pagesMedicare Enrolment Application: Applicant(s) Circumstances and Documents Required When To Use This FormLavneet SinghNo ratings yet
- Ms 004Document17 pagesMs 004mu9241335No ratings yet
- Sa116a 2212en FDocument4 pagesSa116a 2212en FVaccine ScamNo ratings yet
- Medicare Form PDFDocument13 pagesMedicare Form PDFLiz S LandinezNo ratings yet
- Abstudy: Additional InformationDocument20 pagesAbstudy: Additional InformationVaccine ScamNo ratings yet
- Medicare Exemption PDFDocument2 pagesMedicare Exemption PDFAlex PiecesNo ratings yet
- Imprimeeeeee PDFDocument52 pagesImprimeeeeee PDFKarina BarrientosNo ratings yet
- MLE Form - 2017tDocument3 pagesMLE Form - 2017tRaj KumarNo ratings yet
- Carer Payment and - or Carer Allowance Medical Report (SA332a) For A Person - 16 Years or OverDocument8 pagesCarer Payment and - or Carer Allowance Medical Report (SA332a) For A Person - 16 Years or OverWallace DunnNo ratings yet
- Bins 00542Document15 pagesBins 00542iaragaraventabaNo ratings yet
- Comp FormDocument5 pagesComp Formsrsyffy9wfNo ratings yet
- Australian Government Rebate Application FormDocument2 pagesAustralian Government Rebate Application FormGeorge GreerNo ratings yet
- Request For Medicare Claims Information: When To Use This Form Details of Person Making Request 1 2Document4 pagesRequest For Medicare Claims Information: When To Use This Form Details of Person Making Request 1 2kiara.storageNo ratings yet
- Separation Details: This Form Lets Us Know You Have Separated From Your PartnerDocument6 pagesSeparation Details: This Form Lets Us Know You Have Separated From Your PartnerBrooke ZarubinNo ratings yet
- EI - CarePlus - Membership Application Form - DEC2020Document4 pagesEI - CarePlus - Membership Application Form - DEC2020Kunal SeeboruthNo ratings yet
- Walters Shameka 46370 MedicaidrecertappDocument4 pagesWalters Shameka 46370 Medicaidrecertappdoenyka.lewisNo ratings yet
- MetLife Basic GTL CertificateDocument63 pagesMetLife Basic GTL Certificatereddyraj036No ratings yet
- Health and Dental Insurance Coverage: Application ForDocument8 pagesHealth and Dental Insurance Coverage: Application ForDorian GailliardNo ratings yet
- Commonwealth of Australia Statutory Declaration: Purpose of This Form For More InformationDocument4 pagesCommonwealth of Australia Statutory Declaration: Purpose of This Form For More InformationOm KarnNo ratings yet
- Register For A My Health RecordDocument9 pagesRegister For A My Health Recordthe.only.machiavellaNo ratings yet
- HTTPSWWW Servicesaustralia Gov Ausitesdefaultfiles2023-03sa466-2304en-F PDFDocument35 pagesHTTPSWWW Servicesaustralia Gov Ausitesdefaultfiles2023-03sa466-2304en-F PDFsiawashNo ratings yet
- Medicare Two-Way Claim: Purpose of This Form Private Health Insurance Member's Details 1 2 3 4 5Document2 pagesMedicare Two-Way Claim: Purpose of This Form Private Health Insurance Member's Details 1 2 3 4 5lalidawatermarkNo ratings yet
- Health Undertaking: Please Keep This Information Page For Your ReferenceDocument4 pagesHealth Undertaking: Please Keep This Information Page For Your Referencedizzi dagerNo ratings yet
- Social Security Agreement Between Australia and CanadaDocument5 pagesSocial Security Agreement Between Australia and CanadaiuythlitNo ratings yet
- MHD App Form (Trust)Document6 pagesMHD App Form (Trust)mojija5822No ratings yet
- Medicare Care PolicyDocument6 pagesMedicare Care PolicyLeti StarNo ratings yet
- Application To Copy or Transfer From One Medicare Card To AnotherDocument6 pagesApplication To Copy or Transfer From One Medicare Card To AnotherDavid LockeridgeNo ratings yet
- Fs-1-Snap 03-15Document10 pagesFs-1-Snap 03-15benwalterofarrellNo ratings yet
- Disaster Recovery Allowance: NSW Bushfires - September 2019Document16 pagesDisaster Recovery Allowance: NSW Bushfires - September 2019Scott FullerNo ratings yet
- Health Care InstrumentsDocument9 pagesHealth Care InstrumentsarthurNo ratings yet
- Child B2Document9 pagesChild B2myscichowski1985No ratings yet
- Your Dependent Child's Coverage May End SoonDocument3 pagesYour Dependent Child's Coverage May End Soonbigblockz8No ratings yet
- Australian Immunisation Register Ceasing Correspondence and Release of InformationDocument2 pagesAustralian Immunisation Register Ceasing Correspondence and Release of InformationVaccine ScamNo ratings yet
- BHF 01535Document8 pagesBHF 01535AlvinNo ratings yet
- sc2 FormDocument2 pagessc2 Formjanellecavanagh20No ratings yet
- Keep This CardDocument9 pagesKeep This Carddrive jams ANo ratings yet
- Newsletter January 2012Document5 pagesNewsletter January 2012frg_leaderNo ratings yet
- NEST Claim Form Incapacity RetirementDocument4 pagesNEST Claim Form Incapacity RetirementCristian GabrielNo ratings yet
- CH2 Child Benefit Claim Form Internet 05 17Document9 pagesCH2 Child Benefit Claim Form Internet 05 17i1963877No ratings yet
- Budgeting for Infertility: How to Bring Home a Baby Without Breaking the BankFrom EverandBudgeting for Infertility: How to Bring Home a Baby Without Breaking the BankRating: 4.5 out of 5 stars4.5/5 (3)
- Disaster Recovery Services Available to YouFrom EverandDisaster Recovery Services Available to YouRating: 3 out of 5 stars3/5 (1)
- Parent Puzzle: A to Z Guide on Assembling Care for Your ParentsFrom EverandParent Puzzle: A to Z Guide on Assembling Care for Your ParentsNo ratings yet
- Lyrics - More Than AbleDocument2 pagesLyrics - More Than AbleZarita CarranzaNo ratings yet
- English Activity 1Document13 pagesEnglish Activity 1Mika ValenciaNo ratings yet
- Utilization of Agro-Industrial Wastes For The Production of Quality Oyster MushroomsDocument10 pagesUtilization of Agro-Industrial Wastes For The Production of Quality Oyster MushroomsMhelvene AlfarasNo ratings yet
- Nit 2187 3Document62 pagesNit 2187 3Imran MulaniNo ratings yet
- Installing Wonderware InTouch 2014 R2 DevelopmentDocument12 pagesInstalling Wonderware InTouch 2014 R2 DevelopmentARMANDO GALENONo ratings yet
- OO ALV Status Led LightDocument6 pagesOO ALV Status Led LightRam PraneethNo ratings yet
- Course Guide For Simplified Accounting For Entrepreneurs & Professionals (Safe&P)Document7 pagesCourse Guide For Simplified Accounting For Entrepreneurs & Professionals (Safe&P)Darwin Dionisio ClementeNo ratings yet
- Hotkeys ATOM RPGDocument1 pageHotkeys ATOM RPGAlexey KolmakovNo ratings yet
- HahayysDocument30 pagesHahayys2BGrp3Plaza, Anna MaeNo ratings yet
- Introduction To DerivativesDocument9 pagesIntroduction To DerivativesParam ShahNo ratings yet
- Fadi CV 030309Document5 pagesFadi CV 030309fkhaterNo ratings yet
- Pediatric OrthopaedicDocument66 pagesPediatric OrthopaedicDhito RodriguezNo ratings yet
- Paper 8911Document8 pagesPaper 8911IJARSCT JournalNo ratings yet
- Oikonomou Mpegetis S 2014 PHD ThesisDocument352 pagesOikonomou Mpegetis S 2014 PHD ThesisCsillag JanosNo ratings yet
- HH Sheet HANNAHDocument1 pageHH Sheet HANNAHcirohero24No ratings yet
- Nucleic Acid Metabolism Adapted From Zhihong Li Material - May 2024Document79 pagesNucleic Acid Metabolism Adapted From Zhihong Li Material - May 2024Black RavenoidNo ratings yet
- Wedding Vows - What Do They Really MeanDocument28 pagesWedding Vows - What Do They Really Meanpsykosomatik0% (1)
- Template TM1Document104 pagesTemplate TM1Flexi BuboyNo ratings yet
- Annex VI - Final Narrative ReportDocument4 pagesAnnex VI - Final Narrative ReporttijanagruNo ratings yet
- Detail of Common Toilet: Section Elevation C - C' Section Elevation D - D'Document1 pageDetail of Common Toilet: Section Elevation C - C' Section Elevation D - D'RichaNo ratings yet
- Study of A Housing ProjectDocument6 pagesStudy of A Housing ProjectIshraha100% (1)
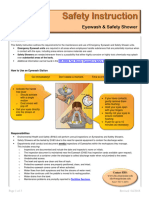
- Eyewash and Safety Shower SiDocument3 pagesEyewash and Safety Shower SiAli EsmaeilbeygiNo ratings yet
- 4.54 A EN DS RDBF01RDBF02RDBF03RDGD01 Sprinkler Guard and Shield FMDocument2 pages4.54 A EN DS RDBF01RDBF02RDBF03RDGD01 Sprinkler Guard and Shield FMAhmad AliNo ratings yet
- Canastilla of Banana LlaneraDocument4 pagesCanastilla of Banana LlaneraValentina AcostaNo ratings yet
- Jescspsu 08Document11 pagesJescspsu 08Alok RanjanNo ratings yet
























































































Download as pdf or txt
You might also like
- Su717 2004en F PDFDocument5 pagesSu717 2004en F PDFIrene ChrimesNo ratings yet
- Managing Filipino Teams by Mike GroganDocument107 pagesManaging Filipino Teams by Mike GroganglycerilkayeNo ratings yet
- Very Advanced Maternal Age, TOG-2021Document10 pagesVery Advanced Maternal Age, TOG-2021saeed hasan saeedNo ratings yet
- Disabikity Pension Application Form Sa466-2305en-FDocument35 pagesDisabikity Pension Application Form Sa466-2305en-FdaryltoschNo ratings yet
- Topographic Maps: Use The Following Hiking Map From Enchanted Rock To Complete The Following QuestionsDocument3 pagesTopographic Maps: Use The Following Hiking Map From Enchanted Rock To Complete The Following QuestionsVinujah Sukumaran50% (4)
- Application To Copy or Transfer From One Medicare Card To AnotherDocument5 pagesApplication To Copy or Transfer From One Medicare Card To AnotherGabriel JonathanNo ratings yet
- Australian Immunisation Register Ceasing Correspondence and Release of InformationDocument2 pagesAustralian Immunisation Register Ceasing Correspondence and Release of InformationAshlee0% (2)
- Health Insurance Application FormDocument2 pagesHealth Insurance Application FormFrenzy Taher100% (1)
- Medicare Enrolment Form: When To Use This FormDocument13 pagesMedicare Enrolment Form: When To Use This FormMohsen DehghaniNo ratings yet
- Separation Document - Ss293 1707en PDocument13 pagesSeparation Document - Ss293 1707en PMark LordNo ratings yet
- ms004 2004en F PDFDocument13 pagesms004 2004en F PDFDanielWildSheepZaninNo ratings yet
- Medicare Enrolment Form (MS004) PDFDocument13 pagesMedicare Enrolment Form (MS004) PDFDanielWildSheepZaninNo ratings yet
- A Beginner's Guide to Disability Insurance Claims in Canada: How to Apply for and Win Payment of Disability Insurance Benefits, Even After a Denial or Unsuccessful AppealFrom EverandA Beginner's Guide to Disability Insurance Claims in Canada: How to Apply for and Win Payment of Disability Insurance Benefits, Even After a Denial or Unsuccessful AppealNo ratings yet
- Faculty of Commerce Bachelor of CommerceDocument28 pagesFaculty of Commerce Bachelor of CommercemawandeNo ratings yet
- The Gods of Greece PDFDocument224 pagesThe Gods of Greece PDFCiro Formicola100% (2)
- Application To Copy or Transfer From One Medicare Card To AnotherDocument6 pagesApplication To Copy or Transfer From One Medicare Card To AnotherjetNo ratings yet
- Medicare Enrolment Form: When To Use This Form Aboriginal and Torres Strait Islander AustralianDocument13 pagesMedicare Enrolment Form: When To Use This Form Aboriginal and Torres Strait Islander AustralianbibitindrajayaNo ratings yet
- Application To Copy or Transfer From One Medicare Card To AnotherDocument5 pagesApplication To Copy or Transfer From One Medicare Card To AnotherJoanne SunNo ratings yet
- Sa116b 2212en FDocument4 pagesSa116b 2212en FVaccine ScamNo ratings yet
- Medicare Enrolment Application: Applicant(s) Circumstances and Documents Required When To Use This FormDocument6 pagesMedicare Enrolment Application: Applicant(s) Circumstances and Documents Required When To Use This FormLavneet SinghNo ratings yet
- Ms 004Document17 pagesMs 004mu9241335No ratings yet
- Sa116a 2212en FDocument4 pagesSa116a 2212en FVaccine ScamNo ratings yet
- Medicare Form PDFDocument13 pagesMedicare Form PDFLiz S LandinezNo ratings yet
- Abstudy: Additional InformationDocument20 pagesAbstudy: Additional InformationVaccine ScamNo ratings yet
- Medicare Exemption PDFDocument2 pagesMedicare Exemption PDFAlex PiecesNo ratings yet
- Imprimeeeeee PDFDocument52 pagesImprimeeeeee PDFKarina BarrientosNo ratings yet
- MLE Form - 2017tDocument3 pagesMLE Form - 2017tRaj KumarNo ratings yet
- Carer Payment and - or Carer Allowance Medical Report (SA332a) For A Person - 16 Years or OverDocument8 pagesCarer Payment and - or Carer Allowance Medical Report (SA332a) For A Person - 16 Years or OverWallace DunnNo ratings yet
- Bins 00542Document15 pagesBins 00542iaragaraventabaNo ratings yet
- Comp FormDocument5 pagesComp Formsrsyffy9wfNo ratings yet
- Australian Government Rebate Application FormDocument2 pagesAustralian Government Rebate Application FormGeorge GreerNo ratings yet
- Request For Medicare Claims Information: When To Use This Form Details of Person Making Request 1 2Document4 pagesRequest For Medicare Claims Information: When To Use This Form Details of Person Making Request 1 2kiara.storageNo ratings yet
- Separation Details: This Form Lets Us Know You Have Separated From Your PartnerDocument6 pagesSeparation Details: This Form Lets Us Know You Have Separated From Your PartnerBrooke ZarubinNo ratings yet
- EI - CarePlus - Membership Application Form - DEC2020Document4 pagesEI - CarePlus - Membership Application Form - DEC2020Kunal SeeboruthNo ratings yet
- Walters Shameka 46370 MedicaidrecertappDocument4 pagesWalters Shameka 46370 Medicaidrecertappdoenyka.lewisNo ratings yet
- MetLife Basic GTL CertificateDocument63 pagesMetLife Basic GTL Certificatereddyraj036No ratings yet
- Health and Dental Insurance Coverage: Application ForDocument8 pagesHealth and Dental Insurance Coverage: Application ForDorian GailliardNo ratings yet
- Commonwealth of Australia Statutory Declaration: Purpose of This Form For More InformationDocument4 pagesCommonwealth of Australia Statutory Declaration: Purpose of This Form For More InformationOm KarnNo ratings yet
- Register For A My Health RecordDocument9 pagesRegister For A My Health Recordthe.only.machiavellaNo ratings yet
- HTTPSWWW Servicesaustralia Gov Ausitesdefaultfiles2023-03sa466-2304en-F PDFDocument35 pagesHTTPSWWW Servicesaustralia Gov Ausitesdefaultfiles2023-03sa466-2304en-F PDFsiawashNo ratings yet
- Medicare Two-Way Claim: Purpose of This Form Private Health Insurance Member's Details 1 2 3 4 5Document2 pagesMedicare Two-Way Claim: Purpose of This Form Private Health Insurance Member's Details 1 2 3 4 5lalidawatermarkNo ratings yet
- Health Undertaking: Please Keep This Information Page For Your ReferenceDocument4 pagesHealth Undertaking: Please Keep This Information Page For Your Referencedizzi dagerNo ratings yet
- Social Security Agreement Between Australia and CanadaDocument5 pagesSocial Security Agreement Between Australia and CanadaiuythlitNo ratings yet
- MHD App Form (Trust)Document6 pagesMHD App Form (Trust)mojija5822No ratings yet
- Medicare Care PolicyDocument6 pagesMedicare Care PolicyLeti StarNo ratings yet
- Application To Copy or Transfer From One Medicare Card To AnotherDocument6 pagesApplication To Copy or Transfer From One Medicare Card To AnotherDavid LockeridgeNo ratings yet
- Fs-1-Snap 03-15Document10 pagesFs-1-Snap 03-15benwalterofarrellNo ratings yet
- Disaster Recovery Allowance: NSW Bushfires - September 2019Document16 pagesDisaster Recovery Allowance: NSW Bushfires - September 2019Scott FullerNo ratings yet
- Health Care InstrumentsDocument9 pagesHealth Care InstrumentsarthurNo ratings yet
- Child B2Document9 pagesChild B2myscichowski1985No ratings yet
- Your Dependent Child's Coverage May End SoonDocument3 pagesYour Dependent Child's Coverage May End Soonbigblockz8No ratings yet
- Australian Immunisation Register Ceasing Correspondence and Release of InformationDocument2 pagesAustralian Immunisation Register Ceasing Correspondence and Release of InformationVaccine ScamNo ratings yet
- BHF 01535Document8 pagesBHF 01535AlvinNo ratings yet
- sc2 FormDocument2 pagessc2 Formjanellecavanagh20No ratings yet
- Keep This CardDocument9 pagesKeep This Carddrive jams ANo ratings yet
- Newsletter January 2012Document5 pagesNewsletter January 2012frg_leaderNo ratings yet
- NEST Claim Form Incapacity RetirementDocument4 pagesNEST Claim Form Incapacity RetirementCristian GabrielNo ratings yet
- CH2 Child Benefit Claim Form Internet 05 17Document9 pagesCH2 Child Benefit Claim Form Internet 05 17i1963877No ratings yet
- Budgeting for Infertility: How to Bring Home a Baby Without Breaking the BankFrom EverandBudgeting for Infertility: How to Bring Home a Baby Without Breaking the BankRating: 4.5 out of 5 stars4.5/5 (3)
- Disaster Recovery Services Available to YouFrom EverandDisaster Recovery Services Available to YouRating: 3 out of 5 stars3/5 (1)
- Parent Puzzle: A to Z Guide on Assembling Care for Your ParentsFrom EverandParent Puzzle: A to Z Guide on Assembling Care for Your ParentsNo ratings yet
- Lyrics - More Than AbleDocument2 pagesLyrics - More Than AbleZarita CarranzaNo ratings yet
- English Activity 1Document13 pagesEnglish Activity 1Mika ValenciaNo ratings yet
- Utilization of Agro-Industrial Wastes For The Production of Quality Oyster MushroomsDocument10 pagesUtilization of Agro-Industrial Wastes For The Production of Quality Oyster MushroomsMhelvene AlfarasNo ratings yet
- Nit 2187 3Document62 pagesNit 2187 3Imran MulaniNo ratings yet
- Installing Wonderware InTouch 2014 R2 DevelopmentDocument12 pagesInstalling Wonderware InTouch 2014 R2 DevelopmentARMANDO GALENONo ratings yet
- OO ALV Status Led LightDocument6 pagesOO ALV Status Led LightRam PraneethNo ratings yet
- Course Guide For Simplified Accounting For Entrepreneurs & Professionals (Safe&P)Document7 pagesCourse Guide For Simplified Accounting For Entrepreneurs & Professionals (Safe&P)Darwin Dionisio ClementeNo ratings yet
- Hotkeys ATOM RPGDocument1 pageHotkeys ATOM RPGAlexey KolmakovNo ratings yet
- HahayysDocument30 pagesHahayys2BGrp3Plaza, Anna MaeNo ratings yet
- Introduction To DerivativesDocument9 pagesIntroduction To DerivativesParam ShahNo ratings yet
- Fadi CV 030309Document5 pagesFadi CV 030309fkhaterNo ratings yet
- Pediatric OrthopaedicDocument66 pagesPediatric OrthopaedicDhito RodriguezNo ratings yet
- Paper 8911Document8 pagesPaper 8911IJARSCT JournalNo ratings yet
- Oikonomou Mpegetis S 2014 PHD ThesisDocument352 pagesOikonomou Mpegetis S 2014 PHD ThesisCsillag JanosNo ratings yet
- HH Sheet HANNAHDocument1 pageHH Sheet HANNAHcirohero24No ratings yet
- Nucleic Acid Metabolism Adapted From Zhihong Li Material - May 2024Document79 pagesNucleic Acid Metabolism Adapted From Zhihong Li Material - May 2024Black RavenoidNo ratings yet
- Wedding Vows - What Do They Really MeanDocument28 pagesWedding Vows - What Do They Really Meanpsykosomatik0% (1)
- Template TM1Document104 pagesTemplate TM1Flexi BuboyNo ratings yet
- Annex VI - Final Narrative ReportDocument4 pagesAnnex VI - Final Narrative ReporttijanagruNo ratings yet
- Detail of Common Toilet: Section Elevation C - C' Section Elevation D - D'Document1 pageDetail of Common Toilet: Section Elevation C - C' Section Elevation D - D'RichaNo ratings yet
- Study of A Housing ProjectDocument6 pagesStudy of A Housing ProjectIshraha100% (1)
- Eyewash and Safety Shower SiDocument3 pagesEyewash and Safety Shower SiAli EsmaeilbeygiNo ratings yet
- 4.54 A EN DS RDBF01RDBF02RDBF03RDGD01 Sprinkler Guard and Shield FMDocument2 pages4.54 A EN DS RDBF01RDBF02RDBF03RDGD01 Sprinkler Guard and Shield FMAhmad AliNo ratings yet
- Canastilla of Banana LlaneraDocument4 pagesCanastilla of Banana LlaneraValentina AcostaNo ratings yet
- Jescspsu 08Document11 pagesJescspsu 08Alok RanjanNo ratings yet