Download as pdf or txt
You might also like
- The Present and Future of Bispecific Antibodies For Cancer TherapyDocument19 pagesThe Present and Future of Bispecific Antibodies For Cancer Therapyvignezh1No ratings yet
- Perjeta Epar Public Assessment Report - enDocument127 pagesPerjeta Epar Public Assessment Report - env9991 v9991No ratings yet
- Breast Cancer ScreeningDocument21 pagesBreast Cancer ScreeningBolivar Isea100% (1)
- ESGO Cervical-Cancer A6 PDFDocument48 pagesESGO Cervical-Cancer A6 PDFRocking ChairNo ratings yet
- ESMO Mama PrimarioDocument23 pagesESMO Mama PrimarioManuel De Jesús FerreirasNo ratings yet
- TrialsDocument7 pagesTrialsthweesha tanejaNo ratings yet
- Ovarian CancerDocument7 pagesOvarian CancerAndi AliNo ratings yet
- 2guia en EmbarazoDocument13 pages2guia en EmbarazoCecilia Quispe JaureguiNo ratings yet
- ESGOESTROESP Guidelines For The Management of Patients With Cervical Cancer - Update 2023Document32 pagesESGOESTROESP Guidelines For The Management of Patients With Cervical Cancer - Update 2023Limbert Rodríguez TiconaNo ratings yet
- Guia Europea Evaluación Lesiones Anexiales PreqxDocument40 pagesGuia Europea Evaluación Lesiones Anexiales PreqxfranciscaNo ratings yet
- ESGO PG Ovarian Cancer Surgery A6 V04 PressDocument16 pagesESGO PG Ovarian Cancer Surgery A6 V04 Press9dc4zvr5vcNo ratings yet
- Predicting The Risk of Malignancy in Adnexal Masses Based On IOTA AJOG 2016Document14 pagesPredicting The Risk of Malignancy in Adnexal Masses Based On IOTA AJOG 2016Fernando Suarez ChumaceroNo ratings yet
- OvarDocument52 pagesOvarAndrei BuruianăNo ratings yet
- Full Title: Accuracy of Clinical Breast Examination's AbnormalitiesDocument21 pagesFull Title: Accuracy of Clinical Breast Examination's AbnormalitiesMaria AyaNo ratings yet
- International Ovarian Tumour Analysis (IOTA) Phase 5Document22 pagesInternational Ovarian Tumour Analysis (IOTA) Phase 5RachnaNo ratings yet
- EAU Guideline 2021Document20 pagesEAU Guideline 2021G WNo ratings yet
- Mottet2016 PDFDocument12 pagesMottet2016 PDFdipawelloiNo ratings yet
- Journal 9Document15 pagesJournal 9Muhammad FaisalNo ratings yet
- Abc3 EsmoDocument18 pagesAbc3 EsmoGerson Mejia ViaNo ratings yet
- European Association of Urology Guidelines On Muscle-Invasive and Metastatic Bladder Cancer: of The 2020 GuidelinesDocument23 pagesEuropean Association of Urology Guidelines On Muscle-Invasive and Metastatic Bladder Cancer: of The 2020 GuidelinesBalqist Asyawa Andra PutriNo ratings yet
- Peccatori2013 PDFDocument11 pagesPeccatori2013 PDFAlfa KaromahNo ratings yet
- Applsci 10 00767 v3Document30 pagesApplsci 10 00767 v3meneeeeeNo ratings yet
- Multiparametric Ultrasound Diagnosis of Breast DiseasesFrom EverandMultiparametric Ultrasound Diagnosis of Breast DiseasesGennady T. SukhikhNo ratings yet
- Cancers 13 02978 v2Document21 pagesCancers 13 02978 v2RevinandaVinaNo ratings yet
- 1 s2.0 S0167814023002207 MainDocument17 pages1 s2.0 S0167814023002207 MainRebeca IbaFerNo ratings yet
- Optical Imaging InbreastsDocument11 pagesOptical Imaging InbreastsCezara RasinarNo ratings yet
- Breast CancerDocument17 pagesBreast CancerLaura CampañaNo ratings yet
- Wiles2017 Article ManagementAndFollow-upOfGallblDocument11 pagesWiles2017 Article ManagementAndFollow-upOfGallblTrần Quốc KhánhNo ratings yet
- ESMO Guideline 2019 - Early Breast Cancer TreatmentDocument27 pagesESMO Guideline 2019 - Early Breast Cancer Treatmentrahma watiNo ratings yet
- Predictors of the risk of fibrosis at 10 years after breast conserving therapy for early breast cancer – A study based on the EORTC trial 22881–10882 ‘boost versus no boost’ / European Journal of Cancer Collette, 2008Document13 pagesPredictors of the risk of fibrosis at 10 years after breast conserving therapy for early breast cancer – A study based on the EORTC trial 22881–10882 ‘boost versus no boost’ / European Journal of Cancer Collette, 2008saipraveen03No ratings yet
- European Society of Urogenital Radiology (ESUR) Guidelines MRI of LeiomyomasDocument13 pagesEuropean Society of Urogenital Radiology (ESUR) Guidelines MRI of LeiomyomasJojo LastNo ratings yet
- Sagesorg-Guidelines For The Use of Laparoscopy During PregnancyDocument32 pagesSagesorg-Guidelines For The Use of Laparoscopy During PregnancyLuis Acosta CumberbatchNo ratings yet
- Magnetic Resonance Imaging of The Breast: Recommendations From The EUSOMA Working GroupDocument21 pagesMagnetic Resonance Imaging of The Breast: Recommendations From The EUSOMA Working GroupNelly ChacónNo ratings yet
- Textbook Breast Disease Diagnosis and Pathology 1St Edition Adnan Aydiner Ebook All Chapter PDFDocument53 pagesTextbook Breast Disease Diagnosis and Pathology 1St Edition Adnan Aydiner Ebook All Chapter PDFmartha.tague296100% (16)
- ESGO-SIOPE Guidelines For The Management of Adolescents and Young Adults With Non-Epithelial Ovarian CancersDocument9 pagesESGO-SIOPE Guidelines For The Management of Adolescents and Young Adults With Non-Epithelial Ovarian CancersAna100% (1)
- The Lancet Volume Issue 2016 (Doi 10.1016/S0140-6736 (16) 31891-8) Harbeck, Nadia Gnant, Michael - Breast CancerDocument17 pagesThe Lancet Volume Issue 2016 (Doi 10.1016/S0140-6736 (16) 31891-8) Harbeck, Nadia Gnant, Michael - Breast CancerAlf RobNo ratings yet
- Ijc 25050Document10 pagesIjc 25050Deviat Ast AmierNo ratings yet
- Clinical Histological and Immunohistochemical Study of Colorectal CarcinomaDocument14 pagesClinical Histological and Immunohistochemical Study of Colorectal Carcinomahappymeluckyme3No ratings yet
- ESMO 5 Advanced Breast CancerDocument27 pagesESMO 5 Advanced Breast CancerAlex DelgadoNo ratings yet
- Acr Practice Parameter For Contrast Mri BreastDocument11 pagesAcr Practice Parameter For Contrast Mri BreastBereanNo ratings yet
- Consenso Internacional Tto NivaDocument15 pagesConsenso Internacional Tto Nivadrluciano.rangelNo ratings yet
- Breast Cancer in Young WomenFrom EverandBreast Cancer in Young WomenOreste GentiliniNo ratings yet
- SEOM TTCC Clinical Guideline in Nasopharynx Cancer 2021Document11 pagesSEOM TTCC Clinical Guideline in Nasopharynx Cancer 2021Giga HasabiNo ratings yet
- Angela Collarino, Sergi Vidal Sicart, Renato A Valdés Olmos NuclearDocument112 pagesAngela Collarino, Sergi Vidal Sicart, Renato A Valdés Olmos NuclearJuan RivasNo ratings yet
- A Major Issue in MedicineDocument29 pagesA Major Issue in MedicineSiti NajwaNo ratings yet
- Diagnostics 10 00103Document13 pagesDiagnostics 10 00103Ahmed NomanNo ratings yet
- Care Pathway of Women With Interval Breast Cancer in 2016 - 2022 - Clinical BreaDocument9 pagesCare Pathway of Women With Interval Breast Cancer in 2016 - 2022 - Clinical BreaAd AdrianaNo ratings yet
- 10 Errores Capitales en EndometriosisDocument13 pages10 Errores Capitales en EndometriosisDavid A Tovar ONo ratings yet
- Best Practice Diagnostic Guidelines For Patients Presenting With Breast SymptomsDocument60 pagesBest Practice Diagnostic Guidelines For Patients Presenting With Breast SymptomsPratamasari Insani100% (2)
- Crems Part 1 2015Document45 pagesCrems Part 1 2015Philip ChiangNo ratings yet
- Cervical Cancer Screening ThesisDocument6 pagesCervical Cancer Screening Thesisbk1svxmr100% (3)
- Introduction ThesisDocument36 pagesIntroduction Thesissourabh jakharNo ratings yet
- Clinical Practice GuidelinesDocument17 pagesClinical Practice GuidelinesPLM 51st National ConventionNo ratings yet
- Cancers 14 01524Document20 pagesCancers 14 01524jNo ratings yet
- 391 RFL 5074533 - 391 RFL 5074533 JDDocument10 pages391 RFL 5074533 - 391 RFL 5074533 JDBibek AcharyaNo ratings yet
- Arab Health Conf Brochure Imaging Diag R7Document6 pagesArab Health Conf Brochure Imaging Diag R7Mitulsinh M RavaljiNo ratings yet
- Ultrasound in Obstet Gyne - 2022 - LandolfoDocument13 pagesUltrasound in Obstet Gyne - 2022 - LandolfoRIRINNo ratings yet
- Hum Reprod Adenomyosis Review 2020Document20 pagesHum Reprod Adenomyosis Review 2020Nguyen ThinhNo ratings yet
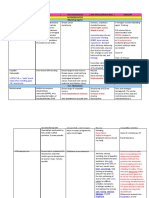
- FARMACO-Biomarker Table With Text 07-12 2023 FINALDocument273 pagesFARMACO-Biomarker Table With Text 07-12 2023 FINALClarice AlhoNo ratings yet
- Roche Upath IVD Algorithm GuideDocument42 pagesRoche Upath IVD Algorithm Guide肥塚泰No ratings yet
- Perjeta Epar Product Information - enDocument43 pagesPerjeta Epar Product Information - enGeo GeoNo ratings yet
- Busting Breast Cancer Myths: A Deep Dive Into Epidemiology, Risk Factors and Effective ManagementDocument20 pagesBusting Breast Cancer Myths: A Deep Dive Into Epidemiology, Risk Factors and Effective ManagementInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Tyrosine Kinase Inhibitor Nilotinib Is More Efficient Than Mitotane in Decreasing Cell Viability in Spheroids Prepared From Adrenocortical Carcinoma CellsDocument16 pagesThe Tyrosine Kinase Inhibitor Nilotinib Is More Efficient Than Mitotane in Decreasing Cell Viability in Spheroids Prepared From Adrenocortical Carcinoma CellsElaine SilveiraNo ratings yet
- pp1 Displayed On Sunday September 09 2007Document94 pagespp1 Displayed On Sunday September 09 2007Лилия ПоляковаNo ratings yet
- Oesophagogastric Cancer Assessment and Management in Adults PDF 1837693014469Document24 pagesOesophagogastric Cancer Assessment and Management in Adults PDF 1837693014469hailemariam gebrehiwotNo ratings yet
- Breast Cancer ReportDocument38 pagesBreast Cancer ReportExcel StephenNo ratings yet
- Breast Cancer 1Document35 pagesBreast Cancer 1Tamalika GhosalNo ratings yet
- TrastuzumabDocument14 pagesTrastuzumabAnaMateiesNo ratings yet
- Drug List WordDocument33 pagesDrug List Wordd clarkeNo ratings yet
- Application of Health Technology Assessment For Oncology Care in IndiaDocument5 pagesApplication of Health Technology Assessment For Oncology Care in Indialaxman kavitkarNo ratings yet
- GenomicDocument3 pagesGenomicAseel AlsheeshNo ratings yet
- Day 4 L2Document90 pagesDay 4 L2yousif.05001467No ratings yet
- 1 s2.0 S0140673623020330 Main 2Document12 pages1 s2.0 S0140673623020330 Main 2Uriel EnriquezNo ratings yet
- Ons Oncc Chemotherapy Immunotherapy Certificate Trial New Update Material Guide With Questions and ADocument19 pagesOns Oncc Chemotherapy Immunotherapy Certificate Trial New Update Material Guide With Questions and Amary011danielNo ratings yet
- Pembrolizumab and Atezolizumab in TNBCDocument11 pagesPembrolizumab and Atezolizumab in TNBCasdffdsaNo ratings yet
- BL BreastDocument14 pagesBL Breastsandhu27152715No ratings yet
- Management of Relapsed Endometrial Cancer After First-Line Chemotherapy - Bradley MonkDocument49 pagesManagement of Relapsed Endometrial Cancer After First-Line Chemotherapy - Bradley Monkinfo7615No ratings yet
- PDF Breast Disease Management and Therapies Volume 2 Adnan Aydiner Ebook Full ChapterDocument53 pagesPDF Breast Disease Management and Therapies Volume 2 Adnan Aydiner Ebook Full Chapterclaire.ayala150100% (3)
- Carcinoma of The Axillary Tail of Spence 2024 International Journal of SurgeDocument4 pagesCarcinoma of The Axillary Tail of Spence 2024 International Journal of SurgeRonald QuezadaNo ratings yet
- Metastatic Diseases Novel Approaches in Diagnosis and Therapeutic Management 1St Edition Sandeep Arora Editor Online Ebook Texxtbook Full Chapter PDFDocument70 pagesMetastatic Diseases Novel Approaches in Diagnosis and Therapeutic Management 1St Edition Sandeep Arora Editor Online Ebook Texxtbook Full Chapter PDFtammy.sage671100% (8)
- 8 Cold Atmospheric Plasma Restores Tamoxifen Sensitivity in Resistant MCF-7Document11 pages8 Cold Atmospheric Plasma Restores Tamoxifen Sensitivity in Resistant MCF-7Ivan Alves de SouzaNo ratings yet
- Breast Cancer Treatment ThesisDocument8 pagesBreast Cancer Treatment Thesisamandamarietopeka100% (2)
- Breast Cancer AssignmentDocument25 pagesBreast Cancer AssignmentTiger KneeNo ratings yet
- ASCO Rapid Update AUG 2022 Metastatic Breast CancerDocument23 pagesASCO Rapid Update AUG 2022 Metastatic Breast CancerAnil RajaniNo ratings yet
- Impact of Eukaryotic Translation Initiation FactorDocument19 pagesImpact of Eukaryotic Translation Initiation FactorMilorad ZjalićNo ratings yet
- Head Neck - 2023 - Weaver - A Molecular Guide To Systemic Therapy in Salivary Gland CarcinomaDocument12 pagesHead Neck - 2023 - Weaver - A Molecular Guide To Systemic Therapy in Salivary Gland CarcinomaafissaNo ratings yet