Download as pdf or txt
You might also like
- Nigerian Law School Medical Centre Bwari-Abuja Hqs Lagos, Enugu, Kano, Yenegoa and Yola Campuses Student'S Personal DataDocument2 pagesNigerian Law School Medical Centre Bwari-Abuja Hqs Lagos, Enugu, Kano, Yenegoa and Yola Campuses Student'S Personal DataIroegbu Mang John100% (1)
- Dengue NS1 RDT Annex 5-6Document4 pagesDengue NS1 RDT Annex 5-6Ga B B Orlongan100% (1)
- Medical Certificate: Department of EducationDocument1 pageMedical Certificate: Department of EducationJo EvangelistaNo ratings yet
- FOH-25 Tuberculosis Screening (M.25)Document1 pageFOH-25 Tuberculosis Screening (M.25)Maria CabañasNo ratings yet
- Verification ReportDocument2 pagesVerification ReportMarvin GamboaNo ratings yet
- General Surgery: Dr. S. Gallinge R Gord On Bud Uhan and Sam Minor, e D Itors Dana M Kay, Associate e D ItorDocument56 pagesGeneral Surgery: Dr. S. Gallinge R Gord On Bud Uhan and Sam Minor, e D Itors Dana M Kay, Associate e D ItorKamran AfzalNo ratings yet
- Concept Map Finished 2Document6 pagesConcept Map Finished 2api-352785497100% (1)
- Dental Itr (Page 1)Document1 pageDental Itr (Page 1)rhu silagoNo ratings yet
- Acute Bloody Diarrhea - CRFDocument2 pagesAcute Bloody Diarrhea - CRFMary Anne Grace Garrido0% (1)
- Case Report Form For HFMDDocument2 pagesCase Report Form For HFMDMendez RhuNo ratings yet
- Non-Neonatal Tetanus: (ICD 10 Code: A35)Document2 pagesNon-Neonatal Tetanus: (ICD 10 Code: A35)CHICKY100% (1)
- Oral Health Examination Record For Teaching and Non Teaching PersonnelDocument1 pageOral Health Examination Record For Teaching and Non Teaching PersonnelAda RicanaNo ratings yet
- Dental Form: Deciduous Maxillary TeethDocument1 pageDental Form: Deciduous Maxillary TeethBianca GermarNo ratings yet
- Case Investigation Form: (For COVID-19 Vaccine AEFI)Document12 pagesCase Investigation Form: (For COVID-19 Vaccine AEFI)Jake RamirezNo ratings yet
- Format of Medical Certificate For Persons With Disabilities (PWD) Name and Address of The Institute/ HospitalDocument1 pageFormat of Medical Certificate For Persons With Disabilities (PWD) Name and Address of The Institute/ HospitalYash ManeNo ratings yet
- Antepartum Record Labor WatchDocument4 pagesAntepartum Record Labor WatchMaryJoy rosalesNo ratings yet
- Chart OdgDocument2 pagesChart Odgkhistine castilloNo ratings yet
- ESR Verification Form ReviseDocument4 pagesESR Verification Form ReviseRouella DoverteNo ratings yet
- Annex A - Self-Assessment Tool For Proposed EPCB Health Facilities PDFDocument5 pagesAnnex A - Self-Assessment Tool For Proposed EPCB Health Facilities PDFCora Mendoza100% (1)
- Gene Xpert FormDocument1 pageGene Xpert FormAina Haravata100% (1)
- Application For DecalDocument3 pagesApplication For DecalJade MaratasNo ratings yet
- Sanitary PermitDocument1 pageSanitary PermitImee CorreaNo ratings yet
- FORM 1 (Application Form)Document2 pagesFORM 1 (Application Form)REX QUILLANo ratings yet
- TB TX CertificationDocument7 pagesTB TX CertificationReinald Raven GuerreroNo ratings yet
- Statement of Acoount For Animal Bite Treatment CenterDocument1 pageStatement of Acoount For Animal Bite Treatment CenterMHIEMHOI100% (2)
- BF Checklist Breastfeeding StationDocument1 pageBF Checklist Breastfeeding StationHoney Abigail Neri100% (1)
- Final Community FormDocument7 pagesFinal Community FormalyanadayritNo ratings yet
- Target Client List FOR: Nutrition & Expanded Program For ImmunizationDocument4 pagesTarget Client List FOR: Nutrition & Expanded Program For ImmunizationJohnmark DubdubanNo ratings yet
- Forms BDocument14 pagesForms BDaryl Joshua SaturnoNo ratings yet
- FWRI Form ReviseDocument3 pagesFWRI Form ReviseJm uniteNo ratings yet
- Cagayan de Oro City College of Nursing Assessment FormDocument12 pagesCagayan de Oro City College of Nursing Assessment Formsticdo_nursing2011No ratings yet
- List of PPAS To Combat Acquired Immune Deficiency SyndromeDocument4 pagesList of PPAS To Combat Acquired Immune Deficiency SyndromeLeonard ArenasNo ratings yet
- Dengue FormDocument2 pagesDengue FormZurc Saquin ApepeNo ratings yet
- CRP Referral Form 2016 Monash Heart V5Document1 pageCRP Referral Form 2016 Monash Heart V5Ansari JavedNo ratings yet
- Post Examination Health Surveillance Form Annex A3 KoronadalDocument1 pagePost Examination Health Surveillance Form Annex A3 KoronadalBricks JauNo ratings yet
- Hospital Discharge Summary Form InstructionsDocument2 pagesHospital Discharge Summary Form Instructionsepi bahoNo ratings yet
- Hso G Medical Examination FormDocument1 pageHso G Medical Examination FormorionsrulerNo ratings yet
- AO 2021-0044 Guidelines On Determining Eligibility For Social Care, Medical and Financial Assistance, and Point of ServiceDocument17 pagesAO 2021-0044 Guidelines On Determining Eligibility For Social Care, Medical and Financial Assistance, and Point of ServiceJonathan delos ReyesNo ratings yet
- Annual Medical ReportDocument6 pagesAnnual Medical ReportVictor Jr MesaNo ratings yet
- Hi - Precision Diagnostics: Medical ReportDocument3 pagesHi - Precision Diagnostics: Medical ReportJoseph LimNo ratings yet
- Voluntary Release-Waiver-Assumption of Risk and Full Indemnity AgreementDocument1 pageVoluntary Release-Waiver-Assumption of Risk and Full Indemnity AgreementJourdan Vigil100% (1)
- Home Against Medical AdviceDocument1 pageHome Against Medical AdvicePia VSNo ratings yet
- Usap Tayo Sa FP Attendance SheetDocument2 pagesUsap Tayo Sa FP Attendance SheetRan DyNo ratings yet
- Medical Certificate: Department of EducationDocument2 pagesMedical Certificate: Department of EducationVanessa R. FloresNo ratings yet
- KIMS Format For Certificate of Medical FitmessDocument1 pageKIMS Format For Certificate of Medical FitmessGovind Pathak AmitNo ratings yet
- Target Client List For Oral Health Care and ServicesDocument8 pagesTarget Client List For Oral Health Care and ServicesLchg KrvyNo ratings yet
- Procurement Plan 2023Document4 pagesProcurement Plan 2023Rhoda DalugdogNo ratings yet
- Form 2a NTP Lab Request FormDocument2 pagesForm 2a NTP Lab Request FormBe Nj100% (1)
- Medical Health RecordDocument1 pageMedical Health RecordNikay SerdeñaNo ratings yet
- AO-2014-0045-A - 1750 Expanded NewbornDocument2 pagesAO-2014-0045-A - 1750 Expanded NewbornRea May NavigarNo ratings yet
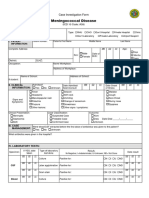
- Case Investigation Form - Meningococcal DiseaseDocument2 pagesCase Investigation Form - Meningococcal Diseaseclaverialc10No ratings yet
- HealthPoint Registration EnglishDocument6 pagesHealthPoint Registration EnglishAnastasia KassaNo ratings yet
- Application Form Blood Collection Unit Blood StationDocument5 pagesApplication Form Blood Collection Unit Blood StationRhodora BenipayoNo ratings yet
- Bemonc Forms RevisedDocument12 pagesBemonc Forms RevisedPhe Pacamarra0% (1)
- CHECKLIST FOR PERSONS UNDER MONITORING (For BHERT Use Only) Re 2019 nCoV ARDDocument1 pageCHECKLIST FOR PERSONS UNDER MONITORING (For BHERT Use Only) Re 2019 nCoV ARDCHICKYNo ratings yet
- Annual Medical Report FormDocument8 pagesAnnual Medical Report Formromulo anascoNo ratings yet
- Assessing The Mouth and PharynxDocument4 pagesAssessing The Mouth and PharynxYudi TrigunaNo ratings yet
- Hso G Dental Form PDFDocument1 pageHso G Dental Form PDFMarlowe SarabiaNo ratings yet
- IELTS YeimirodriguezDocument6 pagesIELTS YeimirodriguezYeimi Rodriguez01No ratings yet
- DOH-HFSRB-QOP01Form1 Rev2 6172022Document3 pagesDOH-HFSRB-QOP01Form1 Rev2 6172022clarisse salvadorNo ratings yet
- Dental Health Record Teaching and Non-Teaching Personnel: Index: DMFTDocument2 pagesDental Health Record Teaching and Non-Teaching Personnel: Index: DMFTEmerson NunezNo ratings yet
- Form 1 Dental RecordDocument2 pagesForm 1 Dental RecordMaico Reyes50% (2)
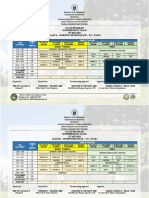
- CLASS-PROGRAM Internediate3Document2 pagesCLASS-PROGRAM Internediate3JohnNo ratings yet
- WLP Q1 W1 PsychosocialDocument6 pagesWLP Q1 W1 PsychosocialJohnNo ratings yet
- Jan 9-13 Week 8 Day 1Document34 pagesJan 9-13 Week 8 Day 1JohnNo ratings yet
- Making StandDocument45 pagesMaking StandJohn100% (1)
- Jan 9-13 Day 2Document27 pagesJan 9-13 Day 2JohnNo ratings yet
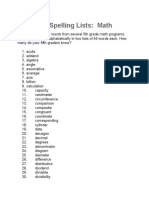
- 5th Grade Spelling ListsDocument12 pages5th Grade Spelling ListsJohnNo ratings yet
- Types of AssessmentDocument33 pagesTypes of AssessmentJohnNo ratings yet
- Mission: DepedDocument15 pagesMission: DepedJohnNo ratings yet
- Seminar: Michael J Seckl, Neil J Sebire, Ross S BerkowitzDocument13 pagesSeminar: Michael J Seckl, Neil J Sebire, Ross S BerkowitzFelicia HalimNo ratings yet
- MIO SheetDocument1 pageMIO SheetjnetNo ratings yet
- Neurology Clerkship Study GuideDocument84 pagesNeurology Clerkship Study GuideHilary Steele100% (1)
- Reco Prostate 2020 2022Document116 pagesReco Prostate 2020 2022Thomas Husson100% (1)
- AGA Technical Review On GI Evaluation of Iron Deficiency AnemiaDocument10 pagesAGA Technical Review On GI Evaluation of Iron Deficiency AnemiaElena ChNo ratings yet
- "Iligtas Sa Tigdas Ang Pinas ": Guide For Vaccination TeamDocument24 pages"Iligtas Sa Tigdas Ang Pinas ": Guide For Vaccination Teamkbl27No ratings yet
- ExaminationofpulseDocument6 pagesExaminationofpulsePeter Paul GollamudiNo ratings yet
- Periodontal Therapy in Older AdultsDocument15 pagesPeriodontal Therapy in Older AdultsPathivada Lumbini100% (1)
- Case Study ON: Blood DyscrasiaDocument40 pagesCase Study ON: Blood DyscrasiaJM RomiasNo ratings yet
- Case Report Trigeminal Neuralgia: Rizka Dana Prastiwi G4A014099 Pembimbing Dr. Untung Gunarto, SP.SDocument12 pagesCase Report Trigeminal Neuralgia: Rizka Dana Prastiwi G4A014099 Pembimbing Dr. Untung Gunarto, SP.SRizka Dana PrastiwiNo ratings yet
- Jcem 0709Document20 pagesJcem 0709Rao Rizwan ShakoorNo ratings yet
- A Rare Cause of Dysphagia - Compression of The Esophagus by An Anterior Cervical Osteophyte Due To Ankylosing SpondylitisDocument5 pagesA Rare Cause of Dysphagia - Compression of The Esophagus by An Anterior Cervical Osteophyte Due To Ankylosing SpondylitisEduardo Lima de Melo Jr.No ratings yet
- GP Osce 1Document3 pagesGP Osce 1Cat NganNo ratings yet
- Nejme 2400102Document3 pagesNejme 2400102linjingwang912No ratings yet
- Impaired Gas ExchangeDocument5 pagesImpaired Gas ExchangeKM67% (3)
- Granuloma AnnulareDocument6 pagesGranuloma AnnulareGitarefinaNo ratings yet
- Abstract Book IOYM 2022Document97 pagesAbstract Book IOYM 2022Mihai PirlogNo ratings yet
- OrchiectomyDocument13 pagesOrchiectomyCherrylyn Raytos0% (1)
- Epidemiologi k3 Revisi-DikonversiDocument16 pagesEpidemiologi k3 Revisi-DikonversiLalisa NisaNo ratings yet
- Pentasa LeafletDocument2 pagesPentasa LeafletreadalotbutnowisdomyetNo ratings yet
- Use of The Hammersmith Infant Neurological Examination in Infants With Cerebral Palsy: A Critical Review of The LiteratureDocument6 pagesUse of The Hammersmith Infant Neurological Examination in Infants With Cerebral Palsy: A Critical Review of The LiteratureshodhgangaNo ratings yet
- Overlooked 150 Year Old Household Cleaner A Remedy For Swine Flu?Document4 pagesOverlooked 150 Year Old Household Cleaner A Remedy For Swine Flu?nsmith7100% (2)
- Dog and Cat Health SecretsDocument70 pagesDog and Cat Health SecretsIvana Dasović100% (1)
- Lecture 12 - Smoking and Health Slides - Sarah JacksonDocument46 pagesLecture 12 - Smoking and Health Slides - Sarah JacksonannaNo ratings yet
- Inflammatory EssayDocument1 pageInflammatory EssayJenny BaiNo ratings yet
- Pharma - M1L1 - Rational Drug PrescribingDocument6 pagesPharma - M1L1 - Rational Drug PrescribingEric Meynard SanchezNo ratings yet
- National Cancer Treatment GuidelinesDocument416 pagesNational Cancer Treatment Guidelinesmelinaabraham2019No ratings yet
- Prof TestDocument13 pagesProf TestOlive NNo ratings yet