Download as pdf or txt
You might also like
- VSIM Clinical Worksheet WORD 06.19Document6 pagesVSIM Clinical Worksheet WORD 06.19Jackie GriffisNo ratings yet
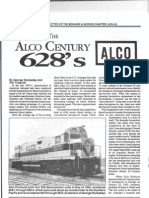
- Alco Century 628'sDocument5 pagesAlco Century 628'sstaustell92100% (1)
- Behavior Intervention PlanDocument4 pagesBehavior Intervention Planapi-505224160100% (1)
- Bengkalis Muria - Jurnal Khusus - Hanifah Hilyah SyahDocument9 pagesBengkalis Muria - Jurnal Khusus - Hanifah Hilyah Syahreza hariansyahNo ratings yet
- Unit 2 - Market SegmentationDocument11 pagesUnit 2 - Market Segmentationlovellmenezes100% (3)
- Regulatory Expert Document-Barry Swanson RevisedDocument3 pagesRegulatory Expert Document-Barry Swanson RevisedVinish SrivastavaNo ratings yet
- First Ward-Based: Early DaysDocument3 pagesFirst Ward-Based: Early DaysMuhammad Zaid SahakNo ratings yet
- HTP-Bed BathingDocument3 pagesHTP-Bed BathingJoanna :DNo ratings yet
- Applying Structured Teaching Principles To Toilet TrainingDocument18 pagesApplying Structured Teaching Principles To Toilet TrainingMabel FreixesNo ratings yet
- Behavior Modification: Presented By: Wajeeha Iqbal BS in Psychology, MS (SLP/T) Riphah College of Rehabilitation SciencesDocument28 pagesBehavior Modification: Presented By: Wajeeha Iqbal BS in Psychology, MS (SLP/T) Riphah College of Rehabilitation Sciencesmazahir hussainNo ratings yet
- Official Action PlanDocument4 pagesOfficial Action Planapi-651948991No ratings yet
- Description of The StrategyDocument7 pagesDescription of The Strategyiulia9gavrisNo ratings yet
- Applying Structured Teaching Principles To Toilet Training: The Child's PerspectiveDocument8 pagesApplying Structured Teaching Principles To Toilet Training: The Child's PerspectiveMaría Ramos ZugastiNo ratings yet
- BEHAVIOR INTERVENTION 05012023 013518amDocument20 pagesBEHAVIOR INTERVENTION 05012023 013518ameemanfatima1261444No ratings yet
- The Beginning Teacher'S Behaviour Toolkit: A SummaryDocument2 pagesThe Beginning Teacher'S Behaviour Toolkit: A SummaryChong Beng LimNo ratings yet
- Potty Training: How To Toilet Train Boys And Girls Overnight; The Best Way To Help Your Toddler With Proven Methods and Tricks; Getting A Beak From Dirty Diapers Is EasyFrom EverandPotty Training: How To Toilet Train Boys And Girls Overnight; The Best Way To Help Your Toddler With Proven Methods and Tricks; Getting A Beak From Dirty Diapers Is EasyNo ratings yet
- Toilet Training For Children With ASDDocument6 pagesToilet Training For Children With ASDZulia ZahirNo ratings yet
- Supporting Program Operations Category lp7Document3 pagesSupporting Program Operations Category lp7api-548033745No ratings yet
- Toilet Training A Skill Development ProgrammeDocument5 pagesToilet Training A Skill Development ProgrammeKidz to Adultz ExhibitionsNo ratings yet
- The Ace Bandage Approach To Digit-Sucking Habits: Clinical SectionDocument3 pagesThe Ace Bandage Approach To Digit-Sucking Habits: Clinical SectionsrinandanNo ratings yet
- Portfolio Project FinalDocument23 pagesPortfolio Project Finalapi-288957404No ratings yet
- Principios Educacion AdultosDocument2 pagesPrincipios Educacion Adultoskaweskar1973No ratings yet
- Inquiries Week 2Document4 pagesInquiries Week 2Bogart YanNo ratings yet
- APPLIED BEHAVIOR ANALYSIS ReportDocument23 pagesAPPLIED BEHAVIOR ANALYSIS ReportCG GumbanNo ratings yet
- Addressing ACEs and Trauma in Primary Care Setting (AAP)Document7 pagesAddressing ACEs and Trauma in Primary Care Setting (AAP)AdvocateforPeds100% (1)
- Back To School e BookDocument10 pagesBack To School e BookDipak DasNo ratings yet
- Behavior TherapyDocument35 pagesBehavior Therapynikos kasiktsisNo ratings yet
- Anyeke PSDocument8 pagesAnyeke PSOkello JimmyNo ratings yet
- ProfedDocument5 pagesProfedAndrea Mae AdanoNo ratings yet
- Thesis On Toilet TrainingDocument6 pagesThesis On Toilet TrainingBuyCollegePaperOnlineSingapore100% (2)
- GoV Caseworkers Handbook 29sept2021Document37 pagesGoV Caseworkers Handbook 29sept2021gatkuothziadaNo ratings yet
- GoV Caseworkers Handbook 29sept2021Document37 pagesGoV Caseworkers Handbook 29sept2021gatkuothziadaNo ratings yet
- Learning Diary and Reading ReportDocument2 pagesLearning Diary and Reading Reporthazel alvarez100% (2)
- Self-Management: An Evidenced-Based Intervention For Autism Spectrum Disorders (Asd)Document6 pagesSelf-Management: An Evidenced-Based Intervention For Autism Spectrum Disorders (Asd)Shahnaz NawazNo ratings yet
- Adaptive ToiletDocument5 pagesAdaptive Toiletmarileks3No ratings yet
- Empathy ResearchDocument1 pageEmpathy Researchapi-605704530No ratings yet
- Behaviour ModificationDocument18 pagesBehaviour ModificationMM 12No ratings yet
- Toilet Training GuideDocument9 pagesToilet Training Guideinvest209100% (1)
- LESSON 5 SPED StudentsDocument6 pagesLESSON 5 SPED StudentsCaryl IvyNo ratings yet
- From Diapers to Big Kid Underwear: A Step-by-Step Potty Training Course for Toddlers and Parents: Course, #1From EverandFrom Diapers to Big Kid Underwear: A Step-by-Step Potty Training Course for Toddlers and Parents: Course, #1No ratings yet
- Lab Report Submission 3 - DiscussionDocument2 pagesLab Report Submission 3 - DiscussionlisavansetersNo ratings yet
- Potty Training NewsletterDocument3 pagesPotty Training NewsletterPammNo ratings yet
- Toileting Nappy ChangingDocument3 pagesToileting Nappy Changingapi-451039239No ratings yet
- Toileting and Nappy Changing Principles and Practices: Quality Area 2Document3 pagesToileting and Nappy Changing Principles and Practices: Quality Area 2api-352133043No ratings yet
- Toilet Training Checklist - CCANDDocument2 pagesToilet Training Checklist - CCANDvyzze kNo ratings yet
- Supporting Appropriate Behavior: Living With AutismDocument4 pagesSupporting Appropriate Behavior: Living With AutismDarkoNo ratings yet
- Guide Managing Challenging BehaviourDocument10 pagesGuide Managing Challenging BehaviourtpckgNo ratings yet
- ElaineDocument18 pagesElaineTrixie De GuzmanNo ratings yet
- Behaviour Modification TechniquesDocument18 pagesBehaviour Modification TechniquesMM 12No ratings yet
- Implementation PlanDocument4 pagesImplementation Planapi-557858701No ratings yet
- Toilet Training: Human Environmental Sciences ExtensionDocument4 pagesToilet Training: Human Environmental Sciences ExtensionMaria Eugenia RomanNo ratings yet
- Lec 5 5th 2019Document13 pagesLec 5 5th 2019ankitabiswas1940No ratings yet
- Business PitchDocument6 pagesBusiness PitchsrishtiNo ratings yet
- Adhd Interventions For ParentsDocument1 pageAdhd Interventions For Parentsandjelaz989No ratings yet
- Excerpt From "Scarcity: Why Having Too Little Means So Much" by Sendhil Mullainathan and Eldar Shafir.Document5 pagesExcerpt From "Scarcity: Why Having Too Little Means So Much" by Sendhil Mullainathan and Eldar Shafir.OnPointRadioNo ratings yet
- Living SkillsDocument8 pagesLiving SkillsSylvia Sylvester MaludaNo ratings yet
- A Building Blocks ModelDocument8 pagesA Building Blocks ModelAnonymous TLQn9SoRRbNo ratings yet
- Teaching Is An Integral Component of Nursing PracticeDocument4 pagesTeaching Is An Integral Component of Nursing PracticeMajorie ArimadoNo ratings yet
- Behaviour and Proffesional EthicsDocument12 pagesBehaviour and Proffesional EthicsalexiusfaustineNo ratings yet
- ACCA Supporting Health Hygiene Skills Sept05Document3 pagesACCA Supporting Health Hygiene Skills Sept05Ana Isabella SimionNo ratings yet
- A Strategic Behaviour Guidance Tool in Paediatric Dentistry: 'Reframing' - An ExperienceDocument3 pagesA Strategic Behaviour Guidance Tool in Paediatric Dentistry: 'Reframing' - An Experiencesilky groverNo ratings yet
- A New Method in Reminder Therapy Technique For Ceasing Digit Sucking Habit in ChildrenDocument3 pagesA New Method in Reminder Therapy Technique For Ceasing Digit Sucking Habit in ChildrensrinandanNo ratings yet
- Reviews: The Brain in Unclassified Mental Retardation. EditedDocument4 pagesReviews: The Brain in Unclassified Mental Retardation. EditedMuhammad Zaid SahakNo ratings yet
- Story: LinseyDocument2 pagesStory: LinseyMuhammad Zaid SahakNo ratings yet
- First Ward-Based: Early DaysDocument3 pagesFirst Ward-Based: Early DaysMuhammad Zaid SahakNo ratings yet
- Mvself: Self Discovery byDocument2 pagesMvself: Self Discovery byMuhammad Zaid SahakNo ratings yet
- Institute News: ProgrammeDocument2 pagesInstitute News: ProgrammeMuhammad Zaid SahakNo ratings yet
- Making Room at Meanwood Park: A Planned Approach: BY D. A. SpencerDocument2 pagesMaking Room at Meanwood Park: A Planned Approach: BY D. A. SpencerMuhammad Zaid SahakNo ratings yet
- Adult Group Homes:: by Alison C. Rosen Research Psychologist, LondonDocument2 pagesAdult Group Homes:: by Alison C. Rosen Research Psychologist, LondonMuhammad Zaid SahakNo ratings yet
- Readers' Letters: 3 PlacesDocument1 pageReaders' Letters: 3 PlacesMuhammad Zaid SahakNo ratings yet
- Briggs: UnderDocument1 pageBriggs: UnderMuhammad Zaid SahakNo ratings yet
- Understanding And: Verity's DoctorsDocument2 pagesUnderstanding And: Verity's DoctorsMuhammad Zaid SahakNo ratings yet
- Evaluating The Ability of and Enabling A Blind Adult With Learning Disability To Sign A Tenancy AgreementDocument7 pagesEvaluating The Ability of and Enabling A Blind Adult With Learning Disability To Sign A Tenancy AgreementMuhammad Zaid SahakNo ratings yet
- Comment: To Be ParticularlyDocument3 pagesComment: To Be ParticularlyMuhammad Zaid SahakNo ratings yet
- Reviews: Options For The R.N.M.SDocument2 pagesReviews: Options For The R.N.M.SMuhammad Zaid SahakNo ratings yet
- Human Resource Management - 1 Prof. Kalyan Chakravarti Department of Basic Courses Indian Institute of Technology, KharagpurDocument35 pagesHuman Resource Management - 1 Prof. Kalyan Chakravarti Department of Basic Courses Indian Institute of Technology, KharagpurIvani KatalNo ratings yet
- Principles of Growth and DevelopmentDocument9 pagesPrinciples of Growth and DevelopmentLj Ferolino92% (13)
- Bullying - Moral Theology ProjectDocument10 pagesBullying - Moral Theology ProjectJaira GayodNo ratings yet
- Biphasic Liquid Dosage FromDocument8 pagesBiphasic Liquid Dosage FromSwaroopSinghJakhar100% (1)
- AngelesDocument9 pagesAngelesjacknewman870100% (1)
- South Indian Food Calorie ChartDocument5 pagesSouth Indian Food Calorie Chartranjit__kayalaNo ratings yet
- FadingDocument10 pagesFadingLê Dương LongNo ratings yet
- 04 Terpenoides CompilationDocument209 pages04 Terpenoides Compilationrustyryan77No ratings yet
- DLL On The Nerve Cell (Kimberly Manahan)Document3 pagesDLL On The Nerve Cell (Kimberly Manahan)Silver RitzNo ratings yet
- Mental Defense MechanismsDocument2 pagesMental Defense Mechanismsjava_biscocho1229100% (2)
- Huduma Wiki HiiDocument20 pagesHuduma Wiki HiiAyatta SteveNo ratings yet
- Active and Passive Insufficiency - PhysiopediaDocument5 pagesActive and Passive Insufficiency - Physiopediateam7MFkkOP YT50% (2)
- Application of System of Linear Equations 2020Document48 pagesApplication of System of Linear Equations 2020Phương Lâm MỹNo ratings yet
- TWI Passivation Report July 2013Document7 pagesTWI Passivation Report July 2013sakshi patilNo ratings yet
- Application of Geochemical Methods in Geothermal ExplorationDocument12 pagesApplication of Geochemical Methods in Geothermal ExplorationJuan JoseNo ratings yet
- IPD Patient History ChecklistDocument2 pagesIPD Patient History ChecklistdrjriNo ratings yet
- Income Tax NotesDocument18 pagesIncome Tax NotesVikash kumarNo ratings yet
- Embragues para Motores EstacionariosDocument12 pagesEmbragues para Motores EstacionariosJiyaYsqn100% (1)
- Biology CH 7 Practice TestDocument6 pagesBiology CH 7 Practice Testvaleria100% (2)
- Up in The AirDocument1 pageUp in The AirMyzheleen RomanNo ratings yet
- Viola DavisDocument1 pageViola DavisGiulia MarmoNo ratings yet
- N-Channel Enhancement Mode MOSFET: Product SummaryDocument5 pagesN-Channel Enhancement Mode MOSFET: Product Summaryserrano.flia.coNo ratings yet
- Pentair Intellibrite 5g Color Led Pool Installation ManualDocument32 pagesPentair Intellibrite 5g Color Led Pool Installation ManualZahidul HasanNo ratings yet
- Montesano Ness LacartarelacionalenterapiadeparejaDocument23 pagesMontesano Ness LacartarelacionalenterapiadeparejaEncuentros y DiálogosNo ratings yet
- Post Traumatic Stress Reactions in Children of War: Journal of Child Psychology and Psychiatry March 1999Document8 pagesPost Traumatic Stress Reactions in Children of War: Journal of Child Psychology and Psychiatry March 1999yuliaNo ratings yet