Download as pdf or txt
You might also like
- Source1CompressorSubstitutionGuide 0814Document227 pagesSource1CompressorSubstitutionGuide 0814DanielGaliciaHernandezNo ratings yet
- PP3 C878e3Document612 pagesPP3 C878e3Ricardo LimaNo ratings yet
- Robotic Technology in Prosthetic Dentistry: A ReviewDocument4 pagesRobotic Technology in Prosthetic Dentistry: A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Robotically Assisted Implantology A Systematic Review From A Young Dental Professionals Perspective I Have No Fear My Dental Robot Is NearDocument6 pagesRobotically Assisted Implantology A Systematic Review From A Young Dental Professionals Perspective I Have No Fear My Dental Robot Is NearAthenaeum Scientific PublishersNo ratings yet
- Rapid Prototyping An Innovative Technique in DentiDocument7 pagesRapid Prototyping An Innovative Technique in DentiShaivi ShrivastavaNo ratings yet
- Accuracy of Dental Implant Surgery Using Dynamic Navigation and Robotic Systems - An in Vitro StudyDocument8 pagesAccuracy of Dental Implant Surgery Using Dynamic Navigation and Robotic Systems - An in Vitro StudyAlejandra MonsalveNo ratings yet
- Optical Coherence Tomography-Guided Robotic Ophtha 221106 220041Document13 pagesOptical Coherence Tomography-Guided Robotic Ophtha 221106 220041MirceaNo ratings yet
- 2024 - Digital Design of A Hybrid Bone and Tooth Supported GuideDocument9 pages2024 - Digital Design of A Hybrid Bone and Tooth Supported GuideLenny GrauNo ratings yet
- Mechatronics Medical Robot For Minimally Invasive Surgeries Design and ImplementationDocument1 pageMechatronics Medical Robot For Minimally Invasive Surgeries Design and ImplementationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Li2019 Article AEye-in-bodyIntegratedSurgeryRDocument14 pagesLi2019 Article AEye-in-bodyIntegratedSurgeryRAbdulkareem 99No ratings yet
- A Systematic Review of The Accuracy of Digital Surgical Guides For Dental ImplantationDocument23 pagesA Systematic Review of The Accuracy of Digital Surgical Guides For Dental ImplantationehabidentNo ratings yet
- A Bimodal Detection-Based Tremor Suppression System For Vascular Interventional Surgery RobotsDocument13 pagesA Bimodal Detection-Based Tremor Suppression System For Vascular Interventional Surgery RobotsAbdulkareem 99No ratings yet
- Artigo 06Document8 pagesArtigo 06Julia PimentelNo ratings yet
- From Implant Planning To Surgical Execution An Integrated Approach For Surgery in Oral ImplantologyDocument10 pagesFrom Implant Planning To Surgical Execution An Integrated Approach For Surgery in Oral ImplantologyDenisa CorneaNo ratings yet
- Applsci 11 02315 v2Document13 pagesApplsci 11 02315 v2fatemasameeraliredaNo ratings yet
- Microrobotics in Endodontics - A ReviewDocument4 pagesMicrorobotics in Endodontics - A ReviewUJ Communication100% (1)
- Digital OrthodonticsDocument16 pagesDigital OrthodonticsDharmapadmi KasilaniNo ratings yet
- Review Article: Trends in Computer-Aided Manufacturing in Prosthodontics: A Review of The Available StreamsDocument15 pagesReview Article: Trends in Computer-Aided Manufacturing in Prosthodontics: A Review of The Available Streamsabdulaziz alzaidNo ratings yet
- Trends in Computer-Aided Manufacturing in Prosthodontics A Review of The Available StreamsDocument16 pagesTrends in Computer-Aided Manufacturing in Prosthodontics A Review of The Available StreamsLinda Garcia PNo ratings yet
- Robotic SurgeryDocument11 pagesRobotic SurgerySam AlatawiNo ratings yet
- Robotic Technology in Foot and Ankle Surgery: A Comprehensive ReviewDocument15 pagesRobotic Technology in Foot and Ankle Surgery: A Comprehensive Reviewzainaalhashimi101No ratings yet
- An Update On Applications of 3D Printing Technologies UsedDocument8 pagesAn Update On Applications of 3D Printing Technologies UsedAlex BurdeNo ratings yet
- Computer-Assisted, Template-Guided Immediate Implant Placement and Loading in The Mandible: A Case ReportDocument9 pagesComputer-Assisted, Template-Guided Immediate Implant Placement and Loading in The Mandible: A Case Reportnesrine boubakriNo ratings yet
- A Visual 3d-Tracking and Positioning Technique For Stereotaxy With CT ScannersDocument11 pagesA Visual 3d-Tracking and Positioning Technique For Stereotaxy With CT Scannershectorkevin2008No ratings yet
- Current Limitations of Surgical RoboticsDocument9 pagesCurrent Limitations of Surgical RoboticsJohn Carlo TambuyatNo ratings yet
- Dental Robotics PresentationDocument12 pagesDental Robotics Presentationapi-707653150No ratings yet
- Periodontology 2000 - 2022 - Chackartchi - Reducing Errors in Guided Implant Surgery To Optimize Treatment OutcomesDocument9 pagesPeriodontology 2000 - 2022 - Chackartchi - Reducing Errors in Guided Implant Surgery To Optimize Treatment OutcomesDr.CdiazNo ratings yet
- Accuracy of The Digital Workflow For Guided Insertion of Orthodontic Palatal Tads: A Step-By-Step 3D AnalysisDocument8 pagesAccuracy of The Digital Workflow For Guided Insertion of Orthodontic Palatal Tads: A Step-By-Step 3D AnalysisThibaut BossuytNo ratings yet
- 2022 CAD CAM Abutment Vs Stock An Update ReviewDocument12 pages2022 CAD CAM Abutment Vs Stock An Update ReviewSonal BaseerNo ratings yet
- The Accuracy of Implant Placement With Computer-GuidedDocument11 pagesThe Accuracy of Implant Placement With Computer-GuidedRyan Ardi PradanaNo ratings yet
- The Development of Computer Aided Manufacturing - PublishedDocument11 pagesThe Development of Computer Aided Manufacturing - PublishedafaqueNo ratings yet
- Continuum Robots For Medical Applications: A SurveyDocument20 pagesContinuum Robots For Medical Applications: A SurveyErwin PerdanaNo ratings yet
- Implant Surgical Guides From The Past To The PresentDocument6 pagesImplant Surgical Guides From The Past To The Presentwaf51No ratings yet
- Dental Robotics and Its Projected Uses in Restorative Dentistry 1Document7 pagesDental Robotics and Its Projected Uses in Restorative Dentistry 1api-707653150No ratings yet
- Buap 6Document11 pagesBuap 6WawawaNo ratings yet
- Application of Autonomous Navigation in RoboticsDocument12 pagesApplication of Autonomous Navigation in RoboticsBasavaraj NavalgundNo ratings yet
- Urologic Robots and Future Directions: Dan Stoianovici, PHDDocument10 pagesUrologic Robots and Future Directions: Dan Stoianovici, PHDavinashjhamechxNo ratings yet
- Isdigitalguidedimplant Surgeryaccurateand Reliable?: Firas Al Yafi,, Brittany Camenisch,, Mohanad Al-SabbaghDocument17 pagesIsdigitalguidedimplant Surgeryaccurateand Reliable?: Firas Al Yafi,, Brittany Camenisch,, Mohanad Al-SabbaghDANTE DELEGUERYNo ratings yet
- Accuracy of Computer-Aided Template-Guided Oral Implant Placement A Prospective Clinical StudyDocument10 pagesAccuracy of Computer-Aided Template-Guided Oral Implant Placement A Prospective Clinical StudyMário LúcioNo ratings yet
- C.E. Credit. Effect of Steam Sterilization On Accuracy of 3D Printed Implant Surgical Guides A Pilot StudyDocument7 pagesC.E. Credit. Effect of Steam Sterilization On Accuracy of 3D Printed Implant Surgical Guides A Pilot Studymarcela fajardoNo ratings yet
- Artificial Intelligence Applications and Ethical Challenges in Oral and Maxillo-Facial Cosmetic Surgery: A Narrative ReviewDocument8 pagesArtificial Intelligence Applications and Ethical Challenges in Oral and Maxillo-Facial Cosmetic Surgery: A Narrative ReviewCatalina Padilla TapiaNo ratings yet
- Reducing Errors in Guided Implant Surgery To Optimize Treatment OutcomesDocument10 pagesReducing Errors in Guided Implant Surgery To Optimize Treatment OutcomesDenisa CorneaNo ratings yet
- Digital IMPLANT Impression TechniquesDocument25 pagesDigital IMPLANT Impression Techniquesjuanandresro93No ratings yet
- Stereolithographic Surgical Template: A Review: Abst TDocument3 pagesStereolithographic Surgical Template: A Review: Abst Tairtifa1No ratings yet
- JCM 10 00704 v2Document18 pagesJCM 10 00704 v2Mrinmayee ThakurNo ratings yet
- 1 s2.0 S2095809920302575 MainDocument9 pages1 s2.0 S2095809920302575 MainWAHYU DWI LESTARINo ratings yet
- Artificial Intelligence in Fixed Implant Prosthodontics: A Retrospective Study of 106 Implant-Supported Monolithic Zirconia Crowns Inserted in The Posterior Jaws of 90 PatientsDocument16 pagesArtificial Intelligence in Fixed Implant Prosthodontics: A Retrospective Study of 106 Implant-Supported Monolithic Zirconia Crowns Inserted in The Posterior Jaws of 90 Patientsanantha narayananNo ratings yet
- Active Upper Limb Prostheses A Review PaperDocument42 pagesActive Upper Limb Prostheses A Review Paperrazankhalife4No ratings yet
- Essay "Is The Surgeon Redundant in The Age of Dental Planning and Workflow"Document24 pagesEssay "Is The Surgeon Redundant in The Age of Dental Planning and Workflow"Gabriel RodriguezNo ratings yet
- 3D Position Tracking Using On Chip Magnetic Sensing in Image Guided Navigation Bronchoscopy PreprintDocument17 pages3D Position Tracking Using On Chip Magnetic Sensing in Image Guided Navigation Bronchoscopy PreprintpadraigNo ratings yet
- Survey On Impact of Robotics On HealthcareDocument8 pagesSurvey On Impact of Robotics On Healthcareharsh3112aNo ratings yet
- Thermocycling Effect On Implant Supported Overdenture Using 3D Printed Peek Bar Following All-On-4 Concept: Randomized Trial-In Vitro StudyDocument16 pagesThermocycling Effect On Implant Supported Overdenture Using 3D Printed Peek Bar Following All-On-4 Concept: Randomized Trial-In Vitro StudyAliaa Wameedh Ramzi AL-OmariNo ratings yet
- Review On Development Status and Key Technologies of Surgical RobotsDocument6 pagesReview On Development Status and Key Technologies of Surgical RobotsAbderaouf BenyammiNo ratings yet
- DR Nandakishore ArticleDocument9 pagesDR Nandakishore ArticleVinod ViswanathanNo ratings yet
- RoboticSurgery An Evolution in PracticeDocument3 pagesRoboticSurgery An Evolution in PracticeJoão Lourenço0% (1)
- Longo Et Al 2021 Augmented Reality, Virtual ReaDocument13 pagesLongo Et Al 2021 Augmented Reality, Virtual ReaLeandro Magno Correa da SilvaNo ratings yet
- Clinical Application of A Stereolithographic Surgical Guide For Simple Positioning of Orthodontic Mini-Implants.Document12 pagesClinical Application of A Stereolithographic Surgical Guide For Simple Positioning of Orthodontic Mini-Implants.Minh ĐạtNo ratings yet
- Radiological Templates and Cad/Cam Surgical Guides-A Literature ReviewDocument37 pagesRadiological Templates and Cad/Cam Surgical Guides-A Literature ReviewMaqbul AlamNo ratings yet
- New Microsoft Office Word Document1Document46 pagesNew Microsoft Office Word Document1rajaishaNo ratings yet
- Development of Porous Medical Implant Scaffolds ViaDocument7 pagesDevelopment of Porous Medical Implant Scaffolds ViajonkNo ratings yet
- Residual Life Prediction and Optimal Maintenance Decision for a Piece of EquipmentFrom EverandResidual Life Prediction and Optimal Maintenance Decision for a Piece of EquipmentNo ratings yet
- Remote Surgery Using A Neuroendovascular InterventDocument4 pagesRemote Surgery Using A Neuroendovascular InterventAbdulkareem 99No ratings yet
- An Error Compensation Method For Surgical Robot BaDocument12 pagesAn Error Compensation Method For Surgical Robot BaAbdulkareem 99No ratings yet
- Robotic Arm For Remote SurgeryDocument19 pagesRobotic Arm For Remote SurgeryAbdulkareem 99No ratings yet
- Current Status of Robot-Assisted Surgery in The CLDocument11 pagesCurrent Status of Robot-Assisted Surgery in The CLAbdulkareem 99No ratings yet
- A Bimodal Detection-Based Tremor Suppression System For Vascular Interventional Surgery RobotsDocument13 pagesA Bimodal Detection-Based Tremor Suppression System For Vascular Interventional Surgery RobotsAbdulkareem 99No ratings yet
- Wearable Biosensors For Human Fatigue Diagnosis ADocument18 pagesWearable Biosensors For Human Fatigue Diagnosis AAbdulkareem 99No ratings yet
- Estimation of The Center of Gravity of The Human Body Using Image ProcessingDocument48 pagesEstimation of The Center of Gravity of The Human Body Using Image ProcessingAbdulkareem 99No ratings yet
- Reappraisal of Telesurgery in The Era of High-SpeeDocument8 pagesReappraisal of Telesurgery in The Era of High-SpeeAbdulkareem 99No ratings yet
- Li2019 Article AEye-in-bodyIntegratedSurgeryRDocument14 pagesLi2019 Article AEye-in-bodyIntegratedSurgeryRAbdulkareem 99No ratings yet
- Ericsson's GSM System Model: SS Switching System AUC HLR MXE MINDocument9 pagesEricsson's GSM System Model: SS Switching System AUC HLR MXE MINtelcoNo ratings yet
- Test Report For Synchronous MachinesDocument60 pagesTest Report For Synchronous MachinesMaria MarcanoNo ratings yet
- G450 Air Conditioning SystemDocument25 pagesG450 Air Conditioning Systemsohaib arifNo ratings yet
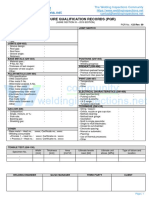
- ASME IX - PQR-All PDFDocument3 pagesASME IX - PQR-All PDFThe Welding Inspections CommunityNo ratings yet
- DX DiagDocument30 pagesDX DiagAadesh PandeyNo ratings yet
- Laboratory Manual Physics of Engineers: Engr. Danielle Joy L. AlcantaraDocument38 pagesLaboratory Manual Physics of Engineers: Engr. Danielle Joy L. AlcantaraSusan LandichoNo ratings yet
- Emcee Script For Math Camp 2023Document3 pagesEmcee Script For Math Camp 2023Analyn Canoy Suazo100% (1)
- PO Communication Methods Technical BriefDocument53 pagesPO Communication Methods Technical BriefWijana NugrahaNo ratings yet
- How To Perform ShortDocument3 pagesHow To Perform Shortbanga_gsNo ratings yet
- Evaluation Fixed Points For The Thermal Calibration Laboratory (Celebrating 10 Years of Slim Cell Production)Document12 pagesEvaluation Fixed Points For The Thermal Calibration Laboratory (Celebrating 10 Years of Slim Cell Production)Arun ChenthamarakshanNo ratings yet
- Creative Media 17-06 PDFDocument21 pagesCreative Media 17-06 PDFsinduja.cseNo ratings yet
- Phenol Removal using Pulsation Bubble Column with Inverse Fluidization airlift Loop Reactor (البحث رقم4)Document8 pagesPhenol Removal using Pulsation Bubble Column with Inverse Fluidization airlift Loop Reactor (البحث رقم4)ali abdulrahman al-ezziNo ratings yet
- ZOD Presentation PDFDocument33 pagesZOD Presentation PDFFelipe Carvajal RodríguezNo ratings yet
- Dsi 700Document30 pagesDsi 700mahh1234No ratings yet
- ES 5 06 0019 - Flange Bolting GuidelinesDocument12 pagesES 5 06 0019 - Flange Bolting Guidelinessam.trags100% (1)
- Uncooled Carbon Microbolometer Imager PDFDocument146 pagesUncooled Carbon Microbolometer Imager PDFamtcorporationNo ratings yet
- Termostato HoneywellDocument48 pagesTermostato HoneywellTámesis LA Tierra Del Siempre VolverNo ratings yet
- ChemDocument6 pagesChemAngela WongNo ratings yet
- Learning Activity SheetDocument6 pagesLearning Activity SheetPOTENCIANO JR TUNAYNo ratings yet
- Asure EssentialsDocument6 pagesAsure EssentialskashyapNo ratings yet
- Kon Boot HelpDocument33 pagesKon Boot Helptmv003No ratings yet
- Pre - Feasibility Study Micro-Hydro SchemeDocument39 pagesPre - Feasibility Study Micro-Hydro SchemeNick_Jeffries100% (2)
- mv110 120 130Document2 pagesmv110 120 130Jorge Martín Cabrera RochaNo ratings yet
- Assembly Word SheetDocument7 pagesAssembly Word SheetnazmulNo ratings yet
- Analysis and Design of Projects in UaeDocument5 pagesAnalysis and Design of Projects in UaealbfaragNo ratings yet
- Anatomy of TypeDocument1 pageAnatomy of Typelunaluna77No ratings yet
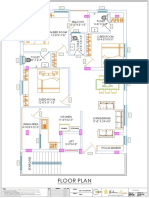
- Rent Building DWG Set 1 PDFDocument6 pagesRent Building DWG Set 1 PDFSai SrimanthNo ratings yet
- Tire Size ChartDocument1 pageTire Size ChartdikidarmawanNo ratings yet