Download as docx, pdf, or txt
You might also like
- Work at Height Permit FormDocument2 pagesWork at Height Permit FormYounis Khan78% (18)
- Permit To Work Form UpdatedDocument3 pagesPermit To Work Form Updatedf.BNo ratings yet
- Heigh Work Pemit - BlueDocument2 pagesHeigh Work Pemit - BlueAravind Babu Dasari100% (6)
- Work at Heights PermitDocument4 pagesWork at Heights Permitrashid zamanNo ratings yet
- Cold Work Permit: The Following Areas / Items Have Been Inspected by Issuer and ReceiverDocument2 pagesCold Work Permit: The Following Areas / Items Have Been Inspected by Issuer and Receiversindarth raveendrakrishnan100% (6)
- Excavation Permit FormDocument2 pagesExcavation Permit FormNash C. Usop100% (1)
- Work at Heights PermitDocument4 pagesWork at Heights PermitFerdinand M. TurbanosNo ratings yet
- Sample Permit To WorkDocument2 pagesSample Permit To WorkPranab AadhiNo ratings yet
- 4 Sample Work at Height PermitDocument2 pages4 Sample Work at Height Permitlam dinhNo ratings yet
- Wah PTWDocument1 pageWah PTWIvan NguyenNo ratings yet
- Permit To Work FormatDocument1 pagePermit To Work FormatManager TrainingNo ratings yet
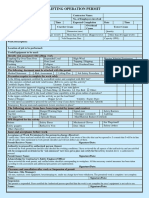
- Lifting Operation PermitDocument2 pagesLifting Operation PermitFMU KSA100% (2)
- Isolation Work PermitDocument2 pagesIsolation Work PermitVijayakumar KarunanidhiNo ratings yet
- Lifting Operation PermitDocument2 pagesLifting Operation Permitsindarth raveendrakrishnan100% (1)
- Work at HDocument2 pagesWork at Hmani narayananNo ratings yet
- Work at Height Permit Form-2020Document2 pagesWork at Height Permit Form-2020Ebrahsm Elshenawy100% (1)
- 14 - Job Safety Analysis-loading and Offloading Materials装卸料Document5 pages14 - Job Safety Analysis-loading and Offloading Materials装卸料Jayvee Baradas Valdez100% (1)
- Light Vehicle Inspection Checklist: Merlinda Pagalan - 0915-8816660Document5 pagesLight Vehicle Inspection Checklist: Merlinda Pagalan - 0915-8816660RCGNo ratings yet
- SICIM Form # JAPL BLUE-Cold Work Permit Rev. 01Document1 pageSICIM Form # JAPL BLUE-Cold Work Permit Rev. 01Farrukh EjazNo ratings yet
- SICIM Form # JAPL BLUE-Cold Work Permit Rev. 01Document2 pagesSICIM Form # JAPL BLUE-Cold Work Permit Rev. 01Farrukh IjazNo ratings yet
- Excavation permit-1-GREENDocument2 pagesExcavation permit-1-GREENAravind Babu Dasari100% (1)
- 17 - Pressure Testing Permit (A4)Document1 page17 - Pressure Testing Permit (A4)Jianping KeNo ratings yet
- JSP For SS No. 5 Tower Crane InstallationDocument15 pagesJSP For SS No. 5 Tower Crane InstallationmohammedtofiqahmedNo ratings yet
- JSP For SS No. 3 Lifting of Heavy Equipment Using CraneDocument14 pagesJSP For SS No. 3 Lifting of Heavy Equipment Using CranemohammedtofiqahmedNo ratings yet
- Work at Height and Work On Near or Over Water - Take 5 Revision Rev FDocument2 pagesWork at Height and Work On Near or Over Water - Take 5 Revision Rev FVicky JiNo ratings yet
- JSP For OHTL No. 11 Access Road and Structure Pad Preparation For High Terrain AreaDocument11 pagesJSP For OHTL No. 11 Access Road and Structure Pad Preparation For High Terrain AreaJaafar LagayanNo ratings yet
- JSP For OHTL No. 16 Erection of Upper Body StructureDocument14 pagesJSP For OHTL No. 16 Erection of Upper Body StructureJaafar Lagayan100% (1)
- Work Permit System Inspection ChecklistDocument2 pagesWork Permit System Inspection ChecklistABDUL RISHAD KunduthodeNo ratings yet
- JSP For OHTL No. 19 Excavation Works For Tower Foundation Pad and ChimneyDocument10 pagesJSP For OHTL No. 19 Excavation Works For Tower Foundation Pad and ChimneyJaafar LagayanNo ratings yet
- JSP For OHTL No. 17 Underline Gantry Installation and ErectionDocument15 pagesJSP For OHTL No. 17 Underline Gantry Installation and ErectionJaafar LagayanNo ratings yet
- Permit To Work Form EnglishDocument1 pagePermit To Work Form EnglishFariz Fatahillah AlbugisiNo ratings yet
- JSP For SS No. 7 PACU InstallationDocument13 pagesJSP For SS No. 7 PACU InstallationJaafar LagayanNo ratings yet
- JSP For OHTL No. 12 Jumper Installation WorksDocument13 pagesJSP For OHTL No. 12 Jumper Installation WorksJaafar LagayanNo ratings yet
- PTW Audit ChecklistDocument3 pagesPTW Audit ChecklistNabi AkramNo ratings yet
- SICIM Form # JAPL GREEN-Confined Space Entry Permit Rev. 01Document1 pageSICIM Form # JAPL GREEN-Confined Space Entry Permit Rev. 01Farrukh Ejaz100% (1)
- Permit To Work: Utracon Construction SDN BHD Utracon Structural Systems SDN BHDDocument2 pagesPermit To Work: Utracon Construction SDN BHD Utracon Structural Systems SDN BHDChe ZahirNo ratings yet
- Working at Height PermitDocument1 pageWorking at Height Permitk.bosanoNo ratings yet
- Permit To Work at Heights: Section 1: ApplicationDocument2 pagesPermit To Work at Heights: Section 1: Applicationvikastiwari171094No ratings yet
- Cold Work Permit Form 2Document2 pagesCold Work Permit Form 2azozinlcNo ratings yet
- Format - Permit To Work 13.02.06 HSE OCP 01 F-01 R1Document4 pagesFormat - Permit To Work 13.02.06 HSE OCP 01 F-01 R1Gaurav Srivats100% (1)
- JSP For SS No. 8 Installation of EOT CraneDocument28 pagesJSP For SS No. 8 Installation of EOT CraneJaafar LagayanNo ratings yet
- 1.PTW AUDIT Dated 16-01-2021Document3 pages1.PTW AUDIT Dated 16-01-2021RakeshNo ratings yet
- JSP For OHTL No. 15 Erection of Common Body StructureDocument14 pagesJSP For OHTL No. 15 Erection of Common Body StructureJaafar LagayanNo ratings yet
- Excavation Work PermitDocument2 pagesExcavation Work Permitmuhammad.younisNo ratings yet
- OHS-PR-09-03-F07 (A) JSP No. 053 Installation of Fiber Optic Cable PanelDocument9 pagesOHS-PR-09-03-F07 (A) JSP No. 053 Installation of Fiber Optic Cable PanelEbrahsm ElshenawyNo ratings yet
- Excavation Permit: The Following Areas / Items Have Been Inspected by Issuer and ReceiverDocument2 pagesExcavation Permit: The Following Areas / Items Have Been Inspected by Issuer and Receiversindarth raveendrakrishnanNo ratings yet
- HSE-12-Working at Height PermitDocument1 pageHSE-12-Working at Height PermitBa N Nhim100% (1)
- JSP For OHTL No. 13 Pilot Wire Paying Out For ConductorsDocument10 pagesJSP For OHTL No. 13 Pilot Wire Paying Out For ConductorsJaafar LagayanNo ratings yet
- BSH Safe Work Method StatementDocument9 pagesBSH Safe Work Method StatementHariprakash karuppannanNo ratings yet
- NEOM Pre Task Briefing Form - New FormatDocument2 pagesNEOM Pre Task Briefing Form - New FormatMohamed HafezNo ratings yet
- Work Permit Audit ChecklistDocument1 pageWork Permit Audit Checklistnitish tiwariNo ratings yet
- Confined Space Work PermitDocument2 pagesConfined Space Work PermitHariharan MuthukrishananNo ratings yet
- Concrete Pouring RAMSDocument19 pagesConcrete Pouring RAMSKaren OlivierNo ratings yet
- PCD-OSH-SF-35 PTW For Confine Space KotaSASDocument2 pagesPCD-OSH-SF-35 PTW For Confine Space KotaSASrizal azizanNo ratings yet
- HEIGHT Work Permit - STTGDCDocument2 pagesHEIGHT Work Permit - STTGDCsttkolkataNo ratings yet
- Form-039-Hydrostatic Testing Work PermitDocument1 pageForm-039-Hydrostatic Testing Work PermitJohn Vincent Macatangay CleofeNo ratings yet
- PCD-OSH-SF-35 PTW For Confine SpaceDocument2 pagesPCD-OSH-SF-35 PTW For Confine Spacerizal azizanNo ratings yet
- Construction Risk in Operational Hospitals: Processes to Ensure Occupant Wellbeing and Minimise DisruptionsFrom EverandConstruction Risk in Operational Hospitals: Processes to Ensure Occupant Wellbeing and Minimise DisruptionsNo ratings yet
- AEL02237 SDS - DISPERBYK-2200 - US - enDocument10 pagesAEL02237 SDS - DISPERBYK-2200 - US - enRıdvan SürmeliNo ratings yet
- Toolbox Talk ChecklistDocument1 pageToolbox Talk ChecklistShafie ZubierNo ratings yet
- MSDS - Haj - B60Document7 pagesMSDS - Haj - B60Future InnovationsNo ratings yet
- Chapter 2Document27 pagesChapter 2محمود محمدNo ratings yet
- Activity 1 - Chemical Safety (GHS-SDS)Document11 pagesActivity 1 - Chemical Safety (GHS-SDS)John Joshua Latras ManticahonNo ratings yet
- HSE-FOR-204-03, PTB CardDocument2 pagesHSE-FOR-204-03, PTB CardMuhammad Atif100% (1)
- Jeyes Safety Data SheetDocument8 pagesJeyes Safety Data Sheetrayshorne939No ratings yet
- General Safety Plan Template: by ThinkhrDocument19 pagesGeneral Safety Plan Template: by ThinkhrRoger Nyipa TadongNo ratings yet
- Material Safety Data Sheet: Section 1 - Chemical Product and Company IdentificationDocument4 pagesMaterial Safety Data Sheet: Section 1 - Chemical Product and Company IdentificationAung SilalaNo ratings yet
- What Steps Are Involved in The Selection of PPEDocument4 pagesWhat Steps Are Involved in The Selection of PPEIain GardnerNo ratings yet
- (The Correlation of Organizational Role Stressors With Stress Level of ICU NursesDocument18 pages(The Correlation of Organizational Role Stressors With Stress Level of ICU NursesAnggriani Puspita AyuNo ratings yet
- Potts Inc Recently Converted From A 5 Day 40 Hour Workweek ToDocument1 pagePotts Inc Recently Converted From A 5 Day 40 Hour Workweek ToMuhammad ShahidNo ratings yet
- Hazard and RiskDocument47 pagesHazard and RiskErica GarcesNo ratings yet
- 50 Reasons Why You Should Put On PPEDocument13 pages50 Reasons Why You Should Put On PPEfatmawaticity.safetyNo ratings yet
- COURSE OUTLINE FOR BOSH 2020 For JULY 20 24Document3 pagesCOURSE OUTLINE FOR BOSH 2020 For JULY 20 24Bos RayNo ratings yet
- Occupational Safty and Health Act 1970Document17 pagesOccupational Safty and Health Act 1970Nitin K RaviNo ratings yet
- Hira HousekeepingDocument1 pageHira Housekeepingspst03792100% (1)
- القيادة الأخلاقية وأثرها في تعزيز سلوك المواطنة التنظيميةDocument18 pagesالقيادة الأخلاقية وأثرها في تعزيز سلوك المواطنة التنظيميةAmanj AmanjNo ratings yet
- Daily OHSE ReportDocument1 pageDaily OHSE ReportNavnath Ambre100% (1)
- Concept Notes Workplace Safety Refers To The Working Environment at A Company and Encompasses All FactorsDocument3 pagesConcept Notes Workplace Safety Refers To The Working Environment at A Company and Encompasses All Factorssushi nakiriNo ratings yet
- Safety Data Sheet: - Made Under Licence of European Label System® Msds Software From Infodyne - HTTPDocument5 pagesSafety Data Sheet: - Made Under Licence of European Label System® Msds Software From Infodyne - HTTPManish KumarNo ratings yet
- Chapter - I - MSDS: Q.1-What Is MSDS? Q.3 - What Q.4 - Where Q.5 - What Q.6 - What Q.7 - Q.8 - WhatDocument36 pagesChapter - I - MSDS: Q.1-What Is MSDS? Q.3 - What Q.4 - Where Q.5 - What Q.6 - What Q.7 - Q.8 - Whatmohammad QutubuddinNo ratings yet
- Chemical SafetyDocument7 pagesChemical SafetyuserytjoniNo ratings yet
- 0 Proven Ingredients For Job Satisfaction: 1. CommunicationDocument26 pages0 Proven Ingredients For Job Satisfaction: 1. CommunicationprabalusamyNo ratings yet
- Safety Data Sheet: 1. Identification of The Substance/Preparation and of The Company/UndertakingDocument9 pagesSafety Data Sheet: 1. Identification of The Substance/Preparation and of The Company/Undertakingdaniel abiaNo ratings yet
- Ge700 2020 Ga24Document6 pagesGe700 2020 Ga24Matthew HillNo ratings yet
- A Review of Literature On Employee Retention: M.S.Kamalaveni, S.Ramesh, T.VetrivelDocument10 pagesA Review of Literature On Employee Retention: M.S.Kamalaveni, S.Ramesh, T.VetrivelGayathrri ShanmugamNo ratings yet
- Managing Risks and Risk Assessment at Work - Useful GuideDocument4 pagesManaging Risks and Risk Assessment at Work - Useful GuideniallNo ratings yet
- Material Safety Data SheetDocument5 pagesMaterial Safety Data SheetTeguh SilaNo ratings yet
- SRL-SDS-8006-28!8!38119-Soda Lime With Indicator Extrapure ARDocument3 pagesSRL-SDS-8006-28!8!38119-Soda Lime With Indicator Extrapure AREVAST FOR CHEMICALSNo ratings yet