Download as pdf or txt
You might also like
- GoldWingGL1800 (2020) CompressedDocument316 pagesGoldWingGL1800 (2020) Compressedchan swantananantNo ratings yet
- Childhood Body Mass Index and Risk of Inflammatory Bowel Disease in Adulthood - A Population-Based Cohort StudyDocument8 pagesChildhood Body Mass Index and Risk of Inflammatory Bowel Disease in Adulthood - A Population-Based Cohort StudyWarren SeowNo ratings yet
- Nutritional Status and Tuberculosis Risk in Adult and Pediatric Household ContactsDocument17 pagesNutritional Status and Tuberculosis Risk in Adult and Pediatric Household ContactshasmawihadriantiNo ratings yet
- Socio-Economic Status Over The Life Course and Obesity: Systematic Review and Meta-AnalysisDocument15 pagesSocio-Economic Status Over The Life Course and Obesity: Systematic Review and Meta-AnalysisAdrián Cuenca MercadoNo ratings yet
- BackgroundDocument16 pagesBackgroundDani KusumaNo ratings yet
- Combination of Measures For Obesity and New-Onset Gallstone Disease 20.16.02Document11 pagesCombination of Measures For Obesity and New-Onset Gallstone Disease 20.16.02hasri ainunNo ratings yet
- Tugas Buk Kasyani Jurnal Sistem Imun Dan ObesitasDocument5 pagesTugas Buk Kasyani Jurnal Sistem Imun Dan ObesitasfideNo ratings yet
- Cureus 0012 00000006929Document11 pagesCureus 0012 00000006929dhaidalganNo ratings yet
- Is BMI The Best Measure of Obesity?: Anthropometric Measures in AdultsDocument4 pagesIs BMI The Best Measure of Obesity?: Anthropometric Measures in AdultsmuthmainnahNo ratings yet
- LC1 BMI and All-Cause Mortality in Older AdultsDocument16 pagesLC1 BMI and All-Cause Mortality in Older AdultsMariNo ratings yet
- 2021 Relation of Body Fat Mass and Fat Free Mass To Total MortalityDocument8 pages2021 Relation of Body Fat Mass and Fat Free Mass To Total MortalityLina M GarciaNo ratings yet
- Association Between Body-Mass Index and Risk of Death in More Than 1 Million AsiansDocument11 pagesAssociation Between Body-Mass Index and Risk of Death in More Than 1 Million AsiansRhinie AstriyanaNo ratings yet
- Park The Impact of Childhood Obesity On MorbidityDocument16 pagesPark The Impact of Childhood Obesity On MorbidityPaty BritoNo ratings yet
- Llewellyn 2015Document12 pagesLlewellyn 2015PriscaArfinesKoesnoNo ratings yet
- 1723-Article Text-7047-4-10-20200605Document7 pages1723-Article Text-7047-4-10-20200605Sarly FebrianaNo ratings yet
- Aogs 101 1364Document10 pagesAogs 101 1364Aina SalsabilaNo ratings yet
- deab224Document11 pagesdeab224ThormmmNo ratings yet
- Diabetes Mellitus Increases The Risk of Active PDFDocument11 pagesDiabetes Mellitus Increases The Risk of Active PDFherry2swNo ratings yet
- A Prospective Study of Obesity and Incidence and Progession of Lower Urinary Tract SymptomsDocument13 pagesA Prospective Study of Obesity and Incidence and Progession of Lower Urinary Tract SymptomssusanaNo ratings yet
- BBLR 5Document10 pagesBBLR 5Firda AureliaNo ratings yet
- 2017 Article 405Document11 pages2017 Article 405Kornelis AribowoNo ratings yet
- Nihms 1518916Document15 pagesNihms 1518916dhaidalganNo ratings yet
- Tuberculosis and Diabetes Mellitus - An Underappreciated AssociationDocument9 pagesTuberculosis and Diabetes Mellitus - An Underappreciated AssociationNajla rayNo ratings yet
- 195 199 WalisDocument5 pages195 199 WalisRajeev NepalNo ratings yet
- Manuscript TBDocument6 pagesManuscript TBsulvitaNo ratings yet
- Nutritional Status and Its Relationship With Blood Pressure Among Children and Adolescents in South ChinaDocument7 pagesNutritional Status and Its Relationship With Blood Pressure Among Children and Adolescents in South ChinautarinuNo ratings yet
- Low Birth Weight and Its Associated Risk Factors: Health Facility-Based Case-Control StudyDocument10 pagesLow Birth Weight and Its Associated Risk Factors: Health Facility-Based Case-Control StudyyasintameganabilaNo ratings yet
- 123-Article Text-270-1-10-20200810Document8 pages123-Article Text-270-1-10-20200810Rosandio Derivanda TranggonoNo ratings yet
- Undesirable Body Mass Index Profiles in Young Adults: No One Is Immune To Obesity Epidemic in PakistanDocument5 pagesUndesirable Body Mass Index Profiles in Young Adults: No One Is Immune To Obesity Epidemic in PakistanDr Alamzeb JadoonNo ratings yet
- BMI HipertensiDocument7 pagesBMI HipertensiAyik M. MandagiNo ratings yet
- 10 5588@ijtld 14 0963Document8 pages10 5588@ijtld 14 0963Oscar Rosero VasconesNo ratings yet
- Luo2020 Article AgeOfObesityOnsetCumulativeObeDocument9 pagesLuo2020 Article AgeOfObesityOnsetCumulativeObehumayrabashirNo ratings yet
- Early Menarche and Teenager Pregnancy As Risk FactorsDocument7 pagesEarly Menarche and Teenager Pregnancy As Risk FactorswidyaNo ratings yet
- INFLAMMATORY Breast CancerDocument20 pagesINFLAMMATORY Breast CancerbencleeseNo ratings yet
- Physical Activity, Abdominal Obesity and The Risk of Coronary Heart Disease: A Korean National Sample StudyDocument7 pagesPhysical Activity, Abdominal Obesity and The Risk of Coronary Heart Disease: A Korean National Sample StudyFrankis De Jesus Vanegas RomeroNo ratings yet
- The Relationship Between Age of Onset and Risk Factors Including Family History and Life Style in Korean Population With Type 2 Diabetes MellitusDocument6 pagesThe Relationship Between Age of Onset and Risk Factors Including Family History and Life Style in Korean Population With Type 2 Diabetes MellitusAulia Nurul IzzahNo ratings yet
- 1Document16 pages1Carlos MelchorNo ratings yet
- Aycan Z 2009Document10 pagesAycan Z 2009qwertyuiopNo ratings yet
- Pediatric Obesity and Cardiometabolic Disorders: Risk Factors and BiomarkersDocument19 pagesPediatric Obesity and Cardiometabolic Disorders: Risk Factors and BiomarkersPriscila Lemasson DuranteNo ratings yet
- Age Dependency of Body Mass Index Distribution in Childhood and Adolescent Inpatients With Anorexia Nervosa With A Focus On DSM-5 and ICD-11 Weight Criteria and Severity SpecifiersDocument14 pagesAge Dependency of Body Mass Index Distribution in Childhood and Adolescent Inpatients With Anorexia Nervosa With A Focus On DSM-5 and ICD-11 Weight Criteria and Severity SpecifiersloloasbNo ratings yet
- CD HAS Bra HortaDocument9 pagesCD HAS Bra HortaAlexandre RochaNo ratings yet
- Writing Project 2 Eng 102Document11 pagesWriting Project 2 Eng 102api-457491124No ratings yet
- Anthropometric Measurements in Childhood and Prediction of Cardiovascular Risk Factors in Adulthood Kaunas Cardiovascular Risk Cohort StudyDocument8 pagesAnthropometric Measurements in Childhood and Prediction of Cardiovascular Risk Factors in Adulthood Kaunas Cardiovascular Risk Cohort Studybrolyssj088No ratings yet
- Complications of Obesity: D. Kinlen, D. Cody and D. O'SheaDocument7 pagesComplications of Obesity: D. Kinlen, D. Cody and D. O'SheaAinun Jariah FahayNo ratings yet
- Anthropometric Measurement To Identify Undernutrition in Cerabral PalsyDocument8 pagesAnthropometric Measurement To Identify Undernutrition in Cerabral PalsyPam Travezani MiyazakiNo ratings yet
- Fnut 08 760437Document9 pagesFnut 08 760437Jerome MontecalvoNo ratings yet
- Relationship of Body Mass Index With Lipid Profile Among Teaching Staff at The Higher Institute of Health Sciences, Sana'aDocument6 pagesRelationship of Body Mass Index With Lipid Profile Among Teaching Staff at The Higher Institute of Health Sciences, Sana'aclaryntafreyaaNo ratings yet
- Bmjopen 2011 000666Document6 pagesBmjopen 2011 000666Fabiola PortugalNo ratings yet
- Chapter 1: IntroductionDocument10 pagesChapter 1: IntroductionSereneBaderNo ratings yet
- Gii and U5 MalnutritionDocument10 pagesGii and U5 MalnutritionAyanHabaneNo ratings yet
- BBH 101h Written Report TBDocument11 pagesBBH 101h Written Report TBapi-608299493No ratings yet
- ObesidadDocument13 pagesObesidadAkiira GarciaNo ratings yet
- Comparison of Different Anthropometric Measures in The Adult Population in Serbia As Indicators of Obesity Data From The National Health Survey 2013Document10 pagesComparison of Different Anthropometric Measures in The Adult Population in Serbia As Indicators of Obesity Data From The National Health Survey 2013snezaimNo ratings yet
- IMC Como Riesgo para Demencia RetrospectivoDocument6 pagesIMC Como Riesgo para Demencia RetrospectivoCarlos AlvaradoNo ratings yet
- Taylor P 2016 IMC y HT NeonatoDocument9 pagesTaylor P 2016 IMC y HT NeonatoYHOISS SMIHT MUNOZ CERONNo ratings yet
- EU Rccm.200611-1717ocDocument6 pagesEU Rccm.200611-1717ocDumitru BiniucNo ratings yet
- The Impact of Obesity On Critical IllnessesDocument21 pagesThe Impact of Obesity On Critical IllnessesrebecarnutNo ratings yet
- Prevalence of Overweight, Obesity and Abdominal Obesity in Bangladeshi University StudentsDocument4 pagesPrevalence of Overweight, Obesity and Abdominal Obesity in Bangladeshi University StudentsTengiz VerulavaNo ratings yet
- 12 Kusrini ICOPH Vol.53 Sup2Document16 pages12 Kusrini ICOPH Vol.53 Sup2Inna 3003No ratings yet
- Fast Facts: Inflammatory Bowel Disease: Translating the science into compassionate IBD careFrom EverandFast Facts: Inflammatory Bowel Disease: Translating the science into compassionate IBD careNo ratings yet
- Oil and Gas ExplorationDocument87 pagesOil and Gas ExplorationVanix DesuasidoNo ratings yet
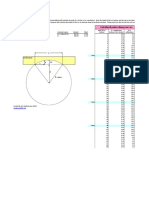
- Arc Layout Calculator: Calculated Points Along Your Arc Enter These ValuesDocument1 pageArc Layout Calculator: Calculated Points Along Your Arc Enter These ValuesPaco PacoNo ratings yet
- List of AGMs Promoted As GMs W.E.F. 25.06.2023Document2 pagesList of AGMs Promoted As GMs W.E.F. 25.06.2023Abhishek ChoubeyNo ratings yet
- 14 CFR Ch. I (1-1-12 Edition) Pt. 25, App. F: Ppendix TO ARTDocument51 pages14 CFR Ch. I (1-1-12 Edition) Pt. 25, App. F: Ppendix TO ARTANA CAROLINA DOS SANTOSNo ratings yet
- Lexmark C500 Menus and MessagesDocument15 pagesLexmark C500 Menus and MessagesjcontractorNo ratings yet
- Stochastic ProcessDocument610 pagesStochastic ProcesshopanzNo ratings yet
- Lesson Plan - Sexual ReproductionDocument3 pagesLesson Plan - Sexual ReproductionHazael Jane BalaisNo ratings yet
- Power Engineering Advances and Challenges. Part A Thermal, Hydro and Nuclear Power by Viorel Badescu, George Cristian Lazaroiu, Linda BarelliDocument458 pagesPower Engineering Advances and Challenges. Part A Thermal, Hydro and Nuclear Power by Viorel Badescu, George Cristian Lazaroiu, Linda BarelliJennifer Cunico100% (1)
- Study of Ashtavinayaka Temples in MaharashtraDocument13 pagesStudy of Ashtavinayaka Temples in MaharashtraRahul RoyNo ratings yet
- Water Needs and Hydration For Cats and Dogs - Brain M.zanghiDocument9 pagesWater Needs and Hydration For Cats and Dogs - Brain M.zanghiann nnNo ratings yet
- Computer GraphicsDocument3 pagesComputer GraphicsGuruKPONo ratings yet
- 1.introduction To How Differentials WorkDocument9 pages1.introduction To How Differentials WorkSameera SdNo ratings yet
- Green Sustainable Airports The Deployment of RenewDocument5 pagesGreen Sustainable Airports The Deployment of Renewcandra trimandokoNo ratings yet
- Shen CoffeDocument3 pagesShen CoffeFood & Beverage ARTOTEL OTISTA BANDUNGNo ratings yet
- Samuel FrimpongDocument14 pagesSamuel Frimpongdunlut pelemNo ratings yet
- WolfDocument3 pagesWolfdsmusicstudioNo ratings yet
- CONVERSATIONS With A - Real Creation StoryDocument60 pagesCONVERSATIONS With A - Real Creation StoryBarb VolkmannNo ratings yet
- Diffusion Coefficient Full Report TiqaDocument19 pagesDiffusion Coefficient Full Report TiqaAtiqah Samad95% (21)
- Project Management in Practice Fifth Edition The World of Project ManagementDocument90 pagesProject Management in Practice Fifth Edition The World of Project ManagementShyair GanglaniNo ratings yet
- Journal of Developmental Psychology. Doi:10.1111/bjdp.12202: VSWM in Children With MLD 1Document27 pagesJournal of Developmental Psychology. Doi:10.1111/bjdp.12202: VSWM in Children With MLD 1Matteo ArcaNo ratings yet
- A Circular Prestressed Concrete Pile Having A Diameter of 40 CM Is To Be Driven in A Layer of Loose SandDocument2 pagesA Circular Prestressed Concrete Pile Having A Diameter of 40 CM Is To Be Driven in A Layer of Loose SandJay Saberdo CayaNo ratings yet
- Business Proposal For Setting Up of A Jacket 2003Document37 pagesBusiness Proposal For Setting Up of A Jacket 2003Abhinav Akash SinghNo ratings yet
- SN1 Vs SN2 PDFDocument1 pageSN1 Vs SN2 PDFHeather UyNo ratings yet
- Section A: Answer Sheet: INBO - 2016 Roll NoDocument9 pagesSection A: Answer Sheet: INBO - 2016 Roll NoDharmendra SinghNo ratings yet
- Pamantasan NG Lungsod NG Maynila Intramuros, ManilaDocument2 pagesPamantasan NG Lungsod NG Maynila Intramuros, ManilaWacko AsahanNo ratings yet
- APM-2024 FlyerDocument2 pagesAPM-2024 FlyeracryptfauNo ratings yet
- TDS Alcomer 216Document2 pagesTDS Alcomer 216PrototypeNo ratings yet
- Welding Code, or AWS D1.1, Structural Welding Code-Steel) To The Construction Division, MaterialsDocument10 pagesWelding Code, or AWS D1.1, Structural Welding Code-Steel) To The Construction Division, MaterialsDak KaizNo ratings yet
- Ping Error MessagesDocument24 pagesPing Error MessagesVijay RubanNo ratings yet