Download as docx, pdf, or txt
You might also like
- Welcome To The Les Mills Instructor PortalDocument4 pagesWelcome To The Les Mills Instructor PortalJNo ratings yet
- Partnership and CorporationDocument15 pagesPartnership and CorporationXyrene Keith MedranoNo ratings yet
- Application Form For Renewal of Registration & 2 or Subsequent Renewal of RegistrationDocument5 pagesApplication Form For Renewal of Registration & 2 or Subsequent Renewal of RegistrationM Irfan Iqbal100% (1)
- Apex Car Rental Agreement BLANKDocument4 pagesApex Car Rental Agreement BLANKSuley KhanNo ratings yet
- Foreign Provisional Permenant RegistrationDocument11 pagesForeign Provisional Permenant RegistrationTina ThomsonNo ratings yet
- GPAT and Gate Pharmacy 3rd Edition: GPAT and Gate Pharmacy 3rd EditionFrom EverandGPAT and Gate Pharmacy 3rd Edition: GPAT and Gate Pharmacy 3rd EditionRating: 4.5 out of 5 stars4.5/5 (6)
- Joining ProformaDocument38 pagesJoining Proformadeepromohanta2021No ratings yet
- Forms To Be Submitted by Provisionally Selected PG Ph.D. Candidates On The Day of AdmissionDocument6 pagesForms To Be Submitted by Provisionally Selected PG Ph.D. Candidates On The Day of Admissionsumit chakrabortyNo ratings yet
- Form of Application For Provisional RegistrationDocument2 pagesForm of Application For Provisional Registrationravi sheladiyaNo ratings yet
- Application Form Ver Date 190913Document5 pagesApplication Form Ver Date 190913Aamir KhanNo ratings yet
- Body Donation Pledge Format EnglishDocument7 pagesBody Donation Pledge Format Englishlingegowda naanuNo ratings yet
- 01 IMA Membership Application FormDocument1 page01 IMA Membership Application Formdrrajak99No ratings yet
- Advertisement For Ayurvedic DoctorDocument2 pagesAdvertisement For Ayurvedic DoctorKirankumar MutnaliNo ratings yet
- Indian Association of EpidemiologistsDocument2 pagesIndian Association of EpidemiologistsAdvanced Research PublicationsNo ratings yet
- Offer Letter - AWS Krishnapattnam - Mr. AbhishekDocument2 pagesOffer Letter - AWS Krishnapattnam - Mr. AbhishekAbhishek KumarNo ratings yet
- Application FormDocument2 pagesApplication FormAbdul GhaffarNo ratings yet
- Application Form: Sub: Application For The Suitable PostDocument5 pagesApplication Form: Sub: Application For The Suitable PostJoseph SmithNo ratings yet
- Medical Fitness Certificate - FormatDocument1 pageMedical Fitness Certificate - FormatAmee PatelNo ratings yet
- Affidavit MergedDocument2 pagesAffidavit MergedabubakarNo ratings yet
- 505 1 Medical Officer 2017Document5 pages505 1 Medical Officer 2017Vivek SinghNo ratings yet
- Annexure - For - PGDIE NITIEDocument5 pagesAnnexure - For - PGDIE NITIEIshika PadhyNo ratings yet
- Rvs Siddha Medical College and Hospital: Application FormDocument2 pagesRvs Siddha Medical College and Hospital: Application Formpsush15No ratings yet
- Membership: Nomination Form For Election ofDocument8 pagesMembership: Nomination Form For Election ofGene ArtsNo ratings yet
- Refresher Course Registration FormDocument2 pagesRefresher Course Registration FormParth OzaNo ratings yet
- PSIT DocsDocument2 pagesPSIT DocsVillageSchool FoundationNo ratings yet
- Curriculum Vitae FDocument3 pagesCurriculum Vitae FYogendra Prawin KumarNo ratings yet
- Enclosures To Application Form For PG Medical CoursesDocument6 pagesEnclosures To Application Form For PG Medical CoursesvigneshNo ratings yet
- Subject: Application For Getting Permission To Carry Out Research Work As A M.D./ M.S. - PG StudentDocument9 pagesSubject: Application For Getting Permission To Carry Out Research Work As A M.D./ M.S. - PG Studentumesh chhotalaNo ratings yet
- Microdanny@Document2 pagesMicrodanny@riyasayadathilNo ratings yet
- Form New Format PDFDocument13 pagesForm New Format PDFANCIENT MYSTERIES OF THE WORLDNo ratings yet
- Application Form For Permanent RegistrationDocument6 pagesApplication Form For Permanent Registrationtejbirsingh2013No ratings yet
- Registration Form (By Email) : 3 International Conference On "Business Ethics, Governance and Sustainable Enterprises"Document2 pagesRegistration Form (By Email) : 3 International Conference On "Business Ethics, Governance and Sustainable Enterprises"Akjm Abdul KadirNo ratings yet
- Mohi-ud-Din Islamic Medical College Sector D-4, Mirpur (AJ&K) Application FormDocument2 pagesMohi-ud-Din Islamic Medical College Sector D-4, Mirpur (AJ&K) Application FormUsama TariqNo ratings yet
- W A M R P ?: HAT RE Y Ights As A ArticipantDocument3 pagesW A M R P ?: HAT RE Y Ights As A ArticipantJack TedescoNo ratings yet
- Intenshiop ............... 2Document1 pageIntenshiop ............... 2Ajay MandraiNo ratings yet
- EligibilityDocument2 pagesEligibilityprashant singhNo ratings yet
- Rajkumar RESUME 2018 PDFDocument3 pagesRajkumar RESUME 2018 PDFLovely ŔâjNo ratings yet
- Job Application FormDocument8 pagesJob Application FormRahim BuxNo ratings yet
- Accreditation FormDocument2 pagesAccreditation FormArnab BhattacharyaNo ratings yet
- Association of Microbiologists of India: Membership Form 2013-2014Document2 pagesAssociation of Microbiologists of India: Membership Form 2013-2014Dr. mukeshNo ratings yet
- Senior Residents & Senior Demonstrators - Annexure 1 & IIDocument3 pagesSenior Residents & Senior Demonstrators - Annexure 1 & IIsarath6872No ratings yet
- Ad DieticianDocument4 pagesAd DieticianTanmoy Pal ChowdhuryNo ratings yet
- Curriculum Vitae: Contact No: 9066124424,6302880988Document2 pagesCurriculum Vitae: Contact No: 9066124424,6302880988indraNo ratings yet
- Ousl Index No 535267Document1 pageOusl Index No 535267Yethmini PereraNo ratings yet
- AffidaviteDocument2 pagesAffidavitePatel OmNo ratings yet
- 1749 Appointment Order Anesthesia Asst - Prof - DR - KhushaliDocument1 page1749 Appointment Order Anesthesia Asst - Prof - DR - Khushalimakwanadrashti1998No ratings yet
- Membership Form / Application For MembershipDocument2 pagesMembership Form / Application For MembershipIron XculptNo ratings yet
- PIMS Annexures MBBS-Admissions-2022Document9 pagesPIMS Annexures MBBS-Admissions-2022Hks HksNo ratings yet
- 2 Application Form Study in SathyabamaDocument2 pages2 Application Form Study in SathyabamaVENKATESH ALISHAMNo ratings yet
- SBCG Training ApplicationDocument3 pagesSBCG Training ApplicationsensiblebusinessNo ratings yet
- National Institute of Ayurveda: Brochure 2019Document6 pagesNational Institute of Ayurveda: Brochure 2019Dhaval KB VyasNo ratings yet
- Tutors Recrut.2017Document3 pagesTutors Recrut.2017Kirankumar MutnaliNo ratings yet
- Application Form For VITEEE - 2013: Full Name Arpit Shringi Application. No.: 2013012259Document2 pagesApplication Form For VITEEE - 2013: Full Name Arpit Shringi Application. No.: 2013012259Arpit ShringiNo ratings yet
- The Thinking Healthy Program - Peer-Delivered Study (THPP) : Final Outcome AssessmentDocument3 pagesThe Thinking Healthy Program - Peer-Delivered Study (THPP) : Final Outcome AssessmentAttalah MohamedNo ratings yet
- LTD Following Are The Terms and Conditions:: BangaloreDocument1 pageLTD Following Are The Terms and Conditions:: BangaloreBLR MGHNo ratings yet
- Bond Anki TDocument4 pagesBond Anki Tamitkumaramit7No ratings yet
- M e PH D Admission Application FormDocument9 pagesM e PH D Admission Application FormAjay GuptaNo ratings yet
- Advertisment and Application Form For Various Post Under MRHRU PunjabDocument4 pagesAdvertisment and Application Form For Various Post Under MRHRU Punjabgamingchan.999No ratings yet
- Directorate of Ayush, Haryana (Government of Haryana) : Advertisement For RecruitmentDocument8 pagesDirectorate of Ayush, Haryana (Government of Haryana) : Advertisement For RecruitmentRenuka KhatkarNo ratings yet
- National Fire Safety College Admission FormDocument2 pagesNational Fire Safety College Admission Formsaad.bagwanNo ratings yet
- Acceptance Form For MDCAT Supervisory StaffDocument1 pageAcceptance Form For MDCAT Supervisory Stafftooba51No ratings yet
- Mediclaim FormDocument1 pageMediclaim Formpicrush2pmNo ratings yet
- Medical Billing & Coding Demystified, 2nd EditionFrom EverandMedical Billing & Coding Demystified, 2nd EditionRating: 2.5 out of 5 stars2.5/5 (2)
- File1 NursingDocument3 pagesFile1 Nursingvishaljames PadharNo ratings yet
- Igmpi Prospectus PHHMDocument76 pagesIgmpi Prospectus PHHMvishaljames PadharNo ratings yet
- Professional CertificationsDocument92 pagesProfessional Certificationsvishaljames PadharNo ratings yet
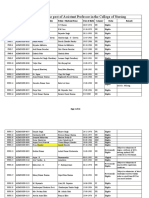
- Interview List For The Post of Assistant Professor in College of Nursing 1Document10 pagesInterview List For The Post of Assistant Professor in College of Nursing 1vishaljames PadharNo ratings yet
- Dmms Medical and Nursing Academy Study Handwritten NoteDocument234 pagesDmms Medical and Nursing Academy Study Handwritten Notevishaljames PadharNo ratings yet
- Result of The Faculty Group A Post 1Document3 pagesResult of The Faculty Group A Post 1vishaljames PadharNo ratings yet
- WP 13915 2019 Order 09-Jul-2022 DigiDocument1 pageWP 13915 2019 Order 09-Jul-2022 Digivishaljames PadharNo ratings yet
- Interview Schedule For Nursing Faculty 21.01.2023 1Document2 pagesInterview Schedule For Nursing Faculty 21.01.2023 1vishaljames PadharNo ratings yet
- Nursing Section DetaDocument6 pagesNursing Section Detavishaljames PadharNo ratings yet
- GFDC VisionDocument20 pagesGFDC Visionvishaljames PadharNo ratings yet
- List Staffnurse21082021Document6 pagesList Staffnurse21082021vishaljames PadharNo ratings yet
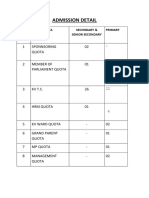
- Admission DetailDocument1 pageAdmission Detailvishaljames PadharNo ratings yet
- WP 12202 2017 Order 24-Feb-2023 DigiDocument1 pageWP 12202 2017 Order 24-Feb-2023 Digivishaljames PadharNo ratings yet
- NUID CardDocument136 pagesNUID Cardvishaljames Padhar100% (1)
- All DLSA Secreataries Mob NoDocument2 pagesAll DLSA Secreataries Mob Novishaljames PadharNo ratings yet
- Theorizing The Organization and Management of Ngos: July 2003Document22 pagesTheorizing The Organization and Management of Ngos: July 2003vishaljames PadharNo ratings yet
- Group 5 2020 Revised Rulebook 5Document3 pagesGroup 5 2020 Revised Rulebook 5vishaljames PadharNo ratings yet
- Tehsil Legal Services CommitteeDocument16 pagesTehsil Legal Services Committeevishaljames PadharNo ratings yet
- Nivesh Scheme 2020Document44 pagesNivesh Scheme 2020vishaljames PadharNo ratings yet
- Quotation Quotation: Macula HealthcareDocument1 pageQuotation Quotation: Macula Healthcarevishaljames PadharNo ratings yet
- Invoice Jail Adhikshak 23.06.2021Document1 pageInvoice Jail Adhikshak 23.06.2021vishaljames PadharNo ratings yet
- Important Dates - NORCET2021Document1 pageImportant Dates - NORCET2021vishaljames PadharNo ratings yet
- The Selection of The Civil Engineer, Salary and Project CostDocument7 pagesThe Selection of The Civil Engineer, Salary and Project CostLevien Jan Dela RosaNo ratings yet
- G.R. No. 94149Document4 pagesG.R. No. 94149Zainne Sarip BandingNo ratings yet
- School of Law and Governance: Submitted To:-Submitted ByDocument18 pagesSchool of Law and Governance: Submitted To:-Submitted Bysuruchi suman 125No ratings yet
- Business Ethics TheoryDocument27 pagesBusiness Ethics TheoryrupaliNo ratings yet
- 1Document7 pages1Hawdin MariwanNo ratings yet
- EnglishDocument24 pagesEnglishyesica rojasNo ratings yet
- HistoryDocument10 pagesHistorySushantika ChakravorttyNo ratings yet
- Letter, Rationale and QuestionnaireDocument3 pagesLetter, Rationale and QuestionnaireLordannie John LanzoNo ratings yet
- Core Periphery (Regional Planning)Document6 pagesCore Periphery (Regional Planning)mrkkenflo80% (5)
- Resolution No. 3 S 2021 First Time Jobseekers Act Today March 19Document9 pagesResolution No. 3 S 2021 First Time Jobseekers Act Today March 19BARANGAY MOLINO IINo ratings yet
- Hungary in The First World WarDocument3 pagesHungary in The First World WarRyan LiebhaberNo ratings yet
- Tulsa Race Riot WebquestDocument6 pagesTulsa Race Riot WebquestIan WilsonNo ratings yet
- The Pacific War 1941-45: Empire of The SunDocument56 pagesThe Pacific War 1941-45: Empire of The SunIvánNo ratings yet
- Selling Process of The Insurance ProductsDocument35 pagesSelling Process of The Insurance ProductsAshish AgarwalNo ratings yet
- Umsc-Constitution 231130 124045Document28 pagesUmsc-Constitution 231130 124045ibrasebsNo ratings yet
- 5 Star Resort - Broker AgreementDocument6 pages5 Star Resort - Broker AgreementDiego AntuneNo ratings yet
- KIGUMODocument3 pagesKIGUMODENNISNo ratings yet
- Environment in Twenty Pages - For UPSC Civi - Baranwal, Varunkumar Baranwal, VarunkumarDocument36 pagesEnvironment in Twenty Pages - For UPSC Civi - Baranwal, Varunkumar Baranwal, Varunkumaramit100% (1)
- Special Release 2020 CPH Population Counts July 13 2021 - 2Document10 pagesSpecial Release 2020 CPH Population Counts July 13 2021 - 2AshNo ratings yet
- Ctr. For Biological Diversity v. McAleenanDocument27 pagesCtr. For Biological Diversity v. McAleenanJohn BinderNo ratings yet
- Criminal Law Art 293-294Document22 pagesCriminal Law Art 293-294Zen ArinesNo ratings yet
- Federal Criminal Complaint Against Jared LoughnerDocument6 pagesFederal Criminal Complaint Against Jared LoughnerVOA NewsNo ratings yet
- Unit 2 Contract and Its ElementsDocument4 pagesUnit 2 Contract and Its ElementsZaya SapkotaNo ratings yet
- Chapter 3 - BudgetDocument17 pagesChapter 3 - BudgetDesiree Faith GaholNo ratings yet
- Tertiary Level Hospital: SL Name of Facility Email Phone / MobileDocument1 pageTertiary Level Hospital: SL Name of Facility Email Phone / MobileRabbir AhmedNo ratings yet
- Francha Compilation Q and ADocument53 pagesFrancha Compilation Q and ARuth Cinco ManocanNo ratings yet
- 1.2.ag. 3. Social Differentiation and StratificationDocument10 pages1.2.ag. 3. Social Differentiation and StratificationSamiya ZamanNo ratings yet