Download as pdf or txt
You might also like
- Strahlenfolter - REMOTE NEURAL MONITORING - Greatdreams - Com - RNMDocument28 pagesStrahlenfolter - REMOTE NEURAL MONITORING - Greatdreams - Com - RNMFred_BlankeNo ratings yet
- Different Subtypes of DyskineticDocument8 pagesDifferent Subtypes of DyskineticMariana CarneiroNo ratings yet
- Pediatric Neurology: Hye-Ryun Yeh MD, Min-Jee Kim MD, Tae-Sung Ko MD, PHD, Mi-Sun Yum MD, PHD, Su-Jeong You MD, PHDDocument6 pagesPediatric Neurology: Hye-Ryun Yeh MD, Min-Jee Kim MD, Tae-Sung Ko MD, PHD, Mi-Sun Yum MD, PHD, Su-Jeong You MD, PHDAdrian KhomanNo ratings yet
- 1 s2.0 S0890856714004079 MainDocument10 pages1 s2.0 S0890856714004079 MainPar DoNo ratings yet
- Brainstem LesionsDocument7 pagesBrainstem LesionsErnesto Ochoa MonroyNo ratings yet
- 1 s2.0 S1059131119305783 MainDocument8 pages1 s2.0 S1059131119305783 MainHappy PramandaNo ratings yet
- Diagnostic HydrocephalDocument5 pagesDiagnostic HydrocephalTiffany NurzamanNo ratings yet
- (31 36) V9N5PTDocument6 pages(31 36) V9N5PTASD2019No ratings yet
- Outcomes of Colorado Children With Acute Flaccid Myelitis at 1 YearDocument9 pagesOutcomes of Colorado Children With Acute Flaccid Myelitis at 1 YearShelbie WattsNo ratings yet
- Cortical Tubers, Cognition, and Epilepsy in Tuberous SclerosisDocument5 pagesCortical Tubers, Cognition, and Epilepsy in Tuberous SclerosisR BNo ratings yet
- Franca (2019) World NeurosurgDocument8 pagesFranca (2019) World NeurosurgCarina FrançaNo ratings yet
- Bayley ScalesDocument4 pagesBayley ScalesPame SniezhkinNo ratings yet
- Patterns of Atrophy in Pathologically Confirmed Dementias: A Voxelwise AnalysisDocument9 pagesPatterns of Atrophy in Pathologically Confirmed Dementias: A Voxelwise AnalysisCaramel luvNo ratings yet
- Opsoclonus-Myoclonus in Children Associated or Not With NeuroblastomaDocument10 pagesOpsoclonus-Myoclonus in Children Associated or Not With Neuroblastomapengchuan72No ratings yet
- Liu Et Al. (2019)Document6 pagesLiu Et Al. (2019)viniciuskiss99No ratings yet
- Epilepsy in Children With Cerebral PalsyDocument6 pagesEpilepsy in Children With Cerebral PalsyTiara Renita LestariNo ratings yet
- Cerebral Palsy in NorwayDocument10 pagesCerebral Palsy in NorwayЯковлев АлександрNo ratings yet
- Cervical DyatoniaDocument6 pagesCervical DyatoniaEmad Moody KaremNo ratings yet
- Dysembryoplastic Neuroepithelial Tumors in Childhood: Long-Term Outcome and Prognostic FeaturesDocument7 pagesDysembryoplastic Neuroepithelial Tumors in Childhood: Long-Term Outcome and Prognostic Featureslucasher35No ratings yet
- Long-Term Outcomes After Surgical Treatment of Pediatric Neurogenic Thoracic Outlet SyndromeDocument11 pagesLong-Term Outcomes After Surgical Treatment of Pediatric Neurogenic Thoracic Outlet Syndromewalter fire 0057No ratings yet
- Surgical Management and Long-Term Outcome of Pediatric Patients With Different Subtypes of Epilepsy Associated With Cerebral Cavernous MalformationsDocument7 pagesSurgical Management and Long-Term Outcome of Pediatric Patients With Different Subtypes of Epilepsy Associated With Cerebral Cavernous MalformationsGonzalo Leonidas Rojas DelgadoNo ratings yet
- Krupp 2007Document7 pagesKrupp 2007Linda CoronadoNo ratings yet
- Comparison Between Kinesitherapy, Magnetic Field and Their Combination For Cerebral Motor Disorders in Early ChildhoodDocument8 pagesComparison Between Kinesitherapy, Magnetic Field and Their Combination For Cerebral Motor Disorders in Early ChildhoodIJAR JOURNALNo ratings yet
- Schizophrenia Research: Xavier Benarous, Marie Raf Fin, Vladimir Ferra Fiat, Angèle Consoli, David CohenDocument12 pagesSchizophrenia Research: Xavier Benarous, Marie Raf Fin, Vladimir Ferra Fiat, Angèle Consoli, David CohenJorge SalazarNo ratings yet
- Dowd 2017 Basal GangliaDocument9 pagesDowd 2017 Basal Gangliasingle_ladyNo ratings yet
- Plasmaferesis en PediatriaDocument6 pagesPlasmaferesis en PediatriaOskr MezaNo ratings yet
- Prevalence and Distribution of MRI Abnormalities in Patients With Psychogenic Nonepileptic EventsDocument4 pagesPrevalence and Distribution of MRI Abnormalities in Patients With Psychogenic Nonepileptic EventsCecilia FRNo ratings yet
- Management of Cerebral Palsy: A Literature Review From A Physiatric PerspectiveDocument4 pagesManagement of Cerebral Palsy: A Literature Review From A Physiatric Perspectivefebry firmansyahNo ratings yet
- Brain Glucose Metabolism and Its RelatioDocument4 pagesBrain Glucose Metabolism and Its RelatioSusana Nuñez RipollNo ratings yet
- Neurological Assgfhgfhfgessment 1Document8 pagesNeurological Assgfhgfhfgessment 1Husaifah BaliwanNo ratings yet
- Ketogenic Diet For The Management of Epilepsy AssoDocument5 pagesKetogenic Diet For The Management of Epilepsy AssoAnita0% (1)
- Long-Term Prognosis After Childhood Convulsive Status Epilepticus: A Prospective Cohort StudyDocument9 pagesLong-Term Prognosis After Childhood Convulsive Status Epilepticus: A Prospective Cohort Studynadia pramitha157No ratings yet
- Vagus Nerve Stimulation in The Treatment of Drug Resistant Epilepsy in 29 Children 2016 European Journal of Paediatric NeurologyDocument6 pagesVagus Nerve Stimulation in The Treatment of Drug Resistant Epilepsy in 29 Children 2016 European Journal of Paediatric NeurologyZeptalanNo ratings yet
- Cerebral PalsyDocument14 pagesCerebral PalsyEka SaputraNo ratings yet
- França (2018) Brain StimulationDocument12 pagesFrança (2018) Brain StimulationAna paula CamargoNo ratings yet
- Early, Accurate Diagnosis and Early Intervention in Cerebral PalsyDocument11 pagesEarly, Accurate Diagnosis and Early Intervention in Cerebral PalsyRoberto López MataNo ratings yet
- 18 01 031 20200804Document7 pages18 01 031 20200804christinaceciliaaNo ratings yet
- 00130478-202105000-00013 Improving "Neuro Checks" in Neonatal ICU and PICU Is A Serial Neurologic Assessment in PediatricsDocument3 pages00130478-202105000-00013 Improving "Neuro Checks" in Neonatal ICU and PICU Is A Serial Neurologic Assessment in PediatricsYo MeNo ratings yet
- Surgical Treatment of Pediatric Focal Cortical DysplasiaDocument8 pagesSurgical Treatment of Pediatric Focal Cortical DysplasiaLuís PachecoNo ratings yet
- Mari 2006Document4 pagesMari 2006Nico NicoNo ratings yet
- Seminar: Solomon L Moshé, Emilio Perucca, Philippe Ryvlin, Torbjörn TomsonDocument15 pagesSeminar: Solomon L Moshé, Emilio Perucca, Philippe Ryvlin, Torbjörn TomsonsriworoNo ratings yet
- Coma and Disorders of Consciousness: Scienti Fic Advances and Practical Considerations For CliniciansDocument8 pagesComa and Disorders of Consciousness: Scienti Fic Advances and Practical Considerations For ClinicianspipikafiyaNo ratings yet
- Cerebral Palsy: Causes and Treatment Alternatives, Based On The Evidence Provided by Gait Analysis - Rupcich M, Bravo RDocument2 pagesCerebral Palsy: Causes and Treatment Alternatives, Based On The Evidence Provided by Gait Analysis - Rupcich M, Bravo RRicardo BravoNo ratings yet
- Henry C Skrehot Neuro Stimulation in Focal Epilepsy ADocument10 pagesHenry C Skrehot Neuro Stimulation in Focal Epilepsy AArbey Aponte PuertoNo ratings yet
- Early, Accurate Diagnosis of Cerebral PalsyDocument11 pagesEarly, Accurate Diagnosis of Cerebral PalsyAndrea PederziniNo ratings yet
- 4Document4 pages4Amr Mohamed GalalNo ratings yet
- Neurocysticercosis Masquerading Psychotic Disorder - A Case ReportDocument3 pagesNeurocysticercosis Masquerading Psychotic Disorder - A Case Reportcynthia jodjanaNo ratings yet
- Personal View: Graham Teasdale, Andrew Maas, Fiona Lecky, Geoff Rey Manley, Nino Stocchetti, Gordon MurrayDocument11 pagesPersonal View: Graham Teasdale, Andrew Maas, Fiona Lecky, Geoff Rey Manley, Nino Stocchetti, Gordon MurrayMariana PeredaNo ratings yet
- Untitled 4Document1 pageUntitled 4Giga HasabiNo ratings yet
- NIH Public Access: Cerebral Hemispherectomy: Sensory Scores Before and After Intensive Mobility TrainingDocument11 pagesNIH Public Access: Cerebral Hemispherectomy: Sensory Scores Before and After Intensive Mobility TrainingBimantoro SaputroNo ratings yet
- Franca 2020 AtaxiaDocument6 pagesFranca 2020 AtaxiainervavsNo ratings yet
- 410 4225 PDFDocument5 pages410 4225 PDFmilhimNo ratings yet
- Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy Advances in Diagnosis and TreatmentDocument11 pagesEarly, Accurate Diagnosis and Early Intervention in Cerebral Palsy Advances in Diagnosis and TreatmentMiguel Angel Rodriguez MartinezNo ratings yet
- CTS PDFDocument6 pagesCTS PDFBiola DwikoNo ratings yet
- Effect of Action Observation Therapy inDocument33 pagesEffect of Action Observation Therapy inseroxat2005No ratings yet
- Jurnal 2Document11 pagesJurnal 2ararapiaNo ratings yet
- 2019 Telerehabilitacion Despues de Un Ictus y AfasiaDocument9 pages2019 Telerehabilitacion Despues de Un Ictus y AfasiaAlba Sueiro DominguezNo ratings yet
- Transcranial Direct Current Stimulation Improves CDocument13 pagesTranscranial Direct Current Stimulation Improves CCarolina Robledo CastroNo ratings yet
- 7Document7 pages7Amr Mohamed GalalNo ratings yet
- Safety of Transcranial Magnetic StimulationDocument15 pagesSafety of Transcranial Magnetic StimulationrajvolgaNo ratings yet
- Overview of Cardiac Valvular Disorders - Cardiovascular Disorders - MSD Manual Professional EditionDocument4 pagesOverview of Cardiac Valvular Disorders - Cardiovascular Disorders - MSD Manual Professional EditionNura Eky VNo ratings yet
- Bloom's Taxonomy - WikipediaDocument11 pagesBloom's Taxonomy - WikipediaNura Eky VNo ratings yet
- 1 s2.0 S1877065719301794 MainDocument8 pages1 s2.0 S1877065719301794 MainNura Eky VNo ratings yet
- 3 Mode Exc OADocument7 pages3 Mode Exc OANura Eky VNo ratings yet
- OTAGO On FrailtyDocument5 pagesOTAGO On FrailtyNura Eky VNo ratings yet
- S0003999321002963Document10 pagesS0003999321002963Nura Eky VNo ratings yet
- 1 s2.0 S0531556520305611 MainDocument8 pages1 s2.0 S0531556520305611 MainNura Eky VNo ratings yet
- 1 s2.0 S0003999321001404Document10 pages1 s2.0 S0003999321001404Nura Eky VNo ratings yet
- Effect of Different Types of Exercises On Psychological and Cognitive Features in People With Parkinson's Disease: A Randomized Controlled TrialDocument10 pagesEffect of Different Types of Exercises On Psychological and Cognitive Features in People With Parkinson's Disease: A Randomized Controlled TrialNura Eky VNo ratings yet
- 16646-Article Text-14610-1-10-20070123Document2 pages16646-Article Text-14610-1-10-20070123Nura Eky VNo ratings yet
- Hof Condition For Dynamic StabilityDocument8 pagesHof Condition For Dynamic StabilityNura Eky VNo ratings yet
- Anterior Cruciate Ligament Injury-Who Succeeds WitDocument9 pagesAnterior Cruciate Ligament Injury-Who Succeeds WitNura Eky VNo ratings yet
- Design CPMDocument5 pagesDesign CPMNura Eky VNo ratings yet
- Spleen: - Site of Lymphocyte Proliferation - Immune Surveillance and Response - Cleanses The BloodDocument13 pagesSpleen: - Site of Lymphocyte Proliferation - Immune Surveillance and Response - Cleanses The BloodNura Eky VNo ratings yet
- Polifarmasi and Fall in ElderlyDocument5 pagesPolifarmasi and Fall in ElderlyNura Eky VNo ratings yet
- Pai Patton97PostPrintDocument7 pagesPai Patton97PostPrintNura Eky VNo ratings yet
- Leonard, 2002Document18 pagesLeonard, 2002Nura Eky VNo ratings yet
- CASP RCT Checklist PDF Fillable FormDocument4 pagesCASP RCT Checklist PDF Fillable FormNura Eky VNo ratings yet
- Impact of Covid Patient RecoveryDocument15 pagesImpact of Covid Patient RecoveryNura Eky VNo ratings yet
- 1 s2.0 S0966636212000811 MainDocument5 pages1 s2.0 S0966636212000811 MainNura Eky VNo ratings yet
- Obesity Review MelaninDocument12 pagesObesity Review MelaninNura Eky VNo ratings yet
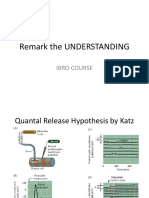
- Remark The UNDERSTANDING: Ibro CourseDocument4 pagesRemark The UNDERSTANDING: Ibro CourseNura Eky VNo ratings yet
- Psychiatry Grand NotesDocument10 pagesPsychiatry Grand NotesNathan T. CheungNo ratings yet
- My Experience With DreamsDocument7 pagesMy Experience With DreamsPamela Rivera SantosNo ratings yet
- Cranial Nerves SummaryDocument6 pagesCranial Nerves SummaryHaider FaqiriNo ratings yet
- Review: Emilio Perucca, Piero Perucca, H Steve White, Elaine C WirrellDocument12 pagesReview: Emilio Perucca, Piero Perucca, H Steve White, Elaine C WirrellFernandoNo ratings yet
- Amino Acids PDFDocument3 pagesAmino Acids PDFJovan StokuchaNo ratings yet
- Physiology Muhammad Ismail 12314Document12 pagesPhysiology Muhammad Ismail 12314Asad SafdarNo ratings yet
- Postpartum BluesDocument17 pagesPostpartum BluesVeliani Putri anggrainiNo ratings yet
- HAMR ManualDocument120 pagesHAMR Manualwarclone100% (3)
- FOUR Score Coma ScaleDocument32 pagesFOUR Score Coma ScaleAndriawan BramNo ratings yet
- Vestibular Function and Anatomy RatnaDocument36 pagesVestibular Function and Anatomy RatnaRatna WindyaningrumNo ratings yet
- MSD ExamDocument4 pagesMSD ExamhELLONo ratings yet
- EssayDocument2 pagesEssayFelipe AndinoNo ratings yet
- Handicap CareDocument18 pagesHandicap CaremuthuuNo ratings yet
- Anesthesia MnemonicsDocument9 pagesAnesthesia MnemonicsLillie Manon100% (1)
- Artificial Neural Network: (Approved by AICTE & Affiliated To UPTU, Lucknow)Document16 pagesArtificial Neural Network: (Approved by AICTE & Affiliated To UPTU, Lucknow)AyushNo ratings yet
- Chapter # 1 Assignment # 1.2: Human Organ Systems Human BrainDocument16 pagesChapter # 1 Assignment # 1.2: Human Organ Systems Human BrainOM PkNo ratings yet
- Notes of CH 7 Control and Coordination - Class 10th Science Study RankersDocument9 pagesNotes of CH 7 Control and Coordination - Class 10th Science Study Rankerssamy0% (1)
- CANSANAYNMDARNEURODocument1 pageCANSANAYNMDARNEUROwarlock ibanezNo ratings yet
- Nervous-System Parctice-TestDocument10 pagesNervous-System Parctice-TestDhon FrondaNo ratings yet
- Brachial Plexus InjuryDocument39 pagesBrachial Plexus InjurymariaNo ratings yet
- Chapter-Six Consumer PerceptionDocument49 pagesChapter-Six Consumer PerceptionGamachu TarikuNo ratings yet
- Hearing Aids PPT FinalDocument26 pagesHearing Aids PPT Finalchristina0% (1)
- Answering Questions Using BiopsychologyDocument4 pagesAnswering Questions Using BiopsychologyAyse KerimNo ratings yet
- The World Through Our SensesDocument14 pagesThe World Through Our SensesamyryuzainiNo ratings yet
- Neurosurgery Syllabus - AustralasiaDocument77 pagesNeurosurgery Syllabus - AustralasiaRaenette DavidNo ratings yet
- 1.1 Sense Organ and Their FunctionDocument20 pages1.1 Sense Organ and Their FunctionReduan Ibrahim100% (3)
- OT Management For CVADocument19 pagesOT Management For CVAMadhurima ChandNo ratings yet
- Assignment in Psychology: Roanne C. LaguaDocument3 pagesAssignment in Psychology: Roanne C. LaguaRoanne LaguaNo ratings yet
- L. Warneke, M.D.: - Progression of Symptoms: Usually TheDocument5 pagesL. Warneke, M.D.: - Progression of Symptoms: Usually TheShradha PatilNo ratings yet