Download as docx, pdf, or txt
You might also like
- 005Document7 pages005Andreea AvasiloaieiNo ratings yet
- Continuing EducationDocument9 pagesContinuing EducationAnitha sujithNo ratings yet
- Epinephrine Versus Dopamine in Neonatal Septic Shock - A Double-Blind PDFDocument8 pagesEpinephrine Versus Dopamine in Neonatal Septic Shock - A Double-Blind PDFCharity TololiuNo ratings yet
- Estado Hemodinamico La Primera Semana de Vida en VLBWDocument7 pagesEstado Hemodinamico La Primera Semana de Vida en VLBWMaluNo ratings yet
- 10 1016@j Jpeds 2020 10 045Document24 pages10 1016@j Jpeds 2020 10 045YasintaUnusNo ratings yet
- Management of Neonatal Hypotension and ShockDocument7 pagesManagement of Neonatal Hypotension and ShockntnquynhproNo ratings yet
- Management of Neonatal Hypotension and ShockDocument7 pagesManagement of Neonatal Hypotension and ShockntnquynhproNo ratings yet
- Variability in The Hemodynamic Response To Fluid Bolus in Pediatric Septic Shock - 1Document11 pagesVariability in The Hemodynamic Response To Fluid Bolus in Pediatric Septic Shock - 1diflopasNo ratings yet
- FP Ago 2020 - Efecto Del Cpap Sobre La Hemodinamia Cerebral en La Hemodinámica Del PrematuroDocument9 pagesFP Ago 2020 - Efecto Del Cpap Sobre La Hemodinamia Cerebral en La Hemodinámica Del Prematurojulius castelloNo ratings yet
- Jnksreenan 2001Document5 pagesJnksreenan 2001fitriNo ratings yet
- 09 2019 Pediatric Neonatology LAYOUT R2Document50 pages09 2019 Pediatric Neonatology LAYOUT R2khalid alharbiNo ratings yet
- The Relationship Between Blood Lactate and Survival Following The Use of Adrenaline in The Treatment of Septic ShockDocument7 pagesThe Relationship Between Blood Lactate and Survival Following The Use of Adrenaline in The Treatment of Septic ShockGoran CucicNo ratings yet
- Infants: Analysis of Systemic Effects and Neonatal Clinical Outcomes Dopamine Versus Epinephrine For Cardiovascular Support in Low Birth WeightDocument12 pagesInfants: Analysis of Systemic Effects and Neonatal Clinical Outcomes Dopamine Versus Epinephrine For Cardiovascular Support in Low Birth WeightJuan Antonio Herrera LealNo ratings yet
- International Journal of Cardiology: Stefano Raffaele Giannubilo, Stefano Cecchi, Elisa Tidu, Andrea CiavattiniDocument3 pagesInternational Journal of Cardiology: Stefano Raffaele Giannubilo, Stefano Cecchi, Elisa Tidu, Andrea CiavattiniFelipe Cortés VegaNo ratings yet
- Animals 11 00685 v3Document12 pagesAnimals 11 00685 v3Carolina Duque RodriguezNo ratings yet
- SEHGAL 2016 - A New Look at Bronchopulmonary Dysplasia - Post Capillary Pathophysiology and Cardiac DysfunctionDocument8 pagesSEHGAL 2016 - A New Look at Bronchopulmonary Dysplasia - Post Capillary Pathophysiology and Cardiac DysfunctionRafael JustinoNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument4 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyFelipe Cortés VegaNo ratings yet
- BMM 2018 0348Document14 pagesBMM 2018 0348Harpreet SinghNo ratings yet
- Ogs 63 293Document12 pagesOgs 63 293DavidNo ratings yet
- Eria 2Document11 pagesEria 2ruth angelinaNo ratings yet
- The Hypertensive NeonateDocument9 pagesThe Hypertensive Neonatelink_wolfloboNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyAlif ZainalNo ratings yet
- Ma 70 408Document5 pagesMa 70 408Zahra AfifahNo ratings yet
- Copeptin in The Differential Diagnosis of Hypotonic PolyuriaDocument10 pagesCopeptin in The Differential Diagnosis of Hypotonic PolyuriacatalinaNo ratings yet
- Medip, IJCP-4171 CSDocument5 pagesMedip, IJCP-4171 CSAarathi raoNo ratings yet
- Co - PeptinDocument5 pagesCo - PeptinBandya SahooNo ratings yet
- 1 s2.0 S1875957218302754 MainDocument8 pages1 s2.0 S1875957218302754 MainanhiramdhaniNo ratings yet
- Hypertension in Infancy: Diagnosis, Management and Outcome: ReviewDocument16 pagesHypertension in Infancy: Diagnosis, Management and Outcome: ReviewJulio César Valdivieso AguirreNo ratings yet
- Machine Learning To Predict Late Respiratory Support in Preterm Infants: A Retrospective Cohort StudyDocument9 pagesMachine Learning To Predict Late Respiratory Support in Preterm Infants: A Retrospective Cohort StudyNodi MNo ratings yet
- Hemodynamic Support in Fluid-Refractory Pediatric Septic ShockDocument6 pagesHemodynamic Support in Fluid-Refractory Pediatric Septic ShockJosé Pepo Apey ReinosoNo ratings yet
- Niknam 2019Document8 pagesNiknam 2019Valdir ReisNo ratings yet
- Clinical StudyDocument6 pagesClinical StudyAndreiMunteanuNo ratings yet
- Prognostic Markers of Neonatal Outcomes in Full Term Neonates Suffering From Perinatal Asphyxia 2167 0897 1000193Document5 pagesPrognostic Markers of Neonatal Outcomes in Full Term Neonates Suffering From Perinatal Asphyxia 2167 0897 1000193Claudia BrînzaNo ratings yet
- Webinar1 Presentation HMforNEXTDocument130 pagesWebinar1 Presentation HMforNEXTAdrian BălanNo ratings yet
- Original ArticleDocument9 pagesOriginal Articlegocelij948No ratings yet
- Urcr DX AsfiksiaDocument3 pagesUrcr DX AsfiksiaChiki CacaNo ratings yet
- Journal Reading - Dopamine Vs EpinephrineDocument51 pagesJournal Reading - Dopamine Vs EpinephrineMoryella MonicaNo ratings yet
- Phphenylephrine Vs EphedrinerineDocument42 pagesPhphenylephrine Vs EphedrinerineDr.Deb Sanjay NagNo ratings yet
- Ma 2018Document1 pageMa 2018Bidhur Chakma 1935371673No ratings yet
- Fetal and Neonatal Effects of N Acetylcysteine When Used - 2016 - The Journal oDocument16 pagesFetal and Neonatal Effects of N Acetylcysteine When Used - 2016 - The Journal oNiluh SukreniNo ratings yet
- Dopamine Vs EpinephrineDocument11 pagesDopamine Vs EpinephrineAyiek WicaksonoNo ratings yet
- Pathophysiology and Treatment Syok Septic in PediatricDocument41 pagesPathophysiology and Treatment Syok Septic in PediatricGustomo PanantroNo ratings yet
- The Use of Sildenafil in Persistent Pulmonary Hypertension of The Newborn PDFDocument6 pagesThe Use of Sildenafil in Persistent Pulmonary Hypertension of The Newborn PDFmaciasdrNo ratings yet
- Evolution of Haemodynamics and Outcome of Fluid Refractory Septic Shock in ChildrenDocument8 pagesEvolution of Haemodynamics and Outcome of Fluid Refractory Septic Shock in ChildrenpetrarizkyNo ratings yet
- Noradrenalina en PrematurosDocument7 pagesNoradrenalina en PrematurosnzunaNo ratings yet
- A Randomized Controlled Trial of Norepinephrine Plus Dobutamine Versus EpinephrineDocument12 pagesA Randomized Controlled Trial of Norepinephrine Plus Dobutamine Versus EpinephrineDokter DewiNo ratings yet
- 2024 PN DG of HTN DingDocument7 pages2024 PN DG of HTN DingАлександра ЛазићNo ratings yet
- Leukemoid Reaction Rare Presentation of Extremely Preterm NeonatesDocument2 pagesLeukemoid Reaction Rare Presentation of Extremely Preterm NeonatesAbdurrahman HasanuddinNo ratings yet
- MainDocument11 pagesMainDhonz R AdiwaramanNo ratings yet
- Progressive Anemia of Prematurity Is Associated With A Critical Increase in Cerebral Oxygen Extraction2020Early Human DevelopmentDocument7 pagesProgressive Anemia of Prematurity Is Associated With A Critical Increase in Cerebral Oxygen Extraction2020Early Human DevelopmentJuan Diego Vilca PinedaNo ratings yet
- Sepsisin ObstetricsDocument9 pagesSepsisin ObstetricsrakulsundaramNo ratings yet
- Journal ReadingDocument5 pagesJournal ReadingRoma WestNo ratings yet
- Pulmonary Arterial Hypertension in Infants With Chronic Lung Disease: Will We Ever Understand It?Document5 pagesPulmonary Arterial Hypertension in Infants With Chronic Lung Disease: Will We Ever Understand It?Adrian KhomanNo ratings yet
- Prednisona Vs ActhDocument7 pagesPrednisona Vs ActhElCanaldeSaadNo ratings yet
- Guideline HypoglycemiaDocument6 pagesGuideline HypoglycemialeslyjanetNo ratings yet
- WRIGHT 2016 - Continuous Positive Airway Pressure To Prevent Neonatal Lung InjuryDocument10 pagesWRIGHT 2016 - Continuous Positive Airway Pressure To Prevent Neonatal Lung InjuryRafael JustinoNo ratings yet
- Jurnal PPHNDocument5 pagesJurnal PPHNJovita OliviaNo ratings yet
- Dose-Related Attenuation of Cardiovascular ResponsDocument7 pagesDose-Related Attenuation of Cardiovascular Responsantoine.dovalNo ratings yet
- Heart Rate Characteristics and Clinical Signs in Neonatal SepsisDocument6 pagesHeart Rate Characteristics and Clinical Signs in Neonatal SepsisDamal An NasherNo ratings yet
- Early Second-Trimester Plasma Levels of Nt-Probnp in Women Who Subsequently Develop Early-Onset PreeclampsiaDocument4 pagesEarly Second-Trimester Plasma Levels of Nt-Probnp in Women Who Subsequently Develop Early-Onset PreeclampsiaLannydchandraNo ratings yet
- Congenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementFrom EverandCongenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementDiva D. De León-CrutchlowNo ratings yet
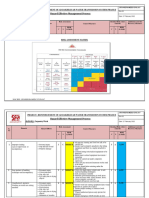
- RISK ASSESSMENT - Carpentry WorkDocument6 pagesRISK ASSESSMENT - Carpentry WorkbalajiNo ratings yet
- Nalco-Tri-Act 2813 MSDSDocument13 pagesNalco-Tri-Act 2813 MSDSSabih UllahNo ratings yet
- Sop For Bio-BurdenDocument5 pagesSop For Bio-BurdenMusyoka Urbanus100% (1)
- Rapport M1-M2Document2 pagesRapport M1-M2LedouxNo ratings yet
- Uncertainity Illness Theory (Merle H.mishel)Document50 pagesUncertainity Illness Theory (Merle H.mishel)Taate Mohammed100% (1)
- Pengaruh Hemolisis Terhadap Nilai Trombosit Dengan Menggunakan Metode Direct CountingDocument6 pagesPengaruh Hemolisis Terhadap Nilai Trombosit Dengan Menggunakan Metode Direct CountingyudhaNo ratings yet
- Migraine & Cluster HeadachesDocument12 pagesMigraine & Cluster HeadachesBigabwa BernardNo ratings yet
- National Insurance Company LimitedDocument6 pagesNational Insurance Company LimitedJeet MaruNo ratings yet
- Patient SatisfactionDocument6 pagesPatient SatisfactionDon Chiaw ManongdoNo ratings yet
- Pharmacy Practice Report SampleDocument26 pagesPharmacy Practice Report Samplesaransh misra67% (3)
- LoadVoucher AspxDocument4 pagesLoadVoucher AspxEdnalyn CasasNo ratings yet
- CV Nicolas Duarte Cifuentes InglesDocument2 pagesCV Nicolas Duarte Cifuentes InglesNicolas Duarte CifuentesNo ratings yet
- Learning Activity Sheet Quarter 2 - MELC 2: Discipline and Ideas in Applied Social SciencesDocument4 pagesLearning Activity Sheet Quarter 2 - MELC 2: Discipline and Ideas in Applied Social Sciencesgayle gallaza100% (1)
- 07 One Missing StrokeDocument10 pages07 One Missing StrokeMiura AngNo ratings yet
- Servant Leadership ReflectionDocument8 pagesServant Leadership Reflectionapi-547372251No ratings yet
- Disaster and Emergency PlanningDocument5 pagesDisaster and Emergency PlanningScarlet GarciaNo ratings yet
- A Definition of CoachingDocument32 pagesA Definition of CoachingSandy KumarNo ratings yet
- Checklist Assessing The Neurological System: S.No Steps YES NODocument9 pagesChecklist Assessing The Neurological System: S.No Steps YES NOpramod kumawat100% (1)
- Chapter 8 Hospital Pharmacy Notes Complete Notes by Noteskarts Acc To ER20Document20 pagesChapter 8 Hospital Pharmacy Notes Complete Notes by Noteskarts Acc To ER20Shamant TNo ratings yet
- Laboratory Errors in The Fabrication of Complete Dentures. A Clinical SurveyDocument5 pagesLaboratory Errors in The Fabrication of Complete Dentures. A Clinical Surveykhaled allaNo ratings yet
- Eni MP Grease 2 - 1720 - 5.0 - ENDocument16 pagesEni MP Grease 2 - 1720 - 5.0 - ENMuhammad Abdul RehmanNo ratings yet
- Primary Health CareDocument17 pagesPrimary Health CareKevins ChepsirNo ratings yet
- Provisional Combined Merit List of Candidates Applied For MDS Courses Under NEET PG 2021Document11 pagesProvisional Combined Merit List of Candidates Applied For MDS Courses Under NEET PG 2021pkv2302No ratings yet
- Unit CostDocument18 pagesUnit CostdoniNo ratings yet
- Zone 2 WorkshopDocument58 pagesZone 2 Workshoprehaangulati2009No ratings yet
- ANCC NCPD ManualDocument58 pagesANCC NCPD Manualshadi alshadafanNo ratings yet
- MKWI4201 Tugas 3Document3 pagesMKWI4201 Tugas 3Kelas B ARS 2018No ratings yet
- Erythrocyte Sedimentation Rate: Westergren MethodDocument20 pagesErythrocyte Sedimentation Rate: Westergren MethodDenise April June CadizNo ratings yet
- Philippine Culture Values and Practices in Relation To Healthcare of Individuals and FamiliesDocument22 pagesPhilippine Culture Values and Practices in Relation To Healthcare of Individuals and FamiliesKhams Tolentino0% (1)