
De Clercq Et Al., 2014
De Clercq Et Al., 2014
You might also like
- MMPX 304 Separation System - System Reference - 1996Document25 pagesMMPX 304 Separation System - System Reference - 1996Centrifugal Separator100% (1)
- NAVFAC Design Procedure 050114 PDFDocument151 pagesNAVFAC Design Procedure 050114 PDFCarl CrowNo ratings yet
- Chess King Manual 201512Document339 pagesChess King Manual 201512Song Jin100% (3)
- Xpediter Training GuideDocument280 pagesXpediter Training GuideJyolsna JyothinadhNo ratings yet
- De Clercq Et Al., 2012Document9 pagesDe Clercq Et Al., 2012Bart De ClercqNo ratings yet
- Yang - Social Support and InflammationDocument12 pagesYang - Social Support and InflammationchrisNo ratings yet
- Adults Perspectives On Cultural, Social and Professional Support in Palliative CareDocument8 pagesAdults Perspectives On Cultural, Social and Professional Support in Palliative CareFatimah FajarNo ratings yet
- Adults Perspectives On Cultural, Social and Professional Support in Palliative CareDocument8 pagesAdults Perspectives On Cultural, Social and Professional Support in Palliative CareFatimah FajarNo ratings yet
- Poscia 2018Document12 pagesPoscia 2018Febria Rike ErlianaNo ratings yet
- Veltkamp 2020Document9 pagesVeltkamp 2020Geanin BurceaNo ratings yet
- J of Family Theo Revie - 2020 - Fuller - The Convoy Model and Later Life Family RelationshipsDocument21 pagesJ of Family Theo Revie - 2020 - Fuller - The Convoy Model and Later Life Family RelationshipsThemby NkovanaNo ratings yet
- 03 Atenção Compartilhada e Referencia SocialDocument20 pages03 Atenção Compartilhada e Referencia SocialBrunna FalgaterNo ratings yet
- McPherson2014 Article TheAssociationBetweenSocialCapDocument16 pagesMcPherson2014 Article TheAssociationBetweenSocialCapMalaika Khan 009No ratings yet
- Wilkinson & Pickett 2017 The Enemy Between Us - Psych & Social Costs of InequalityDocument14 pagesWilkinson & Pickett 2017 The Enemy Between Us - Psych & Social Costs of InequalityXiqiao Katie Chen100% (1)
- Social Networks: Marlène Sapin, Eric D. Widmer, Katia IglesiasDocument14 pagesSocial Networks: Marlène Sapin, Eric D. Widmer, Katia Iglesiasleni vitriaNo ratings yet
- Bowden Green2021Document12 pagesBowden Green2021Makanudo.No ratings yet
- Relationship Between Sense of Community BelongingDocument7 pagesRelationship Between Sense of Community BelongingChloe MintNo ratings yet
- Full Text 01Document39 pagesFull Text 01MA. ANGELICA DE JESUSNo ratings yet
- Community Applied Soc Psy - 2008 - Cicognani - The Impact of Residential Context On Adolescents Subjective Well BeingDocument18 pagesCommunity Applied Soc Psy - 2008 - Cicognani - The Impact of Residential Context On Adolescents Subjective Well Beingregina georgeNo ratings yet
- Facebook As A Source of Social Connectedness in Older AdultsDocument7 pagesFacebook As A Source of Social Connectedness in Older AdultsRewq JoyNo ratings yet
- Why Do People Perceive Themselves As Being Downwardly or Upwardly Mobile?Document21 pagesWhy Do People Perceive Themselves As Being Downwardly or Upwardly Mobile?cutkilerNo ratings yet
- Social Capital 20Document6 pagesSocial Capital 20Adz Jamros Binti JamaliNo ratings yet
- Social Capital and Health: A Review of Prospective Multilevel StudiesDocument9 pagesSocial Capital and Health: A Review of Prospective Multilevel StudiesMónica MartínezNo ratings yet
- "... If There's A Party, Then There's Definitely Alcohol". Construction of Partying Practices and Abstinence in Estonian Youth ForumsDocument16 pages"... If There's A Party, Then There's Definitely Alcohol". Construction of Partying Practices and Abstinence in Estonian Youth ForumsvidhiNo ratings yet
- Hudson Et Al. 2015 Apego y EdadDocument12 pagesHudson Et Al. 2015 Apego y EdadGonzalo Morán MoránNo ratings yet
- INVEST-Working Paper 70 - Social Media Contact With Kin and Happiness in Two GenerationsDocument51 pagesINVEST-Working Paper 70 - Social Media Contact With Kin and Happiness in Two GenerationsIshita SharmaNo ratings yet
- Hota & Batcsh (2019)Document10 pagesHota & Batcsh (2019)YaronNo ratings yet
- Hu Edoc DissertationDocument7 pagesHu Edoc DissertationHelpWithYourPaperCanada100% (1)
- Psyc339 - Term Paper FinalDocument15 pagesPsyc339 - Term Paper FinalAaron BuckleyNo ratings yet
- Beyond The Individual: Evidence Linking Neighborhood Trust and Social Isolation Among Community-Dwelling Older AdultsDocument18 pagesBeyond The Individual: Evidence Linking Neighborhood Trust and Social Isolation Among Community-Dwelling Older AdultsAdriana SerenoNo ratings yet
- Youth PracticalDocument31 pagesYouth PracticalEesha JaiswalNo ratings yet
- 1-s2.0-S235282731830380X-main PAK ARIFINDocument9 pages1-s2.0-S235282731830380X-main PAK ARIFINlettisia anggraNo ratings yet
- Revista de Cercetare (I Interven) Ie Social/: Expert ProjectsDocument21 pagesRevista de Cercetare (I Interven) Ie Social/: Expert ProjectsCristian-Catalin GavatNo ratings yet
- Cai DevpsycholDocument19 pagesCai DevpsycholConsu EloNo ratings yet
- Social Capital at Home Dan School - FullDocument17 pagesSocial Capital at Home Dan School - FullTeguh ImsanNo ratings yet
- Arditti2005EcologicalApproach 2Document11 pagesArditti2005EcologicalApproach 2Sonia DzierzyńskaNo ratings yet
- Governing Emotionally Vulnerable Subjects and Therapisation' of Social JusticeDocument23 pagesGoverning Emotionally Vulnerable Subjects and Therapisation' of Social JusticeCiencia, Salud y Género URJCNo ratings yet
- Micro, Macro, But What About Meso? The Institutional Context of Health InequalitiesDocument2 pagesMicro, Macro, But What About Meso? The Institutional Context of Health InequalitiesRajib DasNo ratings yet
- Internet Ethics of Adolescents-Understanding Demographic DifferencesDocument8 pagesInternet Ethics of Adolescents-Understanding Demographic DifferencestimNo ratings yet
- tmp25FC TMPDocument9 pagestmp25FC TMPFrontiersNo ratings yet
- מימדי הורות- גרוסק ודווידובDocument24 pagesמימדי הורות- גרוסק ודווידובLiron ShalomNo ratings yet
- Velozo J.C.Document5 pagesVelozo J.C.resham agarwalNo ratings yet
- Source of Perceived Social Support and Cognitive Change An 8 Year Prospective Cohort StudyDocument11 pagesSource of Perceived Social Support and Cognitive Change An 8 Year Prospective Cohort StudyTNo ratings yet
- DP 14447Document105 pagesDP 14447Carolina Huarcaya FloresNo ratings yet
- The Role of Socio-Demographics, Family, and Peer Factors in Adolescent Alcohol BehaviorsDocument11 pagesThe Role of Socio-Demographics, Family, and Peer Factors in Adolescent Alcohol BehaviorsIJELS Research JournalNo ratings yet
- Social Participation of School Aged Children Who Use Communication Aids The Views of Children and ParentsDocument16 pagesSocial Participation of School Aged Children Who Use Communication Aids The Views of Children and ParentsericaxiangozNo ratings yet
- SocialjusticetheoryencyclopediaDocument9 pagesSocialjusticetheoryencyclopediaMarian TiongsonNo ratings yet
- Exploring The Potential (LSERO) PDFDocument28 pagesExploring The Potential (LSERO) PDFClaudio PidotoNo ratings yet
- Kroll Social Indicators ResearchDocument22 pagesKroll Social Indicators ResearchAurindra WiieznuNo ratings yet
- Consumption Oriented Engagement in Social Network Sites Undesirable Influence On Personal Well BeingDocument45 pagesConsumption Oriented Engagement in Social Network Sites Undesirable Influence On Personal Well BeingBelhadj TarekNo ratings yet
- Discursive StudiesDocument11 pagesDiscursive StudiesSohag LTCNo ratings yet
- Adolescent Pornography Consumption: A Symbolic Interactionist LensDocument16 pagesAdolescent Pornography Consumption: A Symbolic Interactionist LensAndrea A. Ortiz VázquezNo ratings yet
- EK313 - U18 - Carpenter and McConkeyDocument11 pagesEK313 - U18 - Carpenter and McConkeyfreya.k.tinneyNo ratings yet
- A Social Justice Perspective On The Delivery of Family Support. ResearchDocument8 pagesA Social Justice Perspective On The Delivery of Family Support. ResearchRominaNo ratings yet
- Impact of Perceived Social Support On Psychological Wellbeing in Young AdultsDocument7 pagesImpact of Perceived Social Support On Psychological Wellbeing in Young AdultsIJRASETPublicationsNo ratings yet
- Constructing The Meaning of Family, Care Leaver PaperDocument10 pagesConstructing The Meaning of Family, Care Leaver PaperGee GeeNo ratings yet
- Huang, Edwards, Laurel-Wilson - 2020 - The Shadow of Context Neighborhood and School Socioeconomic Disadvantage, Perceived Social IntegrDocument12 pagesHuang, Edwards, Laurel-Wilson - 2020 - The Shadow of Context Neighborhood and School Socioeconomic Disadvantage, Perceived Social IntegrCarolina Macaya AranedaNo ratings yet
- Ethical ConsiderationsDocument15 pagesEthical ConsiderationsANA DelafuenteNo ratings yet
- Ifedayo Alatise Annotated Bibliography PPN201.Document8 pagesIfedayo Alatise Annotated Bibliography PPN201.diekola ridwanNo ratings yet
- Rottger Rossler 2020Document21 pagesRottger Rossler 2020PolarisNo ratings yet
- Class Contingencies in Networks of Care For School-Aged ChildrenDocument57 pagesClass Contingencies in Networks of Care For School-Aged ChildrenvsudhakarvNo ratings yet
- The Convoy Model: Explaining Social Relations From A Multidisciplinary PerspectiveDocument11 pagesThe Convoy Model: Explaining Social Relations From A Multidisciplinary PerspectiveAna Gutiérrez MartínezNo ratings yet
- Project Resilience: Preparing Youth To Respond To AdversityDocument7 pagesProject Resilience: Preparing Youth To Respond To AdversityinventionjournalsNo ratings yet
- Practitioner's Guide to Empirically Based Measures of Social SkillsFrom EverandPractitioner's Guide to Empirically Based Measures of Social SkillsNo ratings yet
- Research Papers On Primary Education in PakistanDocument4 pagesResearch Papers On Primary Education in Pakistanfvgh9ept100% (1)
- FM136 Mighty Mule Wireless Intercom PDFDocument8 pagesFM136 Mighty Mule Wireless Intercom PDFalanbrannNo ratings yet
- Case 521e Tier3 - enDocument846 pagesCase 521e Tier3 - enRUBEN RINCONNo ratings yet
- The Evacuation and Charge ProcessDocument3 pagesThe Evacuation and Charge ProcessRyan RobbinsNo ratings yet
- Newte Bag Palletizing 2Document4 pagesNewte Bag Palletizing 2Kien Nguyen TrungNo ratings yet
- Nebosh How To Pass Your Open Book Exam On The First AttemptDocument4 pagesNebosh How To Pass Your Open Book Exam On The First Attemptdp.cavozziNo ratings yet
- 10 04 060 SPCDocument1 page10 04 060 SPCMichael Ben-DorNo ratings yet
- 3102213-En FW-UL6W FireWorks Workstation Installation ManualDocument62 pages3102213-En FW-UL6W FireWorks Workstation Installation ManualTrung Thành VõNo ratings yet
- Patumahoe Hill Community Mound - Summit With A View - ForeverDocument32 pagesPatumahoe Hill Community Mound - Summit With A View - ForeverPatumahoeVillageIncNo ratings yet
- Exemple Dissertation Philo BonheurDocument7 pagesExemple Dissertation Philo BonheurPayToWriteAPaperMinneapolis100% (1)
- Elison HR J Chem Educ 2005 82 1086Document3 pagesElison HR J Chem Educ 2005 82 1086Daniel ButlerNo ratings yet
- 120140084-10 InglesDocument2 pages120140084-10 InglesMelany Lopez50% (4)
- Business Mathematics and Statistics Asim Kumar Manna Full ChapterDocument67 pagesBusiness Mathematics and Statistics Asim Kumar Manna Full Chaptergoldie.brooks294100% (6)
- ATA 20 Standard Practices PDFDocument6 pagesATA 20 Standard Practices PDFRicky100% (1)
- Ansi C84-1Document11 pagesAnsi C84-1Rosa Edith Rada Alprecht0% (2)
- Design of Experiments: Instructor: Engr. Ambreen TajammalDocument77 pagesDesign of Experiments: Instructor: Engr. Ambreen TajammalAmbreen TajammalNo ratings yet
- Unit - Ii Software Engineering ProcessDocument39 pagesUnit - Ii Software Engineering ProcessrlkfjnsdlkNo ratings yet
- F24 60manual (New)Document14 pagesF24 60manual (New)Robert CumpaNo ratings yet
- Etabs For ResidentioalDocument6 pagesEtabs For ResidentioalIsmailNo ratings yet
- Liew Huay Ling, Lim Siew Yee and Helmer Aslaksen Department of Mathematics, National University of Singapore Semester 2, 2000/2001Document4 pagesLiew Huay Ling, Lim Siew Yee and Helmer Aslaksen Department of Mathematics, National University of Singapore Semester 2, 2000/20011940LaSalleNo ratings yet
- Folleto Drone PDFDocument2 pagesFolleto Drone PDFBrizard CondoriNo ratings yet
- Upaya Hukum Terhadap Pelanggaran Implementasi (Iot) Di Bidang Pelayanan Kesehatan Menurut Ketentuan Perlindungan Data PribadiDocument17 pagesUpaya Hukum Terhadap Pelanggaran Implementasi (Iot) Di Bidang Pelayanan Kesehatan Menurut Ketentuan Perlindungan Data PribadiValentina AdindaNo ratings yet
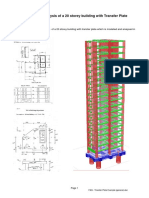
- FAQ - Transfer Plate Example (General) PDFDocument6 pagesFAQ - Transfer Plate Example (General) PDFStevenNo ratings yet
- 5 Elements Chinese Palmistry - #2 PDFDocument8 pages5 Elements Chinese Palmistry - #2 PDFAlison_VicarNo ratings yet
- SHIZUKI Capacitors and ReactorsDocument6 pagesSHIZUKI Capacitors and ReactorsUrsula JohnsonNo ratings yet
- Mohammad Ali CVDocument8 pagesMohammad Ali CVMohammad Ali100% (1)
























































































Download as pdf or txt
You might also like
- MMPX 304 Separation System - System Reference - 1996Document25 pagesMMPX 304 Separation System - System Reference - 1996Centrifugal Separator100% (1)
- NAVFAC Design Procedure 050114 PDFDocument151 pagesNAVFAC Design Procedure 050114 PDFCarl CrowNo ratings yet
- Chess King Manual 201512Document339 pagesChess King Manual 201512Song Jin100% (3)
- Xpediter Training GuideDocument280 pagesXpediter Training GuideJyolsna JyothinadhNo ratings yet
- De Clercq Et Al., 2012Document9 pagesDe Clercq Et Al., 2012Bart De ClercqNo ratings yet
- Yang - Social Support and InflammationDocument12 pagesYang - Social Support and InflammationchrisNo ratings yet
- Adults Perspectives On Cultural, Social and Professional Support in Palliative CareDocument8 pagesAdults Perspectives On Cultural, Social and Professional Support in Palliative CareFatimah FajarNo ratings yet
- Adults Perspectives On Cultural, Social and Professional Support in Palliative CareDocument8 pagesAdults Perspectives On Cultural, Social and Professional Support in Palliative CareFatimah FajarNo ratings yet
- Poscia 2018Document12 pagesPoscia 2018Febria Rike ErlianaNo ratings yet
- Veltkamp 2020Document9 pagesVeltkamp 2020Geanin BurceaNo ratings yet
- J of Family Theo Revie - 2020 - Fuller - The Convoy Model and Later Life Family RelationshipsDocument21 pagesJ of Family Theo Revie - 2020 - Fuller - The Convoy Model and Later Life Family RelationshipsThemby NkovanaNo ratings yet
- 03 Atenção Compartilhada e Referencia SocialDocument20 pages03 Atenção Compartilhada e Referencia SocialBrunna FalgaterNo ratings yet
- McPherson2014 Article TheAssociationBetweenSocialCapDocument16 pagesMcPherson2014 Article TheAssociationBetweenSocialCapMalaika Khan 009No ratings yet
- Wilkinson & Pickett 2017 The Enemy Between Us - Psych & Social Costs of InequalityDocument14 pagesWilkinson & Pickett 2017 The Enemy Between Us - Psych & Social Costs of InequalityXiqiao Katie Chen100% (1)
- Social Networks: Marlène Sapin, Eric D. Widmer, Katia IglesiasDocument14 pagesSocial Networks: Marlène Sapin, Eric D. Widmer, Katia Iglesiasleni vitriaNo ratings yet
- Bowden Green2021Document12 pagesBowden Green2021Makanudo.No ratings yet
- Relationship Between Sense of Community BelongingDocument7 pagesRelationship Between Sense of Community BelongingChloe MintNo ratings yet
- Full Text 01Document39 pagesFull Text 01MA. ANGELICA DE JESUSNo ratings yet
- Community Applied Soc Psy - 2008 - Cicognani - The Impact of Residential Context On Adolescents Subjective Well BeingDocument18 pagesCommunity Applied Soc Psy - 2008 - Cicognani - The Impact of Residential Context On Adolescents Subjective Well Beingregina georgeNo ratings yet
- Facebook As A Source of Social Connectedness in Older AdultsDocument7 pagesFacebook As A Source of Social Connectedness in Older AdultsRewq JoyNo ratings yet
- Why Do People Perceive Themselves As Being Downwardly or Upwardly Mobile?Document21 pagesWhy Do People Perceive Themselves As Being Downwardly or Upwardly Mobile?cutkilerNo ratings yet
- Social Capital 20Document6 pagesSocial Capital 20Adz Jamros Binti JamaliNo ratings yet
- Social Capital and Health: A Review of Prospective Multilevel StudiesDocument9 pagesSocial Capital and Health: A Review of Prospective Multilevel StudiesMónica MartínezNo ratings yet
- "... If There's A Party, Then There's Definitely Alcohol". Construction of Partying Practices and Abstinence in Estonian Youth ForumsDocument16 pages"... If There's A Party, Then There's Definitely Alcohol". Construction of Partying Practices and Abstinence in Estonian Youth ForumsvidhiNo ratings yet
- Hudson Et Al. 2015 Apego y EdadDocument12 pagesHudson Et Al. 2015 Apego y EdadGonzalo Morán MoránNo ratings yet
- INVEST-Working Paper 70 - Social Media Contact With Kin and Happiness in Two GenerationsDocument51 pagesINVEST-Working Paper 70 - Social Media Contact With Kin and Happiness in Two GenerationsIshita SharmaNo ratings yet
- Hota & Batcsh (2019)Document10 pagesHota & Batcsh (2019)YaronNo ratings yet
- Hu Edoc DissertationDocument7 pagesHu Edoc DissertationHelpWithYourPaperCanada100% (1)
- Psyc339 - Term Paper FinalDocument15 pagesPsyc339 - Term Paper FinalAaron BuckleyNo ratings yet
- Beyond The Individual: Evidence Linking Neighborhood Trust and Social Isolation Among Community-Dwelling Older AdultsDocument18 pagesBeyond The Individual: Evidence Linking Neighborhood Trust and Social Isolation Among Community-Dwelling Older AdultsAdriana SerenoNo ratings yet
- Youth PracticalDocument31 pagesYouth PracticalEesha JaiswalNo ratings yet
- 1-s2.0-S235282731830380X-main PAK ARIFINDocument9 pages1-s2.0-S235282731830380X-main PAK ARIFINlettisia anggraNo ratings yet
- Revista de Cercetare (I Interven) Ie Social/: Expert ProjectsDocument21 pagesRevista de Cercetare (I Interven) Ie Social/: Expert ProjectsCristian-Catalin GavatNo ratings yet
- Cai DevpsycholDocument19 pagesCai DevpsycholConsu EloNo ratings yet
- Social Capital at Home Dan School - FullDocument17 pagesSocial Capital at Home Dan School - FullTeguh ImsanNo ratings yet
- Arditti2005EcologicalApproach 2Document11 pagesArditti2005EcologicalApproach 2Sonia DzierzyńskaNo ratings yet
- Governing Emotionally Vulnerable Subjects and Therapisation' of Social JusticeDocument23 pagesGoverning Emotionally Vulnerable Subjects and Therapisation' of Social JusticeCiencia, Salud y Género URJCNo ratings yet
- Micro, Macro, But What About Meso? The Institutional Context of Health InequalitiesDocument2 pagesMicro, Macro, But What About Meso? The Institutional Context of Health InequalitiesRajib DasNo ratings yet
- Internet Ethics of Adolescents-Understanding Demographic DifferencesDocument8 pagesInternet Ethics of Adolescents-Understanding Demographic DifferencestimNo ratings yet
- tmp25FC TMPDocument9 pagestmp25FC TMPFrontiersNo ratings yet
- מימדי הורות- גרוסק ודווידובDocument24 pagesמימדי הורות- גרוסק ודווידובLiron ShalomNo ratings yet
- Velozo J.C.Document5 pagesVelozo J.C.resham agarwalNo ratings yet
- Source of Perceived Social Support and Cognitive Change An 8 Year Prospective Cohort StudyDocument11 pagesSource of Perceived Social Support and Cognitive Change An 8 Year Prospective Cohort StudyTNo ratings yet
- DP 14447Document105 pagesDP 14447Carolina Huarcaya FloresNo ratings yet
- The Role of Socio-Demographics, Family, and Peer Factors in Adolescent Alcohol BehaviorsDocument11 pagesThe Role of Socio-Demographics, Family, and Peer Factors in Adolescent Alcohol BehaviorsIJELS Research JournalNo ratings yet
- Social Participation of School Aged Children Who Use Communication Aids The Views of Children and ParentsDocument16 pagesSocial Participation of School Aged Children Who Use Communication Aids The Views of Children and ParentsericaxiangozNo ratings yet
- SocialjusticetheoryencyclopediaDocument9 pagesSocialjusticetheoryencyclopediaMarian TiongsonNo ratings yet
- Exploring The Potential (LSERO) PDFDocument28 pagesExploring The Potential (LSERO) PDFClaudio PidotoNo ratings yet
- Kroll Social Indicators ResearchDocument22 pagesKroll Social Indicators ResearchAurindra WiieznuNo ratings yet
- Consumption Oriented Engagement in Social Network Sites Undesirable Influence On Personal Well BeingDocument45 pagesConsumption Oriented Engagement in Social Network Sites Undesirable Influence On Personal Well BeingBelhadj TarekNo ratings yet
- Discursive StudiesDocument11 pagesDiscursive StudiesSohag LTCNo ratings yet
- Adolescent Pornography Consumption: A Symbolic Interactionist LensDocument16 pagesAdolescent Pornography Consumption: A Symbolic Interactionist LensAndrea A. Ortiz VázquezNo ratings yet
- EK313 - U18 - Carpenter and McConkeyDocument11 pagesEK313 - U18 - Carpenter and McConkeyfreya.k.tinneyNo ratings yet
- A Social Justice Perspective On The Delivery of Family Support. ResearchDocument8 pagesA Social Justice Perspective On The Delivery of Family Support. ResearchRominaNo ratings yet
- Impact of Perceived Social Support On Psychological Wellbeing in Young AdultsDocument7 pagesImpact of Perceived Social Support On Psychological Wellbeing in Young AdultsIJRASETPublicationsNo ratings yet
- Constructing The Meaning of Family, Care Leaver PaperDocument10 pagesConstructing The Meaning of Family, Care Leaver PaperGee GeeNo ratings yet
- Huang, Edwards, Laurel-Wilson - 2020 - The Shadow of Context Neighborhood and School Socioeconomic Disadvantage, Perceived Social IntegrDocument12 pagesHuang, Edwards, Laurel-Wilson - 2020 - The Shadow of Context Neighborhood and School Socioeconomic Disadvantage, Perceived Social IntegrCarolina Macaya AranedaNo ratings yet
- Ethical ConsiderationsDocument15 pagesEthical ConsiderationsANA DelafuenteNo ratings yet
- Ifedayo Alatise Annotated Bibliography PPN201.Document8 pagesIfedayo Alatise Annotated Bibliography PPN201.diekola ridwanNo ratings yet
- Rottger Rossler 2020Document21 pagesRottger Rossler 2020PolarisNo ratings yet
- Class Contingencies in Networks of Care For School-Aged ChildrenDocument57 pagesClass Contingencies in Networks of Care For School-Aged ChildrenvsudhakarvNo ratings yet
- The Convoy Model: Explaining Social Relations From A Multidisciplinary PerspectiveDocument11 pagesThe Convoy Model: Explaining Social Relations From A Multidisciplinary PerspectiveAna Gutiérrez MartínezNo ratings yet
- Project Resilience: Preparing Youth To Respond To AdversityDocument7 pagesProject Resilience: Preparing Youth To Respond To AdversityinventionjournalsNo ratings yet
- Practitioner's Guide to Empirically Based Measures of Social SkillsFrom EverandPractitioner's Guide to Empirically Based Measures of Social SkillsNo ratings yet
- Research Papers On Primary Education in PakistanDocument4 pagesResearch Papers On Primary Education in Pakistanfvgh9ept100% (1)
- FM136 Mighty Mule Wireless Intercom PDFDocument8 pagesFM136 Mighty Mule Wireless Intercom PDFalanbrannNo ratings yet
- Case 521e Tier3 - enDocument846 pagesCase 521e Tier3 - enRUBEN RINCONNo ratings yet
- The Evacuation and Charge ProcessDocument3 pagesThe Evacuation and Charge ProcessRyan RobbinsNo ratings yet
- Newte Bag Palletizing 2Document4 pagesNewte Bag Palletizing 2Kien Nguyen TrungNo ratings yet
- Nebosh How To Pass Your Open Book Exam On The First AttemptDocument4 pagesNebosh How To Pass Your Open Book Exam On The First Attemptdp.cavozziNo ratings yet
- 10 04 060 SPCDocument1 page10 04 060 SPCMichael Ben-DorNo ratings yet
- 3102213-En FW-UL6W FireWorks Workstation Installation ManualDocument62 pages3102213-En FW-UL6W FireWorks Workstation Installation ManualTrung Thành VõNo ratings yet
- Patumahoe Hill Community Mound - Summit With A View - ForeverDocument32 pagesPatumahoe Hill Community Mound - Summit With A View - ForeverPatumahoeVillageIncNo ratings yet
- Exemple Dissertation Philo BonheurDocument7 pagesExemple Dissertation Philo BonheurPayToWriteAPaperMinneapolis100% (1)
- Elison HR J Chem Educ 2005 82 1086Document3 pagesElison HR J Chem Educ 2005 82 1086Daniel ButlerNo ratings yet
- 120140084-10 InglesDocument2 pages120140084-10 InglesMelany Lopez50% (4)
- Business Mathematics and Statistics Asim Kumar Manna Full ChapterDocument67 pagesBusiness Mathematics and Statistics Asim Kumar Manna Full Chaptergoldie.brooks294100% (6)
- ATA 20 Standard Practices PDFDocument6 pagesATA 20 Standard Practices PDFRicky100% (1)
- Ansi C84-1Document11 pagesAnsi C84-1Rosa Edith Rada Alprecht0% (2)
- Design of Experiments: Instructor: Engr. Ambreen TajammalDocument77 pagesDesign of Experiments: Instructor: Engr. Ambreen TajammalAmbreen TajammalNo ratings yet
- Unit - Ii Software Engineering ProcessDocument39 pagesUnit - Ii Software Engineering ProcessrlkfjnsdlkNo ratings yet
- F24 60manual (New)Document14 pagesF24 60manual (New)Robert CumpaNo ratings yet
- Etabs For ResidentioalDocument6 pagesEtabs For ResidentioalIsmailNo ratings yet
- Liew Huay Ling, Lim Siew Yee and Helmer Aslaksen Department of Mathematics, National University of Singapore Semester 2, 2000/2001Document4 pagesLiew Huay Ling, Lim Siew Yee and Helmer Aslaksen Department of Mathematics, National University of Singapore Semester 2, 2000/20011940LaSalleNo ratings yet
- Folleto Drone PDFDocument2 pagesFolleto Drone PDFBrizard CondoriNo ratings yet
- Upaya Hukum Terhadap Pelanggaran Implementasi (Iot) Di Bidang Pelayanan Kesehatan Menurut Ketentuan Perlindungan Data PribadiDocument17 pagesUpaya Hukum Terhadap Pelanggaran Implementasi (Iot) Di Bidang Pelayanan Kesehatan Menurut Ketentuan Perlindungan Data PribadiValentina AdindaNo ratings yet
- FAQ - Transfer Plate Example (General) PDFDocument6 pagesFAQ - Transfer Plate Example (General) PDFStevenNo ratings yet
- 5 Elements Chinese Palmistry - #2 PDFDocument8 pages5 Elements Chinese Palmistry - #2 PDFAlison_VicarNo ratings yet
- SHIZUKI Capacitors and ReactorsDocument6 pagesSHIZUKI Capacitors and ReactorsUrsula JohnsonNo ratings yet
- Mohammad Ali CVDocument8 pagesMohammad Ali CVMohammad Ali100% (1)