
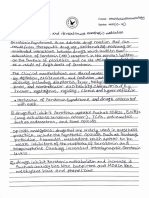
A Nerve Transfer Is A Surgical Operation in Which A Surgeon Reroutes A Healthy
A Nerve Transfer Is A Surgical Operation in Which A Surgeon Reroutes A Healthy
You might also like
- MAITLAND MOBILIZATION - FinalDocument35 pagesMAITLAND MOBILIZATION - FinalBhagawati Pooja94% (17)
- An Introduction To TattvasDocument13 pagesAn Introduction To TattvasTemple of the stars83% (6)
- Dns PDFDocument22 pagesDns PDFOtrovanje100% (1)
- PNF InserviceDocument25 pagesPNF Inserviceapi-518034073No ratings yet
- VCE Project Report FinalDocument17 pagesVCE Project Report FinalPuneet Singh Dhani25% (4)
- Use Cases For Example ATM SystemDocument54 pagesUse Cases For Example ATM SystemGayatri SharmaNo ratings yet
- Therapeutic Exercise 1 IntroductionDocument30 pagesTherapeutic Exercise 1 IntroductionMyrgen TingsonNo ratings yet
- Bobath Approach: Concepts and PrinciplesDocument30 pagesBobath Approach: Concepts and PrinciplesJulia SalvioNo ratings yet
- TTD Special Entry Darshan ReceiptDocument2 pagesTTD Special Entry Darshan Receiptmaheshwara100% (2)
- Proprioceptive Neuromuscular Facilitation (PNF) : BY: Fraymond Mayunga PhysiotherapistDocument50 pagesProprioceptive Neuromuscular Facilitation (PNF) : BY: Fraymond Mayunga PhysiotherapistallytubishaNo ratings yet
- Arthroscopic Shoulder Anterior Stabilisation Rehabilitation Protocol by TENDAYI MUTSOPOTSI MSc. ORTHO-MEDDocument8 pagesArthroscopic Shoulder Anterior Stabilisation Rehabilitation Protocol by TENDAYI MUTSOPOTSI MSc. ORTHO-MEDPhysiotherapy Care SpecialistsNo ratings yet
- Spinal StabilizationDocument32 pagesSpinal StabilizationLakshita PrajapatiNo ratings yet
- "Neuro Rehabilitation": Presented byDocument52 pages"Neuro Rehabilitation": Presented byArchana VermaNo ratings yet
- Theories of Neurological RehabilitationDocument30 pagesTheories of Neurological Rehabilitationabdul haseebNo ratings yet
- Tendon Transfers - RehabilitationDocument4 pagesTendon Transfers - RehabilitationPankaj Malik100% (4)
- Therapeutic ExercisesDocument50 pagesTherapeutic ExercisesBalram Jha100% (3)
- Role of Physio in Neurological Disorders.Document17 pagesRole of Physio in Neurological Disorders.Maheen AnwaarNo ratings yet
- PHK 28575Document9 pagesPHK 28575Cornel BazeliucNo ratings yet
- Sensory Motor Approaches: Asma KhalidDocument31 pagesSensory Motor Approaches: Asma KhalidAsaad Jawed100% (1)
- Exercise Therapy For Physical Therapist: Naruemon LeelayuwatDocument20 pagesExercise Therapy For Physical Therapist: Naruemon LeelayuwatAron NavarroNo ratings yet
- Physiotherapy Rehabilitation Guidelines - Lumbar DisectomyDocument6 pagesPhysiotherapy Rehabilitation Guidelines - Lumbar Disectomyalina4891No ratings yet
- Physiotherapy and Mental Health: Michel ProbstDocument22 pagesPhysiotherapy and Mental Health: Michel ProbstAntónioAbraçosNo ratings yet
- Stretching 4Document30 pagesStretching 4MahiNo ratings yet
- Lec9 Basic Concepts of Spinal Management With ExerciseDocument21 pagesLec9 Basic Concepts of Spinal Management With Exercisesana mumtazNo ratings yet
- Lecture 15 Manual RX ExerciseDocument9 pagesLecture 15 Manual RX ExerciseMarwa MehmoodNo ratings yet
- Progressive Systematic Functional Rehabilitation: Ameema, Hina, IfraDocument33 pagesProgressive Systematic Functional Rehabilitation: Ameema, Hina, Ifrakashmala afzalNo ratings yet
- Excercise TherapyDocument30 pagesExcercise TherapyAbdi Asiis Omar MohamedNo ratings yet
- PT To Prevent Pressure SoresDocument25 pagesPT To Prevent Pressure SoresSelvi SoundararajanNo ratings yet
- Introduction To PNF For StrokeDocument91 pagesIntroduction To PNF For StrokeImran Tarmizi100% (1)
- A Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategies For Frozen ShoulderDocument4 pagesA Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategies For Frozen ShoulderSergiNo ratings yet
- Passive Movements - KinesiologyDocument18 pagesPassive Movements - KinesiologyKanwal Khan50% (2)
- Power PointDocument33 pagesPower PointSougato PandaNo ratings yet
- Foundational Concepts - Part 1Document26 pagesFoundational Concepts - Part 1Neo Derrick Adrian MartinezNo ratings yet
- Li Satri Materi Bing - IIIDocument9 pagesLi Satri Materi Bing - IIILi SatryNo ratings yet
- Muhammed Kocabiyik Physical Medicine & Rehabilitation Iv. Class V. GroupDocument14 pagesMuhammed Kocabiyik Physical Medicine & Rehabilitation Iv. Class V. GroupsanalcrazyNo ratings yet
- Posture and Factor Affecting Posture in Physical TherapyDocument28 pagesPosture and Factor Affecting Posture in Physical TherapyAnand Vaghasiya100% (2)
- Pelvic TractionDocument2 pagesPelvic TractionGabbii CincoNo ratings yet
- World Physical Therapy DayDocument18 pagesWorld Physical Therapy DaySu AlexNo ratings yet
- Application of Bobath COnceptDocument61 pagesApplication of Bobath COnceptArun Kumar PTNo ratings yet
- Low Back Pain: Amir ShuhairiDocument69 pagesLow Back Pain: Amir ShuhairiHikaru99 otakuNo ratings yet
- Lectur 1 Kinesiology 2 DPT-2Document56 pagesLectur 1 Kinesiology 2 DPT-2Syeda Abida Hussain SheraziNo ratings yet
- Lectur 1 Kinesiology 2 DPT-1Document52 pagesLectur 1 Kinesiology 2 DPT-1Syeda Abida Hussain SheraziNo ratings yet
- M1 Introduction To Manual TherapyDocument101 pagesM1 Introduction To Manual TherapySylvia LoongNo ratings yet
- Evolution of Neurodevelopmental Therapy (NDT)Document59 pagesEvolution of Neurodevelopmental Therapy (NDT)Aashish ShankarNo ratings yet
- Ox Ach Exere-Prescripn-slides SuppletDocument40 pagesOx Ach Exere-Prescripn-slides SuppletБаровић ЛукаNo ratings yet
- Bobath ApproachDocument25 pagesBobath ApproachAkshay BadoreNo ratings yet
- Rehabilitation in Spinal Cord InjuryDocument2 pagesRehabilitation in Spinal Cord InjuryAudry ArifinNo ratings yet
- Neurorestorasi Untuk Pasien Stroke Fase Post Akut (Pendekatan Konsep PNF)Document43 pagesNeurorestorasi Untuk Pasien Stroke Fase Post Akut (Pendekatan Konsep PNF)lizadwijanuaryanaNo ratings yet
- Referat Limba Engleză-Zidaroiu Ionuț-EduardDocument6 pagesReferat Limba Engleză-Zidaroiu Ionuț-EduardEduard IonutNo ratings yet
- Brachial Plexus 1Document15 pagesBrachial Plexus 1Einstein JeromeNo ratings yet
- Rehabilitasi Post Op Spine Surgery: Kobal Sangaji Dokter Spesialis Rehabilitasi Medik RS Awalbros PekanbaruDocument27 pagesRehabilitasi Post Op Spine Surgery: Kobal Sangaji Dokter Spesialis Rehabilitasi Medik RS Awalbros PekanbarukurniaNo ratings yet
- Propriocepti VE Neuromuscu LAR FaciclitationDocument37 pagesPropriocepti VE Neuromuscu LAR FaciclitationPriya YadavNo ratings yet
- Physiotherapy Rehabilitation Guidelines - Lumbar Disectomy PDFDocument6 pagesPhysiotherapy Rehabilitation Guidelines - Lumbar Disectomy PDFsilkofosNo ratings yet
- MODULE 1 - THXDocument13 pagesMODULE 1 - THXZgama AbdulrahmanNo ratings yet
- Rehab-Plans-and-Exercises Hip-Arthroscopy Protocol-For-Physiotherapy-Following-SurgeryDocument2 pagesRehab-Plans-and-Exercises Hip-Arthroscopy Protocol-For-Physiotherapy-Following-SurgeryMellow Moon RecordsNo ratings yet
- Fundamental Principles IIDocument12 pagesFundamental Principles IIHunter KeroNo ratings yet
- Treatment ApproachesDocument16 pagesTreatment ApproachesSheron MathewNo ratings yet
- 2 - Eclectic Approach For Stroke ManagementDocument41 pages2 - Eclectic Approach For Stroke Managementpunit lakraNo ratings yet
- Approaches To Therapeutic Exercise and Activity For NeurologicalDocument69 pagesApproaches To Therapeutic Exercise and Activity For NeurologicalPedro M. BorgesNo ratings yet
- CH 1 - PT 1Document60 pagesCH 1 - PT 1noureenNo ratings yet
- Proprioceptive Neuromuscular FacilitationDocument38 pagesProprioceptive Neuromuscular FacilitationNolanNo ratings yet
- Neuroo 170210095341 PDFDocument162 pagesNeuroo 170210095341 PDFmalathiNo ratings yet
- 8-Proprioceptive Neuromuscular FacilitationDocument15 pages8-Proprioceptive Neuromuscular FacilitationSham David PTNo ratings yet
- Reflexology: The Definitive Practitioner's Manual: Recommended by the International Therapy Examination Council for Students and PractitonersFrom EverandReflexology: The Definitive Practitioner's Manual: Recommended by the International Therapy Examination Council for Students and PractitonersRating: 5 out of 5 stars5/5 (6)
- UniversityDocument30 pagesUniversityAya AmerNo ratings yet
- UniversityDocument15 pagesUniversityAya AmerNo ratings yet
- Differentiate Between Fascial and Bell's PalsyDocument19 pagesDifferentiate Between Fascial and Bell's PalsyAya AmerNo ratings yet
- Tracheal Tug - Paradoxical Chest MovementDocument7 pagesTracheal Tug - Paradoxical Chest MovementAya AmerNo ratings yet
- Biochemical and Cellular Mechanisms of Toxic Liver Injury: Neil Kaplowitz, M.DDocument8 pagesBiochemical and Cellular Mechanisms of Toxic Liver Injury: Neil Kaplowitz, M.DAya AmerNo ratings yet
- Skin Manifestations of Common DiseasesDocument5 pagesSkin Manifestations of Common DiseasesAya AmerNo ratings yet
- Comparative and Superlative - TalaDocument3 pagesComparative and Superlative - TalaAya AmerNo ratings yet
- IntroductionDocument4 pagesIntroductionAya AmerNo ratings yet
- Seortonin Syndrome Alaa AmerDocument3 pagesSeortonin Syndrome Alaa AmerAya AmerNo ratings yet
- The Passive - Past Continuous 2 (Transformations)Document2 pagesThe Passive - Past Continuous 2 (Transformations)Aya AmerNo ratings yet
- Chapter 8 Muscular Analysis of Upper Extremity ExercisesDocument20 pagesChapter 8 Muscular Analysis of Upper Extremity ExercisesAya AmerNo ratings yet
- Nonselective Adrenergic β Blocking AgentsDocument1 pageNonselective Adrenergic β Blocking AgentsAya AmerNo ratings yet
- Beta1-Selective Adrenergic Blocking AgentsDocument1 pageBeta1-Selective Adrenergic Blocking AgentsAya AmerNo ratings yet
- Advance Assessment and DiagnosisDocument3 pagesAdvance Assessment and DiagnosisAya AmerNo ratings yet
- Nonselective Adrenergic β Blocking AgentsDocument1 pageNonselective Adrenergic β Blocking AgentsAya AmerNo ratings yet
- History Taking Physical ExamininationDocument41 pagesHistory Taking Physical ExamininationAya AmerNo ratings yet
- Case StudyDocument6 pagesCase StudyAya AmerNo ratings yet
- Indirect Cholinergic - agonists-gLradp-YrplMjq-83987Document1 pageIndirect Cholinergic - agonists-gLradp-YrplMjq-83987Aya AmerNo ratings yet
- Directacting - Cholinergic - Agonists Faxrh3 lYVFRoQ 74189Document1 pageDirectacting - Cholinergic - Agonists Faxrh3 lYVFRoQ 74189Aya AmerNo ratings yet
- Logic ChartDocument1 pageLogic ChartAya AmerNo ratings yet
- Nonselective adrenergic β blocking agentsDocument1 pageNonselective adrenergic β blocking agentsAya AmerNo ratings yet
- Directacting - Cholinergic - Agonists YZFDaR tSaqZ1a 62028Document1 pageDirectacting - Cholinergic - Agonists YZFDaR tSaqZ1a 62028Aya AmerNo ratings yet
- Asimakopulos, A. (1975) - A Kaleckian Theory of Income Distribution. Canadian Journal of Economics, 313-333.Document22 pagesAsimakopulos, A. (1975) - A Kaleckian Theory of Income Distribution. Canadian Journal of Economics, 313-333.lcr89No ratings yet
- Case Study On Akshaya Patra Group-1Document9 pagesCase Study On Akshaya Patra Group-1swaroopNo ratings yet
- Steel Material Table PDFDocument1 pageSteel Material Table PDFNathanNo ratings yet
- Thesis Ethical HackingDocument6 pagesThesis Ethical Hackingshannonsandbillings100% (2)
- Vedic Astrolgy Paet - 4Document64 pagesVedic Astrolgy Paet - 4krumiaaNo ratings yet
- © The Institute of Chartered Accountants of IndiaDocument154 pages© The Institute of Chartered Accountants of IndiaJattu TatiNo ratings yet
- Asme B31.3Document2 pagesAsme B31.3Juan ortega castellarNo ratings yet
- How To Make A MicheladaDocument2 pagesHow To Make A MicheladaJulio Quiroz PalaciosNo ratings yet
- Test Initial EnglezaDocument4 pagesTest Initial EnglezaPop CameliaNo ratings yet
- Touch FootballDocument75 pagesTouch FootballIon Balda MarinNo ratings yet
- Fuschi Et Al 2022 Microplastics in The Great Lakes Environmental Health and Socioeconomic Implications and FutureDocument18 pagesFuschi Et Al 2022 Microplastics in The Great Lakes Environmental Health and Socioeconomic Implications and FuturecriscazanNo ratings yet
- History MiagaoDocument9 pagesHistory MiagaoZONETTE PAREDONo ratings yet
- Sansulin R Suspensi Injeksi 100 IU, ML - Rekombinan Insulin Manusia - DKI0708100443A1 - 2016Document2 pagesSansulin R Suspensi Injeksi 100 IU, ML - Rekombinan Insulin Manusia - DKI0708100443A1 - 2016Yessi VirginiaNo ratings yet
- CESTARO - Plan-Tonificacion Inicial MujerDocument14 pagesCESTARO - Plan-Tonificacion Inicial MujerLucas Javier VidalNo ratings yet
- EQG-How To Generate User License in S4 HANA Using SAP Audit Measurement Program (USMM) v2.00Document9 pagesEQG-How To Generate User License in S4 HANA Using SAP Audit Measurement Program (USMM) v2.00tanudyNo ratings yet
- OpAudCh02 CBET 01 501E ToraldeMa - KristineE.Document4 pagesOpAudCh02 CBET 01 501E ToraldeMa - KristineE.Kristine Esplana ToraldeNo ratings yet
- Europe & ThailandDocument1 pageEurope & ThailandTipitaka TripitakaNo ratings yet
- Ifgtb List Lds Mts 03feb15Document11 pagesIfgtb List Lds Mts 03feb15kaifiahmedNo ratings yet
- Luxury DIY Sulfate Shampoo - Workbook - VFDocument14 pagesLuxury DIY Sulfate Shampoo - Workbook - VFralucaxjsNo ratings yet
- Addmrpt 1 36558 36559Document7 pagesAddmrpt 1 36558 36559Anonymous ZGcs7MwsLNo ratings yet
- Tinker Bell Secret of The Wings Junior No - Disney Book GroupDocument81 pagesTinker Bell Secret of The Wings Junior No - Disney Book GroupXuan Mai Nguyen ThiNo ratings yet
- ChancroidDocument4 pagesChancroidDaniel Vergara ArceNo ratings yet
- 03-737-800 Ramp & Transit Electrical PowerDocument92 pages03-737-800 Ramp & Transit Electrical PowerNicolas Sal100% (2)
- Math Solo Plan NewDocument15 pagesMath Solo Plan NewMicah David SmithNo ratings yet
- Inflationary Gap - WikipediaDocument15 pagesInflationary Gap - WikipediaKush KumarNo ratings yet
- David Staral ComplaintDocument24 pagesDavid Staral Complaintdannyecker_crainNo ratings yet











































































































Download as docx, pdf, or txt
You might also like
- MAITLAND MOBILIZATION - FinalDocument35 pagesMAITLAND MOBILIZATION - FinalBhagawati Pooja94% (17)
- An Introduction To TattvasDocument13 pagesAn Introduction To TattvasTemple of the stars83% (6)
- Dns PDFDocument22 pagesDns PDFOtrovanje100% (1)
- PNF InserviceDocument25 pagesPNF Inserviceapi-518034073No ratings yet
- VCE Project Report FinalDocument17 pagesVCE Project Report FinalPuneet Singh Dhani25% (4)
- Use Cases For Example ATM SystemDocument54 pagesUse Cases For Example ATM SystemGayatri SharmaNo ratings yet
- Therapeutic Exercise 1 IntroductionDocument30 pagesTherapeutic Exercise 1 IntroductionMyrgen TingsonNo ratings yet
- Bobath Approach: Concepts and PrinciplesDocument30 pagesBobath Approach: Concepts and PrinciplesJulia SalvioNo ratings yet
- TTD Special Entry Darshan ReceiptDocument2 pagesTTD Special Entry Darshan Receiptmaheshwara100% (2)
- Proprioceptive Neuromuscular Facilitation (PNF) : BY: Fraymond Mayunga PhysiotherapistDocument50 pagesProprioceptive Neuromuscular Facilitation (PNF) : BY: Fraymond Mayunga PhysiotherapistallytubishaNo ratings yet
- Arthroscopic Shoulder Anterior Stabilisation Rehabilitation Protocol by TENDAYI MUTSOPOTSI MSc. ORTHO-MEDDocument8 pagesArthroscopic Shoulder Anterior Stabilisation Rehabilitation Protocol by TENDAYI MUTSOPOTSI MSc. ORTHO-MEDPhysiotherapy Care SpecialistsNo ratings yet
- Spinal StabilizationDocument32 pagesSpinal StabilizationLakshita PrajapatiNo ratings yet
- "Neuro Rehabilitation": Presented byDocument52 pages"Neuro Rehabilitation": Presented byArchana VermaNo ratings yet
- Theories of Neurological RehabilitationDocument30 pagesTheories of Neurological Rehabilitationabdul haseebNo ratings yet
- Tendon Transfers - RehabilitationDocument4 pagesTendon Transfers - RehabilitationPankaj Malik100% (4)
- Therapeutic ExercisesDocument50 pagesTherapeutic ExercisesBalram Jha100% (3)
- Role of Physio in Neurological Disorders.Document17 pagesRole of Physio in Neurological Disorders.Maheen AnwaarNo ratings yet
- PHK 28575Document9 pagesPHK 28575Cornel BazeliucNo ratings yet
- Sensory Motor Approaches: Asma KhalidDocument31 pagesSensory Motor Approaches: Asma KhalidAsaad Jawed100% (1)
- Exercise Therapy For Physical Therapist: Naruemon LeelayuwatDocument20 pagesExercise Therapy For Physical Therapist: Naruemon LeelayuwatAron NavarroNo ratings yet
- Physiotherapy Rehabilitation Guidelines - Lumbar DisectomyDocument6 pagesPhysiotherapy Rehabilitation Guidelines - Lumbar Disectomyalina4891No ratings yet
- Physiotherapy and Mental Health: Michel ProbstDocument22 pagesPhysiotherapy and Mental Health: Michel ProbstAntónioAbraçosNo ratings yet
- Stretching 4Document30 pagesStretching 4MahiNo ratings yet
- Lec9 Basic Concepts of Spinal Management With ExerciseDocument21 pagesLec9 Basic Concepts of Spinal Management With Exercisesana mumtazNo ratings yet
- Lecture 15 Manual RX ExerciseDocument9 pagesLecture 15 Manual RX ExerciseMarwa MehmoodNo ratings yet
- Progressive Systematic Functional Rehabilitation: Ameema, Hina, IfraDocument33 pagesProgressive Systematic Functional Rehabilitation: Ameema, Hina, Ifrakashmala afzalNo ratings yet
- Excercise TherapyDocument30 pagesExcercise TherapyAbdi Asiis Omar MohamedNo ratings yet
- PT To Prevent Pressure SoresDocument25 pagesPT To Prevent Pressure SoresSelvi SoundararajanNo ratings yet
- Introduction To PNF For StrokeDocument91 pagesIntroduction To PNF For StrokeImran Tarmizi100% (1)
- A Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategies For Frozen ShoulderDocument4 pagesA Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategies For Frozen ShoulderSergiNo ratings yet
- Passive Movements - KinesiologyDocument18 pagesPassive Movements - KinesiologyKanwal Khan50% (2)
- Power PointDocument33 pagesPower PointSougato PandaNo ratings yet
- Foundational Concepts - Part 1Document26 pagesFoundational Concepts - Part 1Neo Derrick Adrian MartinezNo ratings yet
- Li Satri Materi Bing - IIIDocument9 pagesLi Satri Materi Bing - IIILi SatryNo ratings yet
- Muhammed Kocabiyik Physical Medicine & Rehabilitation Iv. Class V. GroupDocument14 pagesMuhammed Kocabiyik Physical Medicine & Rehabilitation Iv. Class V. GroupsanalcrazyNo ratings yet
- Posture and Factor Affecting Posture in Physical TherapyDocument28 pagesPosture and Factor Affecting Posture in Physical TherapyAnand Vaghasiya100% (2)
- Pelvic TractionDocument2 pagesPelvic TractionGabbii CincoNo ratings yet
- World Physical Therapy DayDocument18 pagesWorld Physical Therapy DaySu AlexNo ratings yet
- Application of Bobath COnceptDocument61 pagesApplication of Bobath COnceptArun Kumar PTNo ratings yet
- Low Back Pain: Amir ShuhairiDocument69 pagesLow Back Pain: Amir ShuhairiHikaru99 otakuNo ratings yet
- Lectur 1 Kinesiology 2 DPT-2Document56 pagesLectur 1 Kinesiology 2 DPT-2Syeda Abida Hussain SheraziNo ratings yet
- Lectur 1 Kinesiology 2 DPT-1Document52 pagesLectur 1 Kinesiology 2 DPT-1Syeda Abida Hussain SheraziNo ratings yet
- M1 Introduction To Manual TherapyDocument101 pagesM1 Introduction To Manual TherapySylvia LoongNo ratings yet
- Evolution of Neurodevelopmental Therapy (NDT)Document59 pagesEvolution of Neurodevelopmental Therapy (NDT)Aashish ShankarNo ratings yet
- Ox Ach Exere-Prescripn-slides SuppletDocument40 pagesOx Ach Exere-Prescripn-slides SuppletБаровић ЛукаNo ratings yet
- Bobath ApproachDocument25 pagesBobath ApproachAkshay BadoreNo ratings yet
- Rehabilitation in Spinal Cord InjuryDocument2 pagesRehabilitation in Spinal Cord InjuryAudry ArifinNo ratings yet
- Neurorestorasi Untuk Pasien Stroke Fase Post Akut (Pendekatan Konsep PNF)Document43 pagesNeurorestorasi Untuk Pasien Stroke Fase Post Akut (Pendekatan Konsep PNF)lizadwijanuaryanaNo ratings yet
- Referat Limba Engleză-Zidaroiu Ionuț-EduardDocument6 pagesReferat Limba Engleză-Zidaroiu Ionuț-EduardEduard IonutNo ratings yet
- Brachial Plexus 1Document15 pagesBrachial Plexus 1Einstein JeromeNo ratings yet
- Rehabilitasi Post Op Spine Surgery: Kobal Sangaji Dokter Spesialis Rehabilitasi Medik RS Awalbros PekanbaruDocument27 pagesRehabilitasi Post Op Spine Surgery: Kobal Sangaji Dokter Spesialis Rehabilitasi Medik RS Awalbros PekanbarukurniaNo ratings yet
- Propriocepti VE Neuromuscu LAR FaciclitationDocument37 pagesPropriocepti VE Neuromuscu LAR FaciclitationPriya YadavNo ratings yet
- Physiotherapy Rehabilitation Guidelines - Lumbar Disectomy PDFDocument6 pagesPhysiotherapy Rehabilitation Guidelines - Lumbar Disectomy PDFsilkofosNo ratings yet
- MODULE 1 - THXDocument13 pagesMODULE 1 - THXZgama AbdulrahmanNo ratings yet
- Rehab-Plans-and-Exercises Hip-Arthroscopy Protocol-For-Physiotherapy-Following-SurgeryDocument2 pagesRehab-Plans-and-Exercises Hip-Arthroscopy Protocol-For-Physiotherapy-Following-SurgeryMellow Moon RecordsNo ratings yet
- Fundamental Principles IIDocument12 pagesFundamental Principles IIHunter KeroNo ratings yet
- Treatment ApproachesDocument16 pagesTreatment ApproachesSheron MathewNo ratings yet
- 2 - Eclectic Approach For Stroke ManagementDocument41 pages2 - Eclectic Approach For Stroke Managementpunit lakraNo ratings yet
- Approaches To Therapeutic Exercise and Activity For NeurologicalDocument69 pagesApproaches To Therapeutic Exercise and Activity For NeurologicalPedro M. BorgesNo ratings yet
- CH 1 - PT 1Document60 pagesCH 1 - PT 1noureenNo ratings yet
- Proprioceptive Neuromuscular FacilitationDocument38 pagesProprioceptive Neuromuscular FacilitationNolanNo ratings yet
- Neuroo 170210095341 PDFDocument162 pagesNeuroo 170210095341 PDFmalathiNo ratings yet
- 8-Proprioceptive Neuromuscular FacilitationDocument15 pages8-Proprioceptive Neuromuscular FacilitationSham David PTNo ratings yet
- Reflexology: The Definitive Practitioner's Manual: Recommended by the International Therapy Examination Council for Students and PractitonersFrom EverandReflexology: The Definitive Practitioner's Manual: Recommended by the International Therapy Examination Council for Students and PractitonersRating: 5 out of 5 stars5/5 (6)
- UniversityDocument30 pagesUniversityAya AmerNo ratings yet
- UniversityDocument15 pagesUniversityAya AmerNo ratings yet
- Differentiate Between Fascial and Bell's PalsyDocument19 pagesDifferentiate Between Fascial and Bell's PalsyAya AmerNo ratings yet
- Tracheal Tug - Paradoxical Chest MovementDocument7 pagesTracheal Tug - Paradoxical Chest MovementAya AmerNo ratings yet
- Biochemical and Cellular Mechanisms of Toxic Liver Injury: Neil Kaplowitz, M.DDocument8 pagesBiochemical and Cellular Mechanisms of Toxic Liver Injury: Neil Kaplowitz, M.DAya AmerNo ratings yet
- Skin Manifestations of Common DiseasesDocument5 pagesSkin Manifestations of Common DiseasesAya AmerNo ratings yet
- Comparative and Superlative - TalaDocument3 pagesComparative and Superlative - TalaAya AmerNo ratings yet
- IntroductionDocument4 pagesIntroductionAya AmerNo ratings yet
- Seortonin Syndrome Alaa AmerDocument3 pagesSeortonin Syndrome Alaa AmerAya AmerNo ratings yet
- The Passive - Past Continuous 2 (Transformations)Document2 pagesThe Passive - Past Continuous 2 (Transformations)Aya AmerNo ratings yet
- Chapter 8 Muscular Analysis of Upper Extremity ExercisesDocument20 pagesChapter 8 Muscular Analysis of Upper Extremity ExercisesAya AmerNo ratings yet
- Nonselective Adrenergic β Blocking AgentsDocument1 pageNonselective Adrenergic β Blocking AgentsAya AmerNo ratings yet
- Beta1-Selective Adrenergic Blocking AgentsDocument1 pageBeta1-Selective Adrenergic Blocking AgentsAya AmerNo ratings yet
- Advance Assessment and DiagnosisDocument3 pagesAdvance Assessment and DiagnosisAya AmerNo ratings yet
- Nonselective Adrenergic β Blocking AgentsDocument1 pageNonselective Adrenergic β Blocking AgentsAya AmerNo ratings yet
- History Taking Physical ExamininationDocument41 pagesHistory Taking Physical ExamininationAya AmerNo ratings yet
- Case StudyDocument6 pagesCase StudyAya AmerNo ratings yet
- Indirect Cholinergic - agonists-gLradp-YrplMjq-83987Document1 pageIndirect Cholinergic - agonists-gLradp-YrplMjq-83987Aya AmerNo ratings yet
- Directacting - Cholinergic - Agonists Faxrh3 lYVFRoQ 74189Document1 pageDirectacting - Cholinergic - Agonists Faxrh3 lYVFRoQ 74189Aya AmerNo ratings yet
- Logic ChartDocument1 pageLogic ChartAya AmerNo ratings yet
- Nonselective adrenergic β blocking agentsDocument1 pageNonselective adrenergic β blocking agentsAya AmerNo ratings yet
- Directacting - Cholinergic - Agonists YZFDaR tSaqZ1a 62028Document1 pageDirectacting - Cholinergic - Agonists YZFDaR tSaqZ1a 62028Aya AmerNo ratings yet
- Asimakopulos, A. (1975) - A Kaleckian Theory of Income Distribution. Canadian Journal of Economics, 313-333.Document22 pagesAsimakopulos, A. (1975) - A Kaleckian Theory of Income Distribution. Canadian Journal of Economics, 313-333.lcr89No ratings yet
- Case Study On Akshaya Patra Group-1Document9 pagesCase Study On Akshaya Patra Group-1swaroopNo ratings yet
- Steel Material Table PDFDocument1 pageSteel Material Table PDFNathanNo ratings yet
- Thesis Ethical HackingDocument6 pagesThesis Ethical Hackingshannonsandbillings100% (2)
- Vedic Astrolgy Paet - 4Document64 pagesVedic Astrolgy Paet - 4krumiaaNo ratings yet
- © The Institute of Chartered Accountants of IndiaDocument154 pages© The Institute of Chartered Accountants of IndiaJattu TatiNo ratings yet
- Asme B31.3Document2 pagesAsme B31.3Juan ortega castellarNo ratings yet
- How To Make A MicheladaDocument2 pagesHow To Make A MicheladaJulio Quiroz PalaciosNo ratings yet
- Test Initial EnglezaDocument4 pagesTest Initial EnglezaPop CameliaNo ratings yet
- Touch FootballDocument75 pagesTouch FootballIon Balda MarinNo ratings yet
- Fuschi Et Al 2022 Microplastics in The Great Lakes Environmental Health and Socioeconomic Implications and FutureDocument18 pagesFuschi Et Al 2022 Microplastics in The Great Lakes Environmental Health and Socioeconomic Implications and FuturecriscazanNo ratings yet
- History MiagaoDocument9 pagesHistory MiagaoZONETTE PAREDONo ratings yet
- Sansulin R Suspensi Injeksi 100 IU, ML - Rekombinan Insulin Manusia - DKI0708100443A1 - 2016Document2 pagesSansulin R Suspensi Injeksi 100 IU, ML - Rekombinan Insulin Manusia - DKI0708100443A1 - 2016Yessi VirginiaNo ratings yet
- CESTARO - Plan-Tonificacion Inicial MujerDocument14 pagesCESTARO - Plan-Tonificacion Inicial MujerLucas Javier VidalNo ratings yet
- EQG-How To Generate User License in S4 HANA Using SAP Audit Measurement Program (USMM) v2.00Document9 pagesEQG-How To Generate User License in S4 HANA Using SAP Audit Measurement Program (USMM) v2.00tanudyNo ratings yet
- OpAudCh02 CBET 01 501E ToraldeMa - KristineE.Document4 pagesOpAudCh02 CBET 01 501E ToraldeMa - KristineE.Kristine Esplana ToraldeNo ratings yet
- Europe & ThailandDocument1 pageEurope & ThailandTipitaka TripitakaNo ratings yet
- Ifgtb List Lds Mts 03feb15Document11 pagesIfgtb List Lds Mts 03feb15kaifiahmedNo ratings yet
- Luxury DIY Sulfate Shampoo - Workbook - VFDocument14 pagesLuxury DIY Sulfate Shampoo - Workbook - VFralucaxjsNo ratings yet
- Addmrpt 1 36558 36559Document7 pagesAddmrpt 1 36558 36559Anonymous ZGcs7MwsLNo ratings yet
- Tinker Bell Secret of The Wings Junior No - Disney Book GroupDocument81 pagesTinker Bell Secret of The Wings Junior No - Disney Book GroupXuan Mai Nguyen ThiNo ratings yet
- ChancroidDocument4 pagesChancroidDaniel Vergara ArceNo ratings yet
- 03-737-800 Ramp & Transit Electrical PowerDocument92 pages03-737-800 Ramp & Transit Electrical PowerNicolas Sal100% (2)
- Math Solo Plan NewDocument15 pagesMath Solo Plan NewMicah David SmithNo ratings yet
- Inflationary Gap - WikipediaDocument15 pagesInflationary Gap - WikipediaKush KumarNo ratings yet
- David Staral ComplaintDocument24 pagesDavid Staral Complaintdannyecker_crainNo ratings yet