Download as pdf or txt
You might also like
- Paediatric Assessment FormDocument4 pagesPaediatric Assessment Formdrrajmptn84% (32)
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsFrom EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsNo ratings yet
- AXA PPP Claim Form PDFDocument2 pagesAXA PPP Claim Form PDFEleftheria AggeleaNo ratings yet
- MD India Insurance Claim FormDocument5 pagesMD India Insurance Claim FormYogesh ParchaniNo ratings yet
- Claim Form Dd2642Document4 pagesClaim Form Dd2642Adina BusteaNo ratings yet
- Bupa Global Claim Form: 1 Patient'S DetailsDocument4 pagesBupa Global Claim Form: 1 Patient'S Details123owenNo ratings yet
- Training System For Enhancing Athletic Performance Al VermeilDocument165 pagesTraining System For Enhancing Athletic Performance Al Vermeilxaviermay100% (7)
- Robinhood Work PackDocument12 pagesRobinhood Work PackxaviermayNo ratings yet
- Mnemonics For Clinical ExamDocument20 pagesMnemonics For Clinical ExamDrAmeen1976100% (3)
- Health: Quarter 1-Module 6Document25 pagesHealth: Quarter 1-Module 6Niko Igie Albino Pujeda0% (1)
- CLAIM FORM Maternity MEAF RSA 69041 3Document5 pagesCLAIM FORM Maternity MEAF RSA 69041 3Arindam ChangdarNo ratings yet
- Claim Intimation Form Insurance 0Document2 pagesClaim Intimation Form Insurance 0Vishal SankheNo ratings yet
- GMHP Claim Form - Online PDFDocument4 pagesGMHP Claim Form - Online PDFSalem AmraneNo ratings yet
- Department of State Academic Exchanges Participant Medical History and Examination FormDocument8 pagesDepartment of State Academic Exchanges Participant Medical History and Examination FormNurman HidayatNo ratings yet
- OVHC Claim Form 102017 PDFDocument3 pagesOVHC Claim Form 102017 PDFtarmudiNo ratings yet
- Application For Membership Form: Application No.: Effectivity Date: Contract No.Document2 pagesApplication For Membership Form: Application No.: Effectivity Date: Contract No.Lizeth QuerubinNo ratings yet
- Reg 2-Primary Care Claim Form-31 Oct 2008Document2 pagesReg 2-Primary Care Claim Form-31 Oct 2008Pradeep KhubchandaniNo ratings yet
- SG Worldcare Pre AuthorisationDocument3 pagesSG Worldcare Pre Authorisationbernardlim86No ratings yet
- Claim FormDocument4 pagesClaim FormRohit UtrejaNo ratings yet
- AXA Non Death Claim FormDocument4 pagesAXA Non Death Claim FormKenji ChinNo ratings yet
- BIN Claim Form 1611v11 D PDFDocument5 pagesBIN Claim Form 1611v11 D PDFAnonymous BZF0QIjDNo ratings yet
- ReimbursementDocument2 pagesReimbursementFAZILNo ratings yet
- OMA OM en Claims TravelDelayDocument4 pagesOMA OM en Claims TravelDelayreshwan aliNo ratings yet
- COVID RTW Form (CAN)Document3 pagesCOVID RTW Form (CAN)A. MuyepaNo ratings yet
- Appeal/Exception Request FormDocument2 pagesAppeal/Exception Request FormimranbagdadiNo ratings yet
- Mumbai Claim FormDocument5 pagesMumbai Claim FormsunsangraNo ratings yet
- Phil Health ClaimForm GuidelinesDocument7 pagesPhil Health ClaimForm GuidelinesFerdinand CordovizNo ratings yet
- Certification Vaccination EmployeesDocument2 pagesCertification Vaccination EmployeesMediafax.roNo ratings yet
- Claim Form en Nov 08Document4 pagesClaim Form en Nov 08Juju FernsNo ratings yet
- Important:: CIGNA Group InsuranceDocument2 pagesImportant:: CIGNA Group InsuranceLoganBohannonNo ratings yet
- Form BUPADocument4 pagesForm BUPAterusunduhNo ratings yet
- FB Pregnancy-ComplicationDocument19 pagesFB Pregnancy-ComplicationHihiNo ratings yet
- Medical ReleaseDocument2 pagesMedical ReleasekhangpngNo ratings yet
- Reporting Your Disability Claim: When Do I Report A Claim?Document1 pageReporting Your Disability Claim: When Do I Report A Claim?jfreakerNo ratings yet
- Prescription Reimb Claim FormDocument2 pagesPrescription Reimb Claim FormimthedciNo ratings yet
- Mail Order Form Formed CoDocument2 pagesMail Order Form Formed CoKiran CheriyanNo ratings yet
- Ahmedabad Claim FormDocument5 pagesAhmedabad Claim FormFirdaus PanthakyNo ratings yet
- Gulfcare Insurancec Claim FormDocument1 pageGulfcare Insurancec Claim FormrishijaveriNo ratings yet
- Claim Form: Patient's Details - To Be Completed by The Person Undergoing TreatmentDocument4 pagesClaim Form: Patient's Details - To Be Completed by The Person Undergoing Treatmentpier_roNo ratings yet
- Claim Form-MD IndiaDocument5 pagesClaim Form-MD IndiaMusycal FynncNo ratings yet
- 1 Claim FormDocument36 pages1 Claim Formkarmayukh1No ratings yet
- Mymedicare Registration FormDocument2 pagesMymedicare Registration Formbonnakoy72No ratings yet
- BINS Bupa Global Claim Form en 2005 21089Document8 pagesBINS Bupa Global Claim Form en 2005 21089R.Pearlsis SophiNo ratings yet
- BUPA Intl Claim Form PDFDocument4 pagesBUPA Intl Claim Form PDFisabellashNo ratings yet
- NAS - Reimbursement Claim FormDocument2 pagesNAS - Reimbursement Claim FormPIANGO40% (5)
- Bupa International Claim Form: 1 Patient'S DetailsDocument4 pagesBupa International Claim Form: 1 Patient'S DetailsRealty SolutionsNo ratings yet
- Student Application FormDocument6 pagesStudent Application FormelletjiesNo ratings yet
- Health Benefits Claim Form: InstructionsDocument1 pageHealth Benefits Claim Form: InstructionsAdrianaBujorNo ratings yet
- Alberta Accident Benefits Initial Claims Process: AB-1 (2006/01) Page 1 of 5Document5 pagesAlberta Accident Benefits Initial Claims Process: AB-1 (2006/01) Page 1 of 5Patrick Maguire100% (1)
- Medical Claim Reimbursement Form EnglishDocument2 pagesMedical Claim Reimbursement Form EnglishHananAhmedNo ratings yet
- Med 1Document4 pagesMed 1api-259279833No ratings yet
- Claim Form: 1 Patient's DetailsDocument7 pagesClaim Form: 1 Patient's DetailsEduskill Learning CentreNo ratings yet
- BAH Bupa Global Claim Form EN APR21 0027975Document8 pagesBAH Bupa Global Claim Form EN APR21 0027975ALJABERNo ratings yet
- Bupa Global Claim FormDocument8 pagesBupa Global Claim FormALJABERNo ratings yet
- FMS 094194 PDFDocument10 pagesFMS 094194 PDFAnonymous nGq8TsV4uANo ratings yet
- NOW HEALTH Claim - Form - Uae - RsaDocument2 pagesNOW HEALTH Claim - Form - Uae - RsaWilliam IsaacNo ratings yet
- L Aetna-Disabled-Dep-Physician-FormDocument7 pagesL Aetna-Disabled-Dep-Physician-Formssromani19No ratings yet
- Fulbright Certificate of HealthDocument8 pagesFulbright Certificate of HealthLinda Klimavicius100% (1)
- Pparx ApplicationsDocument8 pagesPparx ApplicationsJames MullinsNo ratings yet
- PackageDocument2 pagesPackageScott StewartNo ratings yet
- Medical Certificates and Reports GP ObligationsDocument12 pagesMedical Certificates and Reports GP ObligationsgovindaNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- A Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsFrom EverandA Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsNo ratings yet
- Newman's Billing and Coding Technicians Study GuideFrom EverandNewman's Billing and Coding Technicians Study GuideRating: 4.5 out of 5 stars4.5/5 (2)
- 1 LumbarFunctionDocument18 pages1 LumbarFunctionxaviermayNo ratings yet
- Anabolic Steroid Guide Part 2 PDFDocument134 pagesAnabolic Steroid Guide Part 2 PDFxaviermayNo ratings yet
- Dominate Your Anatomy - Delts PDFDocument33 pagesDominate Your Anatomy - Delts PDFxaviermayNo ratings yet
- Job Description: Post Title Bja: Department: Reports To: Direct Reports: Role Grade: Location: Key RelationshipsDocument3 pagesJob Description: Post Title Bja: Department: Reports To: Direct Reports: Role Grade: Location: Key RelationshipsxaviermayNo ratings yet
- O C C U P A T I o N S M A T C H I N G e X e R C I S e W o R K S H e e TDocument2 pagesO C C U P A T I o N S M A T C H I N G e X e R C I S e W o R K S H e e TxaviermayNo ratings yet
- Whats My JobDocument2 pagesWhats My JobxaviermayNo ratings yet
- Shoulder Rehab: Renovating The "House" From The Inside OutDocument3 pagesShoulder Rehab: Renovating The "House" From The Inside OutxaviermayNo ratings yet
- Modern JudoDocument151 pagesModern Judobaffledexpert100% (2)
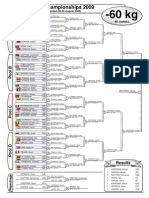
- World Championships 2009Document14 pagesWorld Championships 2009xaviermayNo ratings yet
- ListeriosisDocument11 pagesListeriosisDrChauhanNo ratings yet
- DR - JD - Gemelli - Fetal DemiseDocument14 pagesDR - JD - Gemelli - Fetal DemiseAulia Rizqi MulyaniNo ratings yet
- OB Ozamiz GroupDocument26 pagesOB Ozamiz GroupJb RosillosaNo ratings yet
- BayesDocument9 pagesBayesSiddhesh ParabNo ratings yet
- Obstetrics MnemonicsDocument9 pagesObstetrics MnemonicsJared Khoo Er Hau100% (2)
- DM No. 2023 0083 Guidelines For The FHSIS Data Validation and Reconciliation - 22feb2023 2Document11 pagesDM No. 2023 0083 Guidelines For The FHSIS Data Validation and Reconciliation - 22feb2023 2Carlen Mae L. YacapinNo ratings yet
- Identification of High Risk PregnanciesDocument15 pagesIdentification of High Risk PregnanciesVidya Ganesh100% (12)
- Narrative Review of Pelvic Floor Muscle Training For Childbearing Women-Why, When, What, and HowDocument12 pagesNarrative Review of Pelvic Floor Muscle Training For Childbearing Women-Why, When, What, and HowLéa Cinthia Silva do NascimentoNo ratings yet
- Respiratory Stimulants, Expectorants and Anti-TussivesDocument16 pagesRespiratory Stimulants, Expectorants and Anti-TussivesAshish Mittal0% (3)
- Anal Sphincter Tears at Vaginal Delivery Risk.5Document8 pagesAnal Sphincter Tears at Vaginal Delivery Risk.5Melian AnitaNo ratings yet
- Article - Yoga For Women PDFDocument8 pagesArticle - Yoga For Women PDFinsane88No ratings yet
- HSB Assignment 3Document2 pagesHSB Assignment 3api-550790092No ratings yet
- Ma. Christina B. Celdran - Oraa, RN MANDocument59 pagesMa. Christina B. Celdran - Oraa, RN MANEuscelle Grace Limen100% (1)
- A Guide To Family Planning For Community Health Workers and Their ClientsDocument50 pagesA Guide To Family Planning For Community Health Workers and Their ClientsPaul Mark PilarNo ratings yet
- Culture - Health Beliefs and PracticesDocument2 pagesCulture - Health Beliefs and PracticesCheska YsabelleNo ratings yet
- PGD 5 AnswersDocument14 pagesPGD 5 AnswersDianeNo ratings yet
- I. Listening Comprehension: Teacher: Ms. Ikram Ayachi School: Sidi Boubakker School Level: 9 Grade Date: 08/02/2022Document3 pagesI. Listening Comprehension: Teacher: Ms. Ikram Ayachi School: Sidi Boubakker School Level: 9 Grade Date: 08/02/2022Elizabeth CerqueiraNo ratings yet
- Piis0190962223001639 PDFDocument8 pagesPiis0190962223001639 PDFLighthopeNo ratings yet
- Pregnancy Choices: Raising The Baby, Adoption, and AbortionDocument3 pagesPregnancy Choices: Raising The Baby, Adoption, and AbortionSebastian Sandoval ChavarroNo ratings yet
- Pregnant Abdomen ExamDocument4 pagesPregnant Abdomen ExamAmiel Francisco ReyesNo ratings yet
- Uganda National Adolesecent Health PolicyDocument27 pagesUganda National Adolesecent Health PolicyBashir KabuyeNo ratings yet
- Obstetrics HistoryDocument3 pagesObstetrics HistorymakepaNo ratings yet
- Criteria For Transvaginal Sonographic Diagnosis of Ectopic PregnancyDocument6 pagesCriteria For Transvaginal Sonographic Diagnosis of Ectopic PregnancyDinorah MarcelaNo ratings yet
- Toxemia in PregnancyDocument21 pagesToxemia in PregnancyRiajoy Asis100% (5)
- Clinical Aromatherapy For Pregnancy, Labor and PostpartumDocument1 pageClinical Aromatherapy For Pregnancy, Labor and Postpartumcamila.was.hereNo ratings yet
- Rules On LeaveDocument9 pagesRules On LeaveAnonymous 1lYUUy5T89% (9)
- Article 254. Discharge of Firearms. - Any Person Who Shall Shoot at Another With Any Firearm Shall Suffer The PenaltyDocument8 pagesArticle 254. Discharge of Firearms. - Any Person Who Shall Shoot at Another With Any Firearm Shall Suffer The PenaltyReyes BeeNo ratings yet