Download as pdf or txt
You might also like
- Get Tested: STD Vs Sti STD Vs StiDocument2 pagesGet Tested: STD Vs Sti STD Vs StiJanna May Villafuerte100% (2)
- Quick Guide To Cardiopulmonary Care 4th EditionDocument185 pagesQuick Guide To Cardiopulmonary Care 4th EditionLorenzo Romero AlbarranNo ratings yet
- Basics of Broncho ankitDocument54 pagesBasics of Broncho ankitsandeepsanyasi99No ratings yet
- Improving perioperative care in low-resource settings with goal-directed therapy_ a narrative reviewDocument5 pagesImproving perioperative care in low-resource settings with goal-directed therapy_ a narrative reviewDsm DsmNo ratings yet
- HEMOPTISISDocument6 pagesHEMOPTISISJufrialdy AldyNo ratings yet
- Etm 13 5 2259 PDFDocument4 pagesEtm 13 5 2259 PDFdicky nanda muzidaNo ratings yet
- Massive Hemoptysis An Update On The Role of Bronchoscopy in Diagnosis and Management PDFDocument21 pagesMassive Hemoptysis An Update On The Role of Bronchoscopy in Diagnosis and Management PDFdoc_next_doorNo ratings yet
- DR Oea KhairsyafDocument30 pagesDR Oea KhairsyafErdyNo ratings yet
- 10 1016@j Bja 2020 08 060Document9 pages10 1016@j Bja 2020 08 060kenjiNo ratings yet
- Hemodynamic Impact of Isobaric Levobupivacaine Versus Hyperbaric Bupivacaine For Subarachnoid Anesthesia in Patients Aged 65 and Older Undergoing Hip SurgeryDocument11 pagesHemodynamic Impact of Isobaric Levobupivacaine Versus Hyperbaric Bupivacaine For Subarachnoid Anesthesia in Patients Aged 65 and Older Undergoing Hip SurgeryHana MitayaniNo ratings yet
- Part2 Hypovolemid Trauma Vs Septic Shock (1) .EditedDocument7 pagesPart2 Hypovolemid Trauma Vs Septic Shock (1) .EditedKinkumba MakitaNo ratings yet
- SRI 1 - 2020 Airway Management in Critical Illness An UpdateDocument11 pagesSRI 1 - 2020 Airway Management in Critical Illness An UpdateAlejandro OlivaNo ratings yet
- Plotnikow 2017Document3 pagesPlotnikow 2017Julieta EvangelistaNo ratings yet
- Management of Postoperative HypoxemiaDocument14 pagesManagement of Postoperative HypoxemiaFavio Alvarez De BejarNo ratings yet
- Parallel Technique of Endobronchial Balloon Catheter Tamponade For Transient Alleviation of Massive HemoptysisDocument3 pagesParallel Technique of Endobronchial Balloon Catheter Tamponade For Transient Alleviation of Massive HemoptysisNadia Mrz Mattew MuseNo ratings yet
- SeminarioDocument14 pagesSeminarioochoa4aNo ratings yet
- Ropvacaina VS Lidocaina Premdicacion IotDocument6 pagesRopvacaina VS Lidocaina Premdicacion IotFaith Lu PenalozaNo ratings yet
- A Systematic Approach To The Management of Massive Hemoptysis.Document18 pagesA Systematic Approach To The Management of Massive Hemoptysis.Hitomi-No ratings yet
- US Pulmón para Manejo de Atelectasias PerioperatoriasDocument11 pagesUS Pulmón para Manejo de Atelectasias PerioperatoriasJURAGOMANo ratings yet
- Anesthesia For BronchosDocument11 pagesAnesthesia For Bronchosadink mochammadNo ratings yet
- International Journal of Surgery Case ReportsDocument5 pagesInternational Journal of Surgery Case ReportschrisantyNo ratings yet
- Respiratory Medicine Case ReportsDocument3 pagesRespiratory Medicine Case ReportsAleesya SyahidNo ratings yet
- Respiratory Variations in Arterial Pressure For Guiding Fluid Management in Mechanically VDocument8 pagesRespiratory Variations in Arterial Pressure For Guiding Fluid Management in Mechanically VThászk AstrosaNo ratings yet
- 1 s2.0 S0104001421000385 MainDocument4 pages1 s2.0 S0104001421000385 MainSuci dwi CahyaNo ratings yet
- Operative Hysteroscopy IntravascularDocument4 pagesOperative Hysteroscopy IntravascularWilson rocha untojaNo ratings yet
- Massive Right Hemothorax As The Source of Hemorrhagic Shock After Laparoscopic Cholecystectomy - Case Report of A Rare Intraoperative ComplicationDocument3 pagesMassive Right Hemothorax As The Source of Hemorrhagic Shock After Laparoscopic Cholecystectomy - Case Report of A Rare Intraoperative ComplicationDaniel LesmanaNo ratings yet
- Articol Roberts OrlDocument4 pagesArticol Roberts OrlSabina BădilăNo ratings yet
- Schwameis 2015Document9 pagesSchwameis 2015No NamedNo ratings yet
- Respiratory Medicine Case Reports: Lauren A. Sharan, Thea P. Price, Boyd Hehn, David Manoff, Scott W. CowanDocument4 pagesRespiratory Medicine Case Reports: Lauren A. Sharan, Thea P. Price, Boyd Hehn, David Manoff, Scott W. CowanJha BhoenkNo ratings yet
- Embolization of Bronchial Arteries For The Treatment of HEMOPTYSIS. Update and Literature ReviewDocument20 pagesEmbolization of Bronchial Arteries For The Treatment of HEMOPTYSIS. Update and Literature ReviewHai SheikhNo ratings yet
- Reseccion Pulmonar en Hemoptisis SeveraDocument10 pagesReseccion Pulmonar en Hemoptisis SeverarafodocNo ratings yet
- Case 2Document4 pagesCase 2Malavika RaoNo ratings yet
- Less Invasive Hemodynamic Monitoring in Critically Ill PatientsDocument11 pagesLess Invasive Hemodynamic Monitoring in Critically Ill Patientsهبة بسمان شاكرNo ratings yet
- Emborrhoid Technique Performed On A Patient With Portal Hypertension and Chronic Hemorrhoidal Bleeding As A Salvage TherapyDocument4 pagesEmborrhoid Technique Performed On A Patient With Portal Hypertension and Chronic Hemorrhoidal Bleeding As A Salvage TherapydianisaindiraNo ratings yet
- Resuscitative Endovascular Balloon Occlusion of The Aorta (REBOA) : An Updated ReviewDocument9 pagesResuscitative Endovascular Balloon Occlusion of The Aorta (REBOA) : An Updated ReviewLuis-alfredo Perez Bolde HernandezNo ratings yet
- Mottling ScoreDocument5 pagesMottling ScoreAriadna AncavilNo ratings yet
- Mondoni Et AlDocument11 pagesMondoni Et AlpandylouisputraNo ratings yet
- Apm 12 151 PDFDocument4 pagesApm 12 151 PDFFityan Aulia RahmanNo ratings yet
- Cheng 2017Document6 pagesCheng 2017Lepaca KliffothNo ratings yet
- Contraindications: "Flexible Bronchoscopy in Adults: Overview"Document8 pagesContraindications: "Flexible Bronchoscopy in Adults: Overview"VasFel GicoNo ratings yet
- SUBMITTED TO - Resp. Mr. Somorjit SinghDocument8 pagesSUBMITTED TO - Resp. Mr. Somorjit SinghSimran JosanNo ratings yet
- Stefano Malinverni A Retrospective Comparison ofDocument8 pagesStefano Malinverni A Retrospective Comparison ofAssessoria da Gerência Geral HEHANo ratings yet
- Parapneumonic Effusion: PathophysiologyDocument3 pagesParapneumonic Effusion: PathophysiologyMerry Dame Cristy PaneNo ratings yet
- Ett OkDocument8 pagesEtt OkOman HendiNo ratings yet
- Jurnal Review PulmoDocument33 pagesJurnal Review PulmoGilang FajriansyahNo ratings yet
- Resuscitativeendovascular Balloonocclusionofthe Aorta:: A Practical ReviewDocument18 pagesResuscitativeendovascular Balloonocclusionofthe Aorta:: A Practical ReviewJulian SanchezNo ratings yet
- Cuidados Neuromuscular 2017Document12 pagesCuidados Neuromuscular 2017Tami SchumacherNo ratings yet
- Minimally Invasive Surgery, Robotics, and NaturalDocument65 pagesMinimally Invasive Surgery, Robotics, and Naturalvan016_bunny50% (2)
- Value of Bronchoscopy and Thoracoscopy in Respiratory MedicineDocument36 pagesValue of Bronchoscopy and Thoracoscopy in Respiratory MedicineMokwe Xavier CharlesNo ratings yet
- 2 RevistaDocument9 pages2 RevistaLucas QuilmesNo ratings yet
- Pneumonectomy S RT RpaDocument4 pagesPneumonectomy S RT RpagireeshsachinNo ratings yet
- Luaran Perdarahan Intraventrikel Yang Dilakukan Operasi Di Departemen Bedah Saraf Rsupn Dr. Cipto MangunkusumoDocument5 pagesLuaran Perdarahan Intraventrikel Yang Dilakukan Operasi Di Departemen Bedah Saraf Rsupn Dr. Cipto MangunkusumoMerry AndrianyNo ratings yet
- Chest Wall, Lung, MediastinumDocument124 pagesChest Wall, Lung, MediastinumKenn BrillanteNo ratings yet
- Case Study Residency2Document21 pagesCase Study Residency2computerwhiz42985No ratings yet
- Medicine: Lymphangiomatosis Involving The Pulmonary and Extrapulmonary Lymph Nodes and Surrounding Soft TissueDocument5 pagesMedicine: Lymphangiomatosis Involving The Pulmonary and Extrapulmonary Lymph Nodes and Surrounding Soft TissueAngel FloresNo ratings yet
- JURDING 1 - Usefulness of Lung Ultrasound For Early Detection of Hospital-Acquired Pneumonia in Cardiac Critically Ill Patients On Venoarterial Extracorporeal Membrane OxygenationDocument10 pagesJURDING 1 - Usefulness of Lung Ultrasound For Early Detection of Hospital-Acquired Pneumonia in Cardiac Critically Ill Patients On Venoarterial Extracorporeal Membrane OxygenationLivia Meidy UbayidNo ratings yet
- CLN 66 01 107 PDFDocument5 pagesCLN 66 01 107 PDFGloria KartikaNo ratings yet
- Medical History Physical Exam Chest X-Ray Clinical Signs Breath Sounds Fremitus Pleural Friction Rub Egophony TrachealDocument8 pagesMedical History Physical Exam Chest X-Ray Clinical Signs Breath Sounds Fremitus Pleural Friction Rub Egophony TrachealCholo Mercado ManalastasNo ratings yet
- BronchosDocument12 pagesBronchosAhmad ShyoukhNo ratings yet
- Standard Treatment Guidelines Interventional Radiology: Ministry of Health & Family Welfare Govt. of IndiaDocument75 pagesStandard Treatment Guidelines Interventional Radiology: Ministry of Health & Family Welfare Govt. of IndiaKaustubhNo ratings yet
- HemoptisisDocument7 pagesHemoptisiswiliaNo ratings yet
- Pi Is 1470204519304565Document13 pagesPi Is 1470204519304565Agung Budi PamungkasNo ratings yet
- Wound Dressing Checklist SKL 112 FINAL EDITDocument5 pagesWound Dressing Checklist SKL 112 FINAL EDITCamille GuintoNo ratings yet
- Balio Ox-580 Brochure enDocument4 pagesBalio Ox-580 Brochure enMo AlyNo ratings yet
- Madison Solomon ResumeDocument2 pagesMadison Solomon Resumeapi-321571692No ratings yet
- Handbook of Pediatric Surgery 2010Document454 pagesHandbook of Pediatric Surgery 2010Clau Jorquera Castillo100% (1)
- 733-Article Text-1692-1-10-20210609Document2 pages733-Article Text-1692-1-10-20210609Jaydev DegloorkarNo ratings yet
- SepsisDocument8 pagesSepsisLEONELA VALDES CABELLONo ratings yet
- GASTRECTOMYDocument3 pagesGASTRECTOMYMaria Ydela MeradoresNo ratings yet
- Gabriela Skoczylas Resume Career FairDocument1 pageGabriela Skoczylas Resume Career Fairapi-435929154No ratings yet
- Botox For Plantar FasciitisDocument31 pagesBotox For Plantar FasciitisAngie BongNo ratings yet
- Bmet 262 Outline 2022 2023Document12 pagesBmet 262 Outline 2022 2023Emmanuel PrahNo ratings yet
- Dressing and Bandaging in First Aid: Wound Healing BandageDocument8 pagesDressing and Bandaging in First Aid: Wound Healing BandageRosalouise P. UngabNo ratings yet
- Ncbi List of Books and Dental ArticlesDocument6 pagesNcbi List of Books and Dental ArticlesIulia Isacov0% (1)
- UPDRS v1.0 Annotated CRF PDFDocument8 pagesUPDRS v1.0 Annotated CRF PDFAnaaaerobiosNo ratings yet
- Microbiology Pharm D 2nd Year Question BankDocument13 pagesMicrobiology Pharm D 2nd Year Question Bankshasvina05No ratings yet
- Dr. Heston Standing Orders LandscapeDocument3 pagesDr. Heston Standing Orders LandscapeJosh Heston100% (1)
- American Academy of Sleep Medicine Position Paper For The Use of A Home Sleep Apnea Test For The Diagnosis of OSA in ChildrenDocument5 pagesAmerican Academy of Sleep Medicine Position Paper For The Use of A Home Sleep Apnea Test For The Diagnosis of OSA in ChildrenBenja GuzmánNo ratings yet
- Anatomy and Cardiovascular AssessmentDocument52 pagesAnatomy and Cardiovascular AssessmentNaomi Anne AsuntoNo ratings yet
- The Benefits of Golf For Your HealthDocument2 pagesThe Benefits of Golf For Your Healthlifemaantra comNo ratings yet
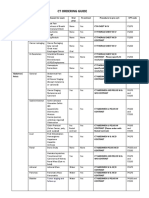
- CT Ordering Guide: Tumor Staging and Follow UpDocument2 pagesCT Ordering Guide: Tumor Staging and Follow UpanonNo ratings yet
- Canine Brucellosis Old Foe and Reemerging ScourgeDocument17 pagesCanine Brucellosis Old Foe and Reemerging ScourgeMargarita CCNo ratings yet
- Supracondylar FractureDocument4 pagesSupracondylar FractureHemanath SinnathambyNo ratings yet
- Nursing Dosage Rounding RulesDocument2 pagesNursing Dosage Rounding RulesAlan AmatoNo ratings yet
- Gingivitis & PeriodontitisDocument24 pagesGingivitis & PeriodontitisHafid Nur ArzanudinNo ratings yet
- Anterior Implant EstheticsDocument9 pagesAnterior Implant EstheticsRatih Cynthia100% (1)
- Failure To Thrive - AAPDocument11 pagesFailure To Thrive - AAPAlexNo ratings yet
- SDG3Document14 pagesSDG3norizan husainNo ratings yet
- Manila Police District (MPD) As of January 2022: Action PNCO, DSTU OIC, Training Section C, DPRMDDocument15 pagesManila Police District (MPD) As of January 2022: Action PNCO, DSTU OIC, Training Section C, DPRMDShan Dave TupasNo ratings yet