Download as pdf or txt
You might also like
- Ethical Dimensions in The Health Professions PDFDocument2 pagesEthical Dimensions in The Health Professions PDFJames0% (7)
- The Impact of Working From Home For The EmployeesDocument78 pagesThe Impact of Working From Home For The EmployeesMhild Gandawali92% (12)
- Megacode Testing ScenariosDocument12 pagesMegacode Testing Scenariosmonsalg2502No ratings yet
- Emergency Department Standing OrdersDocument12 pagesEmergency Department Standing OrdersJ Russel DichosoNo ratings yet
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- LiverpoolSedation ManagementDocument9 pagesLiverpoolSedation ManagementTheresia Avila KurniaNo ratings yet
- LPN DELEGATION and PRIORITIZING AND MOREDocument38 pagesLPN DELEGATION and PRIORITIZING AND MOREDebra PowellNo ratings yet
- Reflective JournalDocument8 pagesReflective Journalapi-486025324100% (1)
- White Spot LesionsDocument8 pagesWhite Spot LesionsMicéli Guimarães BlayaNo ratings yet
- MED-F-003 OPD Patient Assesment NurseDocument2 pagesMED-F-003 OPD Patient Assesment Nursedrakmalik71No ratings yet
- Surgery PearlsDocument2 pagesSurgery Pearlspatriciaatan1497No ratings yet
- Health Failure Clinical PathwayDocument2 pagesHealth Failure Clinical Pathwayferishandy bagaskaraNo ratings yet
- Heart Failure Clinical Pathway TemplateDocument3 pagesHeart Failure Clinical Pathway Templategusmarinda fauziahNo ratings yet
- Pathway Fractured HIPDocument7 pagesPathway Fractured HIPDewi Ratna SariNo ratings yet
- PREOPinguinalherniaDocument2 pagesPREOPinguinalherniapatriciaatan1497No ratings yet
- PearlsDocument2 pagesPearlspatriciaatan1497No ratings yet
- PearlsDocument2 pagesPearlspatriciaatan1497No ratings yet
- Surgery PearlsDocument2 pagesSurgery Pearlspatriciaatan1497No ratings yet
- PearlsDocument2 pagesPearlspatriciaatan1497No ratings yet
- Surgery PearlsDocument2 pagesSurgery Pearlspatriciaatan1497No ratings yet
- Clinical Pathway - Stroke Without Thrombolytic TherapyDocument4 pagesClinical Pathway - Stroke Without Thrombolytic TherapysiusiuwidyantoNo ratings yet
- ICU GoalDocument1 pageICU GoalChiu LeoNo ratings yet
- Module 6 Elaborate - SanchezDocument14 pagesModule 6 Elaborate - SanchezKaye Cyril SanchezNo ratings yet
- Module 6 Elaborate - SanchezDocument14 pagesModule 6 Elaborate - SanchezKaye Cyril SanchezNo ratings yet
- Rot ExamDocument2 pagesRot ExamRalph Elvin MacanlalayNo ratings yet
- Discharge Plan FormatDocument3 pagesDischarge Plan FormatYuraNo ratings yet
- Clinical Pathway For Hypertensive Urgency (Revised)Document6 pagesClinical Pathway For Hypertensive Urgency (Revised)Heide Danica A. BaltazarNo ratings yet
- JCI Standards Only 6th Ed HospitalDocument12 pagesJCI Standards Only 6th Ed HospitalHengkyNo ratings yet
- My Hospital FacilitiesDocument10 pagesMy Hospital Facilities3E, KENNADY KARUNAKARAN, PRINCENo ratings yet
- Vicpostoporderform WebDocument2 pagesVicpostoporderform WebJunaid ShahNo ratings yet
- Stroke Guidelines: Cva Critical Pathway Department of NeurologyDocument5 pagesStroke Guidelines: Cva Critical Pathway Department of NeurologyplethoraldorkNo ratings yet
- Fdar Charting - Imh-1Document34 pagesFdar Charting - Imh-1Rekkusu MakeinuNo ratings yet
- Characteristics of Thrombotic CVA: Transition To Neurological Nursing in The United States of AmericaDocument22 pagesCharacteristics of Thrombotic CVA: Transition To Neurological Nursing in The United States of AmericaAnn MavitiNo ratings yet
- Tool 3 For Adapting and PrintingDocument1 pageTool 3 For Adapting and PrintingAddisNo ratings yet
- Greyzones 2023 V7.1Document12 pagesGreyzones 2023 V7.1Abdel-hafiz MamounNo ratings yet
- ACI Cognition Screening For Older AdultsDocument2 pagesACI Cognition Screening For Older AdultsBadrun IbrahimNo ratings yet
- Clinical AttendanceDocument1 pageClinical AttendancedeemagNo ratings yet
- Interdisciplinary Plan of Care and Patient EducationDocument26 pagesInterdisciplinary Plan of Care and Patient Educationhuggr84629No ratings yet
- Case Study CHNDocument5 pagesCase Study CHNIsaiah RabangNo ratings yet
- Truspected Stroke AlgorithmDocument4 pagesTruspected Stroke Algorithmtri wahyunoNo ratings yet
- ANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientDocument5 pagesANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientjackydoodsonNo ratings yet
- Module 4 OtpDocument42 pagesModule 4 Otpzack NourNo ratings yet
- Delirium: Lindsay Trantum ACNP-BC VUMC Neuroscience ICUDocument22 pagesDelirium: Lindsay Trantum ACNP-BC VUMC Neuroscience ICUarunNo ratings yet
- Hydrocephalus Clinical Pathway: James L. PatigayonDocument6 pagesHydrocephalus Clinical Pathway: James L. PatigayonJayson OlileNo ratings yet
- Surgery PearlsDocument2 pagesSurgery Pearlspatriciaatan1497No ratings yet
- Newly Revise Emergency Nursing 1Document65 pagesNewly Revise Emergency Nursing 1Mikee PaningbatanNo ratings yet
- A-D-C A V-A-N-D-I-M-L-S: Hospital Admission Orders & ObjectivesDocument2 pagesA-D-C A V-A-N-D-I-M-L-S: Hospital Admission Orders & Objectivescjro99No ratings yet
- NIHSSDocument15 pagesNIHSSganiaNo ratings yet
- Pharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDocument20 pagesPharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDzaky UlayyaNo ratings yet
- NCP and Focus Charting For PainDocument3 pagesNCP and Focus Charting For PainArian May MarcosNo ratings yet
- Nursing Recruitment Skills Checklist: Guidance or DirectionDocument4 pagesNursing Recruitment Skills Checklist: Guidance or DirectionKRIZZEL CATAMINNo ratings yet
- Sedation in Critically IllDocument32 pagesSedation in Critically IllSamantha Deshapriya100% (1)
- Assessment and Management of Delirium in Pediatric PatientsDocument7 pagesAssessment and Management of Delirium in Pediatric PatientsEunike Karamoy100% (1)
- Electrolyte ImbalanceDocument4 pagesElectrolyte ImbalanceDoneva Lyn MedinaNo ratings yet
- Total Hip and Knee ReplacementsDocument57 pagesTotal Hip and Knee ReplacementsBryndenNo ratings yet
- ABCDEF Bundle WebcastDocument42 pagesABCDEF Bundle WebcastsoulstakersNo ratings yet
- Use of Restraint Form - Education Points For CompletionDocument2 pagesUse of Restraint Form - Education Points For Completionnostra83No ratings yet
- Health AssessmentDocument12 pagesHealth Assessmentjmzxmdy597No ratings yet
- ST ND RD TH: ST ND RD TH ST ND RD TH ST ND RD TH ST ND RD TH ST ND RD TH ST ND RD THDocument3 pagesST ND RD TH: ST ND RD TH ST ND RD TH ST ND RD TH ST ND RD TH ST ND RD TH ST ND RD THFrances PurisimaNo ratings yet
- Nursing Care Plan Funds 2Document7 pagesNursing Care Plan Funds 2Yash RamawatNo ratings yet
- Assistant Nurse Comp Check 2018Document3 pagesAssistant Nurse Comp Check 2018pmnh nqps0% (1)
- Interfacility Transfer ChecklistDocument2 pagesInterfacility Transfer ChecklistDewi Ratna Sari0% (1)
- The COAT & Review Approach: How to recognise and manage unwell patientsFrom EverandThe COAT & Review Approach: How to recognise and manage unwell patientsRating: 5 out of 5 stars5/5 (1)
- Risk Management Framework & Risk Management ProcessDocument47 pagesRisk Management Framework & Risk Management Processratna kartikaNo ratings yet
- Pengenalan Ultrasonografi Organ HepatobilierDocument29 pagesPengenalan Ultrasonografi Organ Hepatobilierratna kartikaNo ratings yet
- Status Lokalis PasienDocument1 pageStatus Lokalis Pasienratna kartikaNo ratings yet
- SERTIFIKATDocument2 pagesSERTIFIKATratna kartikaNo ratings yet
- Jadwal Agust Sept 2022 KeduaDocument5 pagesJadwal Agust Sept 2022 Keduaratna kartikaNo ratings yet
- Pain ManagementDocument40 pagesPain ManagementPutra Pratama100% (1)
- Xyz Clinical Evaluation Tool-Yastrzemski 1Document3 pagesXyz Clinical Evaluation Tool-Yastrzemski 1api-323159742No ratings yet
- Prevention of Deep Vein ThrombosisDocument11 pagesPrevention of Deep Vein ThrombosisSindhuja vivekanandhanNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Second Reminder Letter Without PrejudiceDocument1 pageParamount Health Services & Insurance Tpa Private Limited: Second Reminder Letter Without PrejudiceRishabh ShuklaNo ratings yet
- Plateletrich Plasma Injections For Knee Osteoarthritis PDF 1899874048147909Document5 pagesPlateletrich Plasma Injections For Knee Osteoarthritis PDF 1899874048147909JanetNo ratings yet
- JKKP 8 - Register of Occupational Accidents, Dangerous Occurrence, Occupational Poisoning and Occupational DiseaseDocument5 pagesJKKP 8 - Register of Occupational Accidents, Dangerous Occurrence, Occupational Poisoning and Occupational Diseasepalanii5No ratings yet
- CisplatinDocument3 pagesCisplatinRicey MelegritoNo ratings yet
- A 2-Year-Old Child With Cough and Respiratory Distress: Family Medicine and Community HealthDocument2 pagesA 2-Year-Old Child With Cough and Respiratory Distress: Family Medicine and Community HealthElse FashiosNo ratings yet
- Economics Project: Country Risk AnalysisDocument39 pagesEconomics Project: Country Risk AnalysistanmayNo ratings yet
- Assingment ON Ethical and Psychosocial Issues in Genetic TestingDocument17 pagesAssingment ON Ethical and Psychosocial Issues in Genetic TestingVaishali JainarainNo ratings yet
- Instructions For New (First-Time) First Aid-CPR-AED Instructor Candidates (Oct 2019)Document4 pagesInstructions For New (First-Time) First Aid-CPR-AED Instructor Candidates (Oct 2019)مريم محمدNo ratings yet
- Dr. X and The Quest For Food Safety Video Review Teacher KeyDocument8 pagesDr. X and The Quest For Food Safety Video Review Teacher KeyemNo ratings yet
- Assisting Bone Marrow Aspiration DraftDocument6 pagesAssisting Bone Marrow Aspiration Draftabcde pwnjabiNo ratings yet
- Orbital Metastasis of A Pediatric Nasopharyngeal Carcinoma A Rare Case ReportDocument4 pagesOrbital Metastasis of A Pediatric Nasopharyngeal Carcinoma A Rare Case ReportInternational Journal of Innovative Science and Research Technology100% (1)
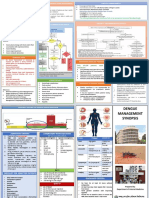
- Dengue Management Synopsis BSMMUDocument2 pagesDengue Management Synopsis BSMMURakibk65No ratings yet
- I Summary Family MedicineDocument185 pagesI Summary Family MedicineModa ModyNo ratings yet
- ICS Standards 2024.Document1,305 pagesICS Standards 2024.Urología GinecológicaNo ratings yet
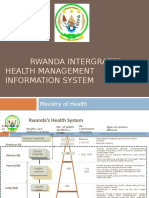
- Rwanda Intergrated Health Management Information SystemDocument11 pagesRwanda Intergrated Health Management Information SystemSanjeev ChouguleNo ratings yet
- Meningococcal Infection in ChildrenDocument6 pagesMeningococcal Infection in ChildrenAdrian KhomanNo ratings yet
- LaborDocument16 pagesLaborREALYN ZAMBASNo ratings yet
- My CVDocument4 pagesMy CVOsama AmoudiNo ratings yet
- Periosakthi - 2023 Brouchure-5Document4 pagesPeriosakthi - 2023 Brouchure-5sasi dharanNo ratings yet
- HEALTH 9 EXAM (2nd Quarter) QuestionsDocument3 pagesHEALTH 9 EXAM (2nd Quarter) QuestionsKert Cyrel Romero0% (1)
- Lower Respiratory InfectionDocument71 pagesLower Respiratory Infectionpaulyn ramos100% (1)
- Daycare Fact SheetDocument1 pageDaycare Fact SheetJoana R. SilvaNo ratings yet
- Fajardo Max JR Plumbing Design and Estimate 2nd Editionpdf PDF FreeDocument175 pagesFajardo Max JR Plumbing Design and Estimate 2nd Editionpdf PDF FreeBry Ann BarawidNo ratings yet
- Scope Of-Practice For Entry Level Programmes 17.08.2020Document36 pagesScope Of-Practice For Entry Level Programmes 17.08.2020dorothy kageniNo ratings yet