Download as docx, pdf, or txt
You might also like
- Atls Questions and AnswersDocument14 pagesAtls Questions and AnswersAgil Rumboko Sumitro50% (6)
- Renal ExamDocument12 pagesRenal ExamCamille Espinosa100% (7)
- Clinical Reasoning Questions - CollaborationDocument4 pagesClinical Reasoning Questions - CollaborationMohammad OmarNo ratings yet
- Urinary Tract Infection Nursing-Care-PlanDocument3 pagesUrinary Tract Infection Nursing-Care-PlanRnspeakcomNo ratings yet
- Bruno Breitmeyer-Blindspots - The Many Ways We Cannot See-Oxford University Press, USA (2010) PDFDocument281 pagesBruno Breitmeyer-Blindspots - The Many Ways We Cannot See-Oxford University Press, USA (2010) PDFFrancisco Villar100% (1)
- Cues/ Clues Diagnosis Analysis Objectives Intervention S Rationale EvaluationDocument8 pagesCues/ Clues Diagnosis Analysis Objectives Intervention S Rationale EvaluationRecah PangilinanNo ratings yet
- The Correlation Between Disease Stage and Pulmonary Edema Assessed With Chest Xray in Chronic Kidney Disease PatientsDocument6 pagesThe Correlation Between Disease Stage and Pulmonary Edema Assessed With Chest Xray in Chronic Kidney Disease PatientsAnnisa RabbaniNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care Planusama_salaymehNo ratings yet
- Nursing Care Plan: Cues Nursing Diagnosis Analysis Goal and Objectives Interventions Rationale EvaluationDocument3 pagesNursing Care Plan: Cues Nursing Diagnosis Analysis Goal and Objectives Interventions Rationale EvaluationCalimlim KimNo ratings yet
- Concept Map (Aplastic Anemia) b1Document6 pagesConcept Map (Aplastic Anemia) b1Ran PioloNo ratings yet
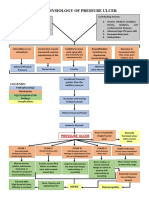
- Pathophysiology of Pressure UlcerDocument1 pagePathophysiology of Pressure UlcerSTORAGE FILENo ratings yet
- Drug StudyDocument8 pagesDrug StudyJohn Ronald P. RamosNo ratings yet
- Evidence-Based Nursing: I. Clinical QuestionDocument4 pagesEvidence-Based Nursing: I. Clinical QuestionRay Jorge MarmetoNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation IndependentDocument1 pageAssessment Diagnosis Planning Intervention Rationale Evaluation IndependentAdhaNo ratings yet
- BSN4D-SG2 DM Type2Document201 pagesBSN4D-SG2 DM Type2Charisse CaydanNo ratings yet
- LOG101 Exercise No. 2 - Types of Definitions 20230217091032Document2 pagesLOG101 Exercise No. 2 - Types of Definitions 20230217091032Daniella TimbolNo ratings yet
- Clinical Features and Diagnosis of Hemophagocytic Lymphohistiocytosis - UpToDateDocument27 pagesClinical Features and Diagnosis of Hemophagocytic Lymphohistiocytosis - UpToDateSalvatore ScutoNo ratings yet
- Sample Case Presentation - Occult BacteremiaDocument51 pagesSample Case Presentation - Occult BacteremiaPrecious Gutierrez BagazinNo ratings yet
- This Study Resource Was Shared Via: Nursing Care Plan FormDocument3 pagesThis Study Resource Was Shared Via: Nursing Care Plan FormissaiahnicolleNo ratings yet
- NCP PainDocument2 pagesNCP PainApril_Ivy_Raga_3835No ratings yet
- 4th Yr. Med Cardio Module Question - Copy-1Document11 pages4th Yr. Med Cardio Module Question - Copy-1Sheda BondNo ratings yet
- Problem: Pain at 6/10 For A "Sore Right Shoulder" Date Evaluated: December 14, 2020Document2 pagesProblem: Pain at 6/10 For A "Sore Right Shoulder" Date Evaluated: December 14, 2020florenzoNo ratings yet
- NCP For Ulnar SurgeryDocument5 pagesNCP For Ulnar SurgeryjiloNo ratings yet
- Subjective: Objective: Short Term: Independent: Independent: Short TermDocument2 pagesSubjective: Objective: Short Term: Independent: Independent: Short TermJohn Patrick CuencoNo ratings yet
- Propranolol, Prophylactic Warfarin, Low Molecular Weight Heparin (LMWH), Furosemide, AntibioticsDocument8 pagesPropranolol, Prophylactic Warfarin, Low Molecular Weight Heparin (LMWH), Furosemide, AntibioticsArlyn MarcelinoNo ratings yet
- NCP KoDocument1 pageNCP Kojiellianemae100% (1)
- Circulating Nurse ScriptDocument1 pageCirculating Nurse Scriptmaga.abigail.bsnNo ratings yet
- Case Pres A1-RhdDocument11 pagesCase Pres A1-RhdCharm TanyaNo ratings yet
- Nursing Care Plan: Subjective: During 8 Hours Nursing Management: (5) After 8 HoursDocument4 pagesNursing Care Plan: Subjective: During 8 Hours Nursing Management: (5) After 8 HoursRawan KhateebNo ratings yet
- Scribd 020922 Case Study-Oncology A&kDocument2 pagesScribd 020922 Case Study-Oncology A&kKellie DNo ratings yet
- Impact of The Ageing Member To The FamilyDocument5 pagesImpact of The Ageing Member To The FamilyAngel Joy CatalanNo ratings yet
- NCP Acute PainDocument5 pagesNCP Acute PainEzra TuanNo ratings yet
- Case 1 - Pneumonia (Final)Document4 pagesCase 1 - Pneumonia (Final)Joegie ArioNo ratings yet
- DX Fracture PDFDocument8 pagesDX Fracture PDFSherree HayesNo ratings yet
- Nursing Care Plans For Activity IntoleranceDocument4 pagesNursing Care Plans For Activity IntolerancethebigtwirpNo ratings yet
- Community Health Nursing-1 Unit 2Document52 pagesCommunity Health Nursing-1 Unit 2Asif Ali LashariNo ratings yet
- NCPDocument2 pagesNCPChe2x^^100% (2)
- NCP Hip FractureDocument5 pagesNCP Hip FractureCherry Ann BalagotNo ratings yet
- Student Nurses' Community: NURSING CARE PLAN Functional Urinary IncontinenceDocument4 pagesStudent Nurses' Community: NURSING CARE PLAN Functional Urinary IncontinenceJez RarangNo ratings yet
- NCPDocument5 pagesNCPMcmc Ryan Ferdinand GutierrezNo ratings yet
- Case CHFDocument10 pagesCase CHFAgnes Erlita Distriani Patade50% (2)
- NCP On DyspneaDocument5 pagesNCP On DyspneaDizzy BualanNo ratings yet
- Nursing Management of Dengue FeverDocument45 pagesNursing Management of Dengue FeverMadhavi ModaNo ratings yet
- FluidDocument45 pagesFluidloglesb1No ratings yet
- NCP Risk InfectionDocument1 pageNCP Risk InfectionEni RahmawatiNo ratings yet
- E000779 FullDocument19 pagesE000779 Fullmartina silalahiNo ratings yet
- NCPDocument8 pagesNCPAriaNo ratings yet
- Basilar Skull FractureDocument16 pagesBasilar Skull FractureRindahMDNo ratings yet
- 5 - Respiratory AssessmentDocument61 pages5 - Respiratory AssessmentAbboud Ali100% (1)
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Objectives Interventions Rationale EvaluationJP2001100% (1)
- Pleural EffusionDocument12 pagesPleural EffusionWan HafizNo ratings yet
- Fludrocortisone (Florinef)Document17 pagesFludrocortisone (Florinef)passer byNo ratings yet
- NCP - Impaired Gas Exchange (COPD)Document3 pagesNCP - Impaired Gas Exchange (COPD)Karen Joy ItoNo ratings yet
- RRLDocument3 pagesRRLKevin M. VillacorteNo ratings yet
- PoliomyelitisDocument4 pagesPoliomyelitisGerard Adad Misa100% (1)
- Decreased Cardiac OutputDocument5 pagesDecreased Cardiac Outputshuang81No ratings yet
- Coughs and Colds Nurse Management of Upper Respiratory Tract InfectionDocument3 pagesCoughs and Colds Nurse Management of Upper Respiratory Tract InfectionMichael Anthony ErmitaNo ratings yet
- Hypertension CASE REPORTDocument57 pagesHypertension CASE REPORTJulienne Sanchez-SalazarNo ratings yet
- Ineffective Tissue PerfusionDocument5 pagesIneffective Tissue PerfusionKryza Dale Bunado BaticanNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- 1st Clinical NCPDocument4 pages1st Clinical NCPjoidaNo ratings yet
- OXYTOCINDocument3 pagesOXYTOCINJaye Aprile Adrianne KuizonNo ratings yet
- DRUG-STUDY-FORMAT-Binangonan Lakeview 2ndDocument2 pagesDRUG-STUDY-FORMAT-Binangonan Lakeview 2ndDianne UlandayNo ratings yet
- 5TH NCPDocument5 pages5TH NCPjoidaNo ratings yet
- 4TH NCPDocument4 pages4TH NCPjoidaNo ratings yet
- PathophysioDocument2 pagesPathophysiojoidaNo ratings yet
- 6TH NCPDocument4 pages6TH NCPjoidaNo ratings yet
- 2nd Day ClinicalDocument2 pages2nd Day ClinicaljoidaNo ratings yet
- 2nd Clinical CaseDocument4 pages2nd Clinical CasejoidaNo ratings yet
- 2nd NCPDocument4 pages2nd NCPjoidaNo ratings yet
- 1st ReflectionDocument1 page1st ReflectionjoidaNo ratings yet
- 1st Cinical CaseDocument5 pages1st Cinical CasejoidaNo ratings yet
- 1st Clinical NCPDocument4 pages1st Clinical NCPjoidaNo ratings yet
- 1st Drug StudyDocument3 pages1st Drug StudyjoidaNo ratings yet
- 3rd - NCPDocument5 pages3rd - NCPjoidaNo ratings yet
- 3rd - Neurogenic ShockDocument7 pages3rd - Neurogenic ShockjoidaNo ratings yet
- 2nd - Pulmonary EmbolismDocument6 pages2nd - Pulmonary EmbolismjoidaNo ratings yet
- 1st - CVADocument6 pages1st - CVAjoidaNo ratings yet
- 2nd Summative Test Q1 GR 12Document2 pages2nd Summative Test Q1 GR 12Ardie DomingoNo ratings yet
- Early Identification and Remediation For Infants With Poor SuckDocument10 pagesEarly Identification and Remediation For Infants With Poor SuckMara CadinoiuNo ratings yet
- Pradik Pengelolaan NyeriDocument24 pagesPradik Pengelolaan NyeriAndi SetyawanNo ratings yet
- Tumores HepaticosDocument77 pagesTumores HepaticosAnita Villanueva ArandaNo ratings yet
- Chapter 005Document76 pagesChapter 005api-263755297100% (1)
- Leaf Litter 3.1Document64 pagesLeaf Litter 3.1Drosera Capensis CapensisNo ratings yet
- Veterinary MedicineDocument16 pagesVeterinary Medicineapi-359846566No ratings yet
- GI Endo Eval Exam IIDocument7 pagesGI Endo Eval Exam IICraig Jesse B. LardizabalNo ratings yet
- BMS533 Practical 1Document10 pagesBMS533 Practical 1NURUL AIHAN AHMAD HILMINo ratings yet
- Integumentary SystemDocument49 pagesIntegumentary SystemAte LizaNo ratings yet
- The Basics of VirusesDocument4 pagesThe Basics of VirusesSharolt SierraNo ratings yet
- Materi Digestive SystemDocument13 pagesMateri Digestive Systembetta putriNo ratings yet
- Pathophysiology: Schematic DiagramDocument4 pagesPathophysiology: Schematic DiagramTyron ChuaNo ratings yet
- Soumya S Nair Biodata 4-07Document24 pagesSoumya S Nair Biodata 4-07ElizabethNo ratings yet
- Bausch and Lomb Case StudyDocument19 pagesBausch and Lomb Case Studyranjeetkumar23100% (1)
- Classroom Set-Up Food Vaccine FrequencyDocument5 pagesClassroom Set-Up Food Vaccine FrequencyLuke Edward PanganibanNo ratings yet
- NCPDocument11 pagesNCPJaziel Remo100% (1)
- Indian National Biology Olympiad 2015Document50 pagesIndian National Biology Olympiad 2015Science Olympiad BlogNo ratings yet
- Advantage2 Unit2 1Document2 pagesAdvantage2 Unit2 1Patricia Fernández AbellánNo ratings yet
- RODAHL 2019 Be Fit For LifeDocument213 pagesRODAHL 2019 Be Fit For LifegonzalezalberteNo ratings yet
- Franco ProfileDocument46 pagesFranco ProfileSumit SharmaNo ratings yet
- Field Guide To Antibiotic StewardshipDocument30 pagesField Guide To Antibiotic StewardshipHosam GomaaNo ratings yet
- ThesisDocument18 pagesThesisArshNo ratings yet
- Condiments and SpicesDocument171 pagesCondiments and SpicesŞerban VeronicaNo ratings yet
- Guidelinesfordomestictravel (Airortrainorinter Statebustravel) PDFDocument1 pageGuidelinesfordomestictravel (Airortrainorinter Statebustravel) PDFBhai Amerik JiNo ratings yet
- Womens OrgasmsDocument30 pagesWomens OrgasmsMarkWoodxxxNo ratings yet
- MaretDocument132 pagesMarettipanoesaNo ratings yet