
Addressing The Forgotten Art of Fundoscopy ': Evaluation of A Novel Teaching Ophthalmoscope
Addressing The Forgotten Art of Fundoscopy ': Evaluation of A Novel Teaching Ophthalmoscope
You might also like
- PE11 - MELC 4 Module 4 - Week7 For Teacher PDFDocument24 pagesPE11 - MELC 4 Module 4 - Week7 For Teacher PDFRommel Cando80% (5)
- Free Preview - The Stall Slayer PDFDocument9 pagesFree Preview - The Stall Slayer PDFRohit RumadeNo ratings yet
- Smartphone Ophthalmoscope As A Tool in Teaching Direct Ophthalmoscopy: A Crossover Randomized Controlled TrialDocument9 pagesSmartphone Ophthalmoscope As A Tool in Teaching Direct Ophthalmoscopy: A Crossover Randomized Controlled TrialWalisson BarbosaNo ratings yet
- 16Document2 pages16Walisson BarbosaNo ratings yet
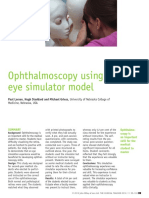
- Ophthalmoscopy Using An Eye Simulator Model: SimulationDocument5 pagesOphthalmoscopy Using An Eye Simulator Model: SimulationWalisson BarbosaNo ratings yet
- An Experimental Training Support Framework For Eye Fundus Examination Skill DevelopmentDocument13 pagesAn Experimental Training Support Framework For Eye Fundus Examination Skill DevelopmentWalisson BarbosaNo ratings yet
- Evaluation of An Online Peer Fundus Photograph Matching Program in Teaching Direct Ophthalmoscopy To Medical StudentsDocument6 pagesEvaluation of An Online Peer Fundus Photograph Matching Program in Teaching Direct Ophthalmoscopy To Medical StudentsWalisson BarbosaNo ratings yet
- Application of A 3d-Printed Eye Model For Teaching Direct Ophthalmoscopy To UndergraduatesDocument8 pagesApplication of A 3d-Printed Eye Model For Teaching Direct Ophthalmoscopy To UndergraduatesWalisson BarbosaNo ratings yet
- Prospective, Randomized Trial Comparing Simulator-Based Versus Traditional Teaching of Direct Ophthalmoscopy For Medical StudentsDocument10 pagesProspective, Randomized Trial Comparing Simulator-Based Versus Traditional Teaching of Direct Ophthalmoscopy For Medical StudentsWalisson 5No ratings yet
- Integrating Retinal Simulation With A Peer-Assessed Group OSCE Format To Teach Direct OphthalmosDocument6 pagesIntegrating Retinal Simulation With A Peer-Assessed Group OSCE Format To Teach Direct OphthalmosWalisson BarbosaNo ratings yet
- 4Document10 pages4Walisson 5No ratings yet
- Comparison of Smartphone Ophthalmoscopy Vs Conventional Direct Ophthalmoscopy As A Teaching Tool For Medical Students: The Cosmos StudyDocument11 pagesComparison of Smartphone Ophthalmoscopy Vs Conventional Direct Ophthalmoscopy As A Teaching Tool For Medical Students: The Cosmos StudyWalisson 5No ratings yet
- Etter To The Editor: Virtual Reality-Based Proficiency Test in Direct OphthalmosDocument2 pagesEtter To The Editor: Virtual Reality-Based Proficiency Test in Direct OphthalmosWalisson BarbosaNo ratings yet
- A Preliminary Usability Comparison of Augmented and Virtual Reality User Interactions For Direct OphthalmosDocument8 pagesA Preliminary Usability Comparison of Augmented and Virtual Reality User Interactions For Direct OphthalmosWalisson BarbosaNo ratings yet
- Teaching Ophthalmoscopy To Medical Students (The Totems Study)Document16 pagesTeaching Ophthalmoscopy To Medical Students (The Totems Study)Walisson BarbosaNo ratings yet
- Evaluating The Effectiveness of Small-Group Training in Teaching Medical Students Integral Clinical Eye Examination SkillsDocument8 pagesEvaluating The Effectiveness of Small-Group Training in Teaching Medical Students Integral Clinical Eye Examination SkillsWalisson 5No ratings yet
- The Effectiveness of Smartphone Ophthalmoscope Compared To Direct Ophthalmoscope As A Teaching ToolDocument13 pagesThe Effectiveness of Smartphone Ophthalmoscope Compared To Direct Ophthalmoscope As A Teaching ToolWalisson BarbosaNo ratings yet
- The Cycloplegic Autorefraction Related With Retinoscopy Patients (Article Review)Document6 pagesThe Cycloplegic Autorefraction Related With Retinoscopy Patients (Article Review)Central Asian StudiesNo ratings yet
- Effect of Repeated Low-Level Red-Light Therapy For Myopia Control in Children A Multicenter Randomized Controlled TrialDocument11 pagesEffect of Repeated Low-Level Red-Light Therapy For Myopia Control in Children A Multicenter Randomized Controlled TrialYekiita QuinteroNo ratings yet
- Teaching Smartphone Funduscopy With 20 Diopter Lens in Undergraduate Medical EducationDocument11 pagesTeaching Smartphone Funduscopy With 20 Diopter Lens in Undergraduate Medical EducationWalisson 5No ratings yet
- Comparison of Conventional and Wide Field Direct Ophthalmoscopy On Medical Students ' Self-Confidence For Fundus Examination: A 1-Year Follow-UpDocument9 pagesComparison of Conventional and Wide Field Direct Ophthalmoscopy On Medical Students ' Self-Confidence For Fundus Examination: A 1-Year Follow-UpWalisson BarbosaNo ratings yet
- Efficacy and Safety of A Soft Contact Lens To Control MyopiaprogressionDocument8 pagesEfficacy and Safety of A Soft Contact Lens To Control MyopiaprogressionAmandaNo ratings yet
- A Novel Approach To Teaching Fundoscopy Using A Virtual FormatDocument7 pagesA Novel Approach To Teaching Fundoscopy Using A Virtual FormatWalisson BarbosaNo ratings yet
- Use of A Fundus Photograph Matching Program in Imparting Pro Ficiency in OphthalmosDocument6 pagesUse of A Fundus Photograph Matching Program in Imparting Pro Ficiency in OphthalmosWalisson BarbosaNo ratings yet
- Perceived Usefulness and Ease of Use of Fundoscopy by Medical Students: A Randomised Crossover Trial of Six Technologies (eFOCUS 1)Document9 pagesPerceived Usefulness and Ease of Use of Fundoscopy by Medical Students: A Randomised Crossover Trial of Six Technologies (eFOCUS 1)Walisson BarbosaNo ratings yet
- Contact Lens ThesisDocument6 pagesContact Lens Thesisdnqj27m0100% (2)
- Training LabDocument1 pageTraining LabsightbdNo ratings yet
- Investigation of The Efficacy of An Online ToolDocument9 pagesInvestigation of The Efficacy of An Online ToolDani DuneNo ratings yet
- Objectively Measured Near Work, Outdoor Exposure and Myopia in ChildrenDocument6 pagesObjectively Measured Near Work, Outdoor Exposure and Myopia in ChildrenqisthiNo ratings yet
- Ophthalmoscopy Simulation Advances in Training and Practice For Medical Students and Young OphthalmologistsDocument6 pagesOphthalmoscopy Simulation Advances in Training and Practice For Medical Students and Young OphthalmologistsNour hane BiadNo ratings yet
- Eyesi Indirect BrochureDocument12 pagesEyesi Indirect BrochureHaag-Streit UK (HS-UK)No ratings yet
- Ocular Fundus Photography As An Educational Tool: Ddmackay@iupui - EduDocument33 pagesOcular Fundus Photography As An Educational Tool: Ddmackay@iupui - EduWalisson BarbosaNo ratings yet
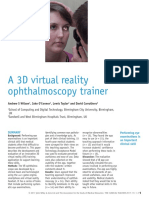
- A 3D Virtual Reality Ophthalmoscopy Trainer: Original ArticleDocument5 pagesA 3D Virtual Reality Ophthalmoscopy Trainer: Original ArticleWalisson BarbosaNo ratings yet
- Eye 2011154 ADocument7 pagesEye 2011154 AAmba PutraNo ratings yet
- Introduction and Objectives: Ophthalmoscopy Is A CoreDocument6 pagesIntroduction and Objectives: Ophthalmoscopy Is A CoreWalisson BarbosaNo ratings yet
- Done 3Document45 pagesDone 3CHIMA ONWUKA MONGNo ratings yet
- Knowledge, Usage and Barriers Associated With Contact Lens Wear in GhanaDocument6 pagesKnowledge, Usage and Barriers Associated With Contact Lens Wear in Ghanagrace odeyNo ratings yet
- A Reliable and Valid Questionnaire Was Developed To Measure Computer Vision Syndrome at The WorkplaceDocument13 pagesA Reliable and Valid Questionnaire Was Developed To Measure Computer Vision Syndrome at The WorkplacechandradwtrNo ratings yet
- Contact Lenses Vs Spectacles in Myopes: Is There Any Difference in Accommodative and Binocular Function?Document12 pagesContact Lenses Vs Spectacles in Myopes: Is There Any Difference in Accommodative and Binocular Function?mau tauNo ratings yet
- Precision and Agreement of Corneal Power Measurements Obtained Using A New Corneal Topographer OphthatopDocument16 pagesPrecision and Agreement of Corneal Power Measurements Obtained Using A New Corneal Topographer OphthatopWaleed Ah-DhaifiNo ratings yet
- Real-Time Teleophthalmology Versus Face-To-Face Consultation: A Systematic ReviewDocument10 pagesReal-Time Teleophthalmology Versus Face-To-Face Consultation: A Systematic ReviewJatinderBaliNo ratings yet
- Alamanos 2016Document12 pagesAlamanos 2016dana40018256No ratings yet
- EMP2 3 E12630Document25 pagesEMP2 3 E12630Briando Stevano LinelejanNo ratings yet
- Prospective Evaluation of Medical Student Accuracy Conducting Direct Ophthalmoscopy With An Unmodified Iphone XDocument8 pagesProspective Evaluation of Medical Student Accuracy Conducting Direct Ophthalmoscopy With An Unmodified Iphone XWalisson BarbosaNo ratings yet
- Resource_7_-_PPA2023MLT5473_220521_MF_Chair_Time_JJI_version_final_Updated_1Document2 pagesResource_7_-_PPA2023MLT5473_220521_MF_Chair_Time_JJI_version_final_Updated_1maritzaNo ratings yet
- Agreement and repeatability of scotopic pupil size measurement with the 2WIN-S portable refractor in Chinese adultsDocument8 pagesAgreement and repeatability of scotopic pupil size measurement with the 2WIN-S portable refractor in Chinese adultsreshma eldhoNo ratings yet
- High Myopiaypartial Reduction Ortho-K: A 2-Year Randomized StudyDocument10 pagesHigh Myopiaypartial Reduction Ortho-K: A 2-Year Randomized StudykarakuraNo ratings yet
- Video Interpretation and Diagnosis of Pediatric Amblyopia and Eye DiseasseDocument7 pagesVideo Interpretation and Diagnosis of Pediatric Amblyopia and Eye DiseasseDinda Ajeng AninditaNo ratings yet
- Direct Ophthalmoscopy On YouTube Analysis of Instructional YouTube Videos Content and Approach To VisualizationDocument8 pagesDirect Ophthalmoscopy On YouTube Analysis of Instructional YouTube Videos Content and Approach To VisualizationVlarah Alondra LiponNo ratings yet
- Sankaridurg 2023Document26 pagesSankaridurg 2023youthcp93No ratings yet
- OSCE Scope of The OSCE in The Assessment of ClinicDocument5 pagesOSCE Scope of The OSCE in The Assessment of Clinicdruzair007No ratings yet
- Eyesi Direct BrochureDocument12 pagesEyesi Direct BrochureHaag-Streit UK (HS-UK)No ratings yet
- E001035 FullDocument6 pagesE001035 FullRannyNo ratings yet
- Ophthalmic and Physiological Optics Volume 36 Issue 2 2016 (Doi 10.1111/opo.12275) Tauste, Ana Ronda, Elena Molina, María-José Seguí, Mar - Effect of Contact Lens Use On Computer Vision SyndromeDocument8 pagesOphthalmic and Physiological Optics Volume 36 Issue 2 2016 (Doi 10.1111/opo.12275) Tauste, Ana Ronda, Elena Molina, María-José Seguí, Mar - Effect of Contact Lens Use On Computer Vision SyndromeAdhe WagiNo ratings yet
- Comparison of Vision-Related Quality of Life Between Wearing Orthokeratology Lenses and Spectacles in Myopic Children LDocument5 pagesComparison of Vision-Related Quality of Life Between Wearing Orthokeratology Lenses and Spectacles in Myopic Children Lกนกกานต์ ธาดาธัญลักษณ์No ratings yet
- A Comparison of The Plusoptix S09 With An AutorefrDocument4 pagesA Comparison of The Plusoptix S09 With An Autorefrعباس مطهر الماخذيNo ratings yet
- EAOO Abstracts Dublin 22Document40 pagesEAOO Abstracts Dublin 22Cristina ÁlvarezNo ratings yet
- 1 s2.0 S002248042200453X MainDocument15 pages1 s2.0 S002248042200453X MainVikas KumarNo ratings yet
- Current Advances in Ophthalmic TechnologyFrom EverandCurrent Advances in Ophthalmic TechnologyParul IchhpujaniNo ratings yet
- OptometryDocument8 pagesOptometryasad aliNo ratings yet
- Methods For Assessing Corneal Opacity: Seminars in OphthalmologyDocument7 pagesMethods For Assessing Corneal Opacity: Seminars in OphthalmologyGermán PérezNo ratings yet
- Retinal Prosthesis: A Clinical Guide to Successful ImplementationFrom EverandRetinal Prosthesis: A Clinical Guide to Successful ImplementationMark S. HumayunNo ratings yet
- Comparison of Smartphone Ophthalmoscopy Vs Conventional Direct Ophthalmoscopy As A Teaching Tool For Medical Students: The Cosmos StudyDocument11 pagesComparison of Smartphone Ophthalmoscopy Vs Conventional Direct Ophthalmoscopy As A Teaching Tool For Medical Students: The Cosmos StudyWalisson 5No ratings yet
- Teaching Smartphone Funduscopy With 20 Diopter Lens in Undergraduate Medical EducationDocument11 pagesTeaching Smartphone Funduscopy With 20 Diopter Lens in Undergraduate Medical EducationWalisson 5No ratings yet
- Evaluating The Effectiveness of Small-Group Training in Teaching Medical Students Integral Clinical Eye Examination SkillsDocument8 pagesEvaluating The Effectiveness of Small-Group Training in Teaching Medical Students Integral Clinical Eye Examination SkillsWalisson 5No ratings yet
- 4Document10 pages4Walisson 5No ratings yet
- Prospective, Randomized Trial Comparing Simulator-Based Versus Traditional Teaching of Direct Ophthalmoscopy For Medical StudentsDocument10 pagesProspective, Randomized Trial Comparing Simulator-Based Versus Traditional Teaching of Direct Ophthalmoscopy For Medical StudentsWalisson 5No ratings yet
- Flexible E-Learning Video Approach To Improve Fundus Examination Skills For Medical Students: A Mixed-Methods StudyDocument9 pagesFlexible E-Learning Video Approach To Improve Fundus Examination Skills For Medical Students: A Mixed-Methods StudyWalisson 5No ratings yet
- Analisis Penerapan Metode Activity Based Costing (ABC) Dalam Menentukan Tarif Jasa Rawat Inap Di RSUD Kota PrabumulihDocument12 pagesAnalisis Penerapan Metode Activity Based Costing (ABC) Dalam Menentukan Tarif Jasa Rawat Inap Di RSUD Kota PrabumulihAffira AfriNo ratings yet
- Ultrarunning MagDocument60 pagesUltrarunning MagLynseyNo ratings yet
- Syngoplaza ProchureDocument49 pagesSyngoplaza ProchurehajerbenNo ratings yet
- 10besar Kode PenyakitDocument5 pages10besar Kode PenyakitDEWINo ratings yet
- SynopsisDocument8 pagesSynopsisarunNo ratings yet
- Activity #1: ETHICAL CASE Name: Date: Year/Section: Grade/scoreDocument4 pagesActivity #1: ETHICAL CASE Name: Date: Year/Section: Grade/scoreJovie FabrosNo ratings yet
- Determination 446 Pesticides Residue by GC Ms and LC MsDocument32 pagesDetermination 446 Pesticides Residue by GC Ms and LC MsMohammed ELAbadsaNo ratings yet
- Firefly Prime Mobile AppDocument7 pagesFirefly Prime Mobile Appmukh bhaNo ratings yet
- The Manual of Ethiopian Medical History - People To People PDFDocument60 pagesThe Manual of Ethiopian Medical History - People To People PDFShiferaw Biru100% (1)
- Impact of Covid19 On The Indian Stock MarketDocument6 pagesImpact of Covid19 On The Indian Stock MarketB31 Viraj PatilNo ratings yet
- Hormones ImbalanceDocument3 pagesHormones ImbalanceKiran KhanNo ratings yet
- November 2009 Final EditionDocument45 pagesNovember 2009 Final Editionaajo136No ratings yet
- Soal D3 Bidan HermanDocument2 pagesSoal D3 Bidan HermanMidwifeDeviFadhaNo ratings yet
- PHENYLKETONURIADocument3 pagesPHENYLKETONURIAMiwa IshiiNo ratings yet
- "After All, There Is Nothing As Interesting As People, and One Can Never Study Them Enough" Vincent Van GoghDocument38 pages"After All, There Is Nothing As Interesting As People, and One Can Never Study Them Enough" Vincent Van GoghAnonymous 1gH7ra9ANo ratings yet
- A Review On Various Uses of N-Acetyl CysteineDocument7 pagesA Review On Various Uses of N-Acetyl CysteineMudrikaNo ratings yet
- Stresses and Challenges For New Graduates in HospitalsDocument6 pagesStresses and Challenges For New Graduates in HospitalskitsilNo ratings yet
- Maternity Nursing ReviewDocument37 pagesMaternity Nursing Reviewshenric16No ratings yet
- Justin PT NanguneriDocument53 pagesJustin PT NanguneriJustin Xaviour dhasNo ratings yet
- Bilal Ahmad Khan CVDocument2 pagesBilal Ahmad Khan CVfr.faisal8265No ratings yet
- One Minute Push Up TestDocument5 pagesOne Minute Push Up Testayieeeee03No ratings yet
- Mark The Letter A, B, C, or D On Your Answer Sheet To Indicate The Correct Answer To Each of The Following QuestionsDocument5 pagesMark The Letter A, B, C, or D On Your Answer Sheet To Indicate The Correct Answer To Each of The Following QuestionsVăn phú NguyễnNo ratings yet
- Data SecuityDocument15 pagesData Secuitybikram160106No ratings yet
- IELTS Cause-Problem and Effect-Solution Model EssayDocument17 pagesIELTS Cause-Problem and Effect-Solution Model EssaySayaf RashadNo ratings yet
- Community Resilience: Integrating Hazard Management and Community EngagementDocument21 pagesCommunity Resilience: Integrating Hazard Management and Community EngagementJavier Gonzales IwanciwNo ratings yet
- How To Prevent BullyingDocument4 pagesHow To Prevent BullyingLiezel-jheng Apostol LozadaNo ratings yet
- Ayurvedic Medicine For Bhutansha RasaDocument6 pagesAyurvedic Medicine For Bhutansha RasaKolluri RajeshNo ratings yet
- Medical Condition Report Free PDF TemplateDocument2 pagesMedical Condition Report Free PDF Templateapi-340236228No ratings yet

























































































Download as pdf or txt
You might also like
- PE11 - MELC 4 Module 4 - Week7 For Teacher PDFDocument24 pagesPE11 - MELC 4 Module 4 - Week7 For Teacher PDFRommel Cando80% (5)
- Free Preview - The Stall Slayer PDFDocument9 pagesFree Preview - The Stall Slayer PDFRohit RumadeNo ratings yet
- Smartphone Ophthalmoscope As A Tool in Teaching Direct Ophthalmoscopy: A Crossover Randomized Controlled TrialDocument9 pagesSmartphone Ophthalmoscope As A Tool in Teaching Direct Ophthalmoscopy: A Crossover Randomized Controlled TrialWalisson BarbosaNo ratings yet
- 16Document2 pages16Walisson BarbosaNo ratings yet
- Ophthalmoscopy Using An Eye Simulator Model: SimulationDocument5 pagesOphthalmoscopy Using An Eye Simulator Model: SimulationWalisson BarbosaNo ratings yet
- An Experimental Training Support Framework For Eye Fundus Examination Skill DevelopmentDocument13 pagesAn Experimental Training Support Framework For Eye Fundus Examination Skill DevelopmentWalisson BarbosaNo ratings yet
- Evaluation of An Online Peer Fundus Photograph Matching Program in Teaching Direct Ophthalmoscopy To Medical StudentsDocument6 pagesEvaluation of An Online Peer Fundus Photograph Matching Program in Teaching Direct Ophthalmoscopy To Medical StudentsWalisson BarbosaNo ratings yet
- Application of A 3d-Printed Eye Model For Teaching Direct Ophthalmoscopy To UndergraduatesDocument8 pagesApplication of A 3d-Printed Eye Model For Teaching Direct Ophthalmoscopy To UndergraduatesWalisson BarbosaNo ratings yet
- Prospective, Randomized Trial Comparing Simulator-Based Versus Traditional Teaching of Direct Ophthalmoscopy For Medical StudentsDocument10 pagesProspective, Randomized Trial Comparing Simulator-Based Versus Traditional Teaching of Direct Ophthalmoscopy For Medical StudentsWalisson 5No ratings yet
- Integrating Retinal Simulation With A Peer-Assessed Group OSCE Format To Teach Direct OphthalmosDocument6 pagesIntegrating Retinal Simulation With A Peer-Assessed Group OSCE Format To Teach Direct OphthalmosWalisson BarbosaNo ratings yet
- 4Document10 pages4Walisson 5No ratings yet
- Comparison of Smartphone Ophthalmoscopy Vs Conventional Direct Ophthalmoscopy As A Teaching Tool For Medical Students: The Cosmos StudyDocument11 pagesComparison of Smartphone Ophthalmoscopy Vs Conventional Direct Ophthalmoscopy As A Teaching Tool For Medical Students: The Cosmos StudyWalisson 5No ratings yet
- Etter To The Editor: Virtual Reality-Based Proficiency Test in Direct OphthalmosDocument2 pagesEtter To The Editor: Virtual Reality-Based Proficiency Test in Direct OphthalmosWalisson BarbosaNo ratings yet
- A Preliminary Usability Comparison of Augmented and Virtual Reality User Interactions For Direct OphthalmosDocument8 pagesA Preliminary Usability Comparison of Augmented and Virtual Reality User Interactions For Direct OphthalmosWalisson BarbosaNo ratings yet
- Teaching Ophthalmoscopy To Medical Students (The Totems Study)Document16 pagesTeaching Ophthalmoscopy To Medical Students (The Totems Study)Walisson BarbosaNo ratings yet
- Evaluating The Effectiveness of Small-Group Training in Teaching Medical Students Integral Clinical Eye Examination SkillsDocument8 pagesEvaluating The Effectiveness of Small-Group Training in Teaching Medical Students Integral Clinical Eye Examination SkillsWalisson 5No ratings yet
- The Effectiveness of Smartphone Ophthalmoscope Compared To Direct Ophthalmoscope As A Teaching ToolDocument13 pagesThe Effectiveness of Smartphone Ophthalmoscope Compared To Direct Ophthalmoscope As A Teaching ToolWalisson BarbosaNo ratings yet
- The Cycloplegic Autorefraction Related With Retinoscopy Patients (Article Review)Document6 pagesThe Cycloplegic Autorefraction Related With Retinoscopy Patients (Article Review)Central Asian StudiesNo ratings yet
- Effect of Repeated Low-Level Red-Light Therapy For Myopia Control in Children A Multicenter Randomized Controlled TrialDocument11 pagesEffect of Repeated Low-Level Red-Light Therapy For Myopia Control in Children A Multicenter Randomized Controlled TrialYekiita QuinteroNo ratings yet
- Teaching Smartphone Funduscopy With 20 Diopter Lens in Undergraduate Medical EducationDocument11 pagesTeaching Smartphone Funduscopy With 20 Diopter Lens in Undergraduate Medical EducationWalisson 5No ratings yet
- Comparison of Conventional and Wide Field Direct Ophthalmoscopy On Medical Students ' Self-Confidence For Fundus Examination: A 1-Year Follow-UpDocument9 pagesComparison of Conventional and Wide Field Direct Ophthalmoscopy On Medical Students ' Self-Confidence For Fundus Examination: A 1-Year Follow-UpWalisson BarbosaNo ratings yet
- Efficacy and Safety of A Soft Contact Lens To Control MyopiaprogressionDocument8 pagesEfficacy and Safety of A Soft Contact Lens To Control MyopiaprogressionAmandaNo ratings yet
- A Novel Approach To Teaching Fundoscopy Using A Virtual FormatDocument7 pagesA Novel Approach To Teaching Fundoscopy Using A Virtual FormatWalisson BarbosaNo ratings yet
- Use of A Fundus Photograph Matching Program in Imparting Pro Ficiency in OphthalmosDocument6 pagesUse of A Fundus Photograph Matching Program in Imparting Pro Ficiency in OphthalmosWalisson BarbosaNo ratings yet
- Perceived Usefulness and Ease of Use of Fundoscopy by Medical Students: A Randomised Crossover Trial of Six Technologies (eFOCUS 1)Document9 pagesPerceived Usefulness and Ease of Use of Fundoscopy by Medical Students: A Randomised Crossover Trial of Six Technologies (eFOCUS 1)Walisson BarbosaNo ratings yet
- Contact Lens ThesisDocument6 pagesContact Lens Thesisdnqj27m0100% (2)
- Training LabDocument1 pageTraining LabsightbdNo ratings yet
- Investigation of The Efficacy of An Online ToolDocument9 pagesInvestigation of The Efficacy of An Online ToolDani DuneNo ratings yet
- Objectively Measured Near Work, Outdoor Exposure and Myopia in ChildrenDocument6 pagesObjectively Measured Near Work, Outdoor Exposure and Myopia in ChildrenqisthiNo ratings yet
- Ophthalmoscopy Simulation Advances in Training and Practice For Medical Students and Young OphthalmologistsDocument6 pagesOphthalmoscopy Simulation Advances in Training and Practice For Medical Students and Young OphthalmologistsNour hane BiadNo ratings yet
- Eyesi Indirect BrochureDocument12 pagesEyesi Indirect BrochureHaag-Streit UK (HS-UK)No ratings yet
- Ocular Fundus Photography As An Educational Tool: Ddmackay@iupui - EduDocument33 pagesOcular Fundus Photography As An Educational Tool: Ddmackay@iupui - EduWalisson BarbosaNo ratings yet
- A 3D Virtual Reality Ophthalmoscopy Trainer: Original ArticleDocument5 pagesA 3D Virtual Reality Ophthalmoscopy Trainer: Original ArticleWalisson BarbosaNo ratings yet
- Eye 2011154 ADocument7 pagesEye 2011154 AAmba PutraNo ratings yet
- Introduction and Objectives: Ophthalmoscopy Is A CoreDocument6 pagesIntroduction and Objectives: Ophthalmoscopy Is A CoreWalisson BarbosaNo ratings yet
- Done 3Document45 pagesDone 3CHIMA ONWUKA MONGNo ratings yet
- Knowledge, Usage and Barriers Associated With Contact Lens Wear in GhanaDocument6 pagesKnowledge, Usage and Barriers Associated With Contact Lens Wear in Ghanagrace odeyNo ratings yet
- A Reliable and Valid Questionnaire Was Developed To Measure Computer Vision Syndrome at The WorkplaceDocument13 pagesA Reliable and Valid Questionnaire Was Developed To Measure Computer Vision Syndrome at The WorkplacechandradwtrNo ratings yet
- Contact Lenses Vs Spectacles in Myopes: Is There Any Difference in Accommodative and Binocular Function?Document12 pagesContact Lenses Vs Spectacles in Myopes: Is There Any Difference in Accommodative and Binocular Function?mau tauNo ratings yet
- Precision and Agreement of Corneal Power Measurements Obtained Using A New Corneal Topographer OphthatopDocument16 pagesPrecision and Agreement of Corneal Power Measurements Obtained Using A New Corneal Topographer OphthatopWaleed Ah-DhaifiNo ratings yet
- Real-Time Teleophthalmology Versus Face-To-Face Consultation: A Systematic ReviewDocument10 pagesReal-Time Teleophthalmology Versus Face-To-Face Consultation: A Systematic ReviewJatinderBaliNo ratings yet
- Alamanos 2016Document12 pagesAlamanos 2016dana40018256No ratings yet
- EMP2 3 E12630Document25 pagesEMP2 3 E12630Briando Stevano LinelejanNo ratings yet
- Prospective Evaluation of Medical Student Accuracy Conducting Direct Ophthalmoscopy With An Unmodified Iphone XDocument8 pagesProspective Evaluation of Medical Student Accuracy Conducting Direct Ophthalmoscopy With An Unmodified Iphone XWalisson BarbosaNo ratings yet
- Resource_7_-_PPA2023MLT5473_220521_MF_Chair_Time_JJI_version_final_Updated_1Document2 pagesResource_7_-_PPA2023MLT5473_220521_MF_Chair_Time_JJI_version_final_Updated_1maritzaNo ratings yet
- Agreement and repeatability of scotopic pupil size measurement with the 2WIN-S portable refractor in Chinese adultsDocument8 pagesAgreement and repeatability of scotopic pupil size measurement with the 2WIN-S portable refractor in Chinese adultsreshma eldhoNo ratings yet
- High Myopiaypartial Reduction Ortho-K: A 2-Year Randomized StudyDocument10 pagesHigh Myopiaypartial Reduction Ortho-K: A 2-Year Randomized StudykarakuraNo ratings yet
- Video Interpretation and Diagnosis of Pediatric Amblyopia and Eye DiseasseDocument7 pagesVideo Interpretation and Diagnosis of Pediatric Amblyopia and Eye DiseasseDinda Ajeng AninditaNo ratings yet
- Direct Ophthalmoscopy On YouTube Analysis of Instructional YouTube Videos Content and Approach To VisualizationDocument8 pagesDirect Ophthalmoscopy On YouTube Analysis of Instructional YouTube Videos Content and Approach To VisualizationVlarah Alondra LiponNo ratings yet
- Sankaridurg 2023Document26 pagesSankaridurg 2023youthcp93No ratings yet
- OSCE Scope of The OSCE in The Assessment of ClinicDocument5 pagesOSCE Scope of The OSCE in The Assessment of Clinicdruzair007No ratings yet
- Eyesi Direct BrochureDocument12 pagesEyesi Direct BrochureHaag-Streit UK (HS-UK)No ratings yet
- E001035 FullDocument6 pagesE001035 FullRannyNo ratings yet
- Ophthalmic and Physiological Optics Volume 36 Issue 2 2016 (Doi 10.1111/opo.12275) Tauste, Ana Ronda, Elena Molina, María-José Seguí, Mar - Effect of Contact Lens Use On Computer Vision SyndromeDocument8 pagesOphthalmic and Physiological Optics Volume 36 Issue 2 2016 (Doi 10.1111/opo.12275) Tauste, Ana Ronda, Elena Molina, María-José Seguí, Mar - Effect of Contact Lens Use On Computer Vision SyndromeAdhe WagiNo ratings yet
- Comparison of Vision-Related Quality of Life Between Wearing Orthokeratology Lenses and Spectacles in Myopic Children LDocument5 pagesComparison of Vision-Related Quality of Life Between Wearing Orthokeratology Lenses and Spectacles in Myopic Children Lกนกกานต์ ธาดาธัญลักษณ์No ratings yet
- A Comparison of The Plusoptix S09 With An AutorefrDocument4 pagesA Comparison of The Plusoptix S09 With An Autorefrعباس مطهر الماخذيNo ratings yet
- EAOO Abstracts Dublin 22Document40 pagesEAOO Abstracts Dublin 22Cristina ÁlvarezNo ratings yet
- 1 s2.0 S002248042200453X MainDocument15 pages1 s2.0 S002248042200453X MainVikas KumarNo ratings yet
- Current Advances in Ophthalmic TechnologyFrom EverandCurrent Advances in Ophthalmic TechnologyParul IchhpujaniNo ratings yet
- OptometryDocument8 pagesOptometryasad aliNo ratings yet
- Methods For Assessing Corneal Opacity: Seminars in OphthalmologyDocument7 pagesMethods For Assessing Corneal Opacity: Seminars in OphthalmologyGermán PérezNo ratings yet
- Retinal Prosthesis: A Clinical Guide to Successful ImplementationFrom EverandRetinal Prosthesis: A Clinical Guide to Successful ImplementationMark S. HumayunNo ratings yet
- Comparison of Smartphone Ophthalmoscopy Vs Conventional Direct Ophthalmoscopy As A Teaching Tool For Medical Students: The Cosmos StudyDocument11 pagesComparison of Smartphone Ophthalmoscopy Vs Conventional Direct Ophthalmoscopy As A Teaching Tool For Medical Students: The Cosmos StudyWalisson 5No ratings yet
- Teaching Smartphone Funduscopy With 20 Diopter Lens in Undergraduate Medical EducationDocument11 pagesTeaching Smartphone Funduscopy With 20 Diopter Lens in Undergraduate Medical EducationWalisson 5No ratings yet
- Evaluating The Effectiveness of Small-Group Training in Teaching Medical Students Integral Clinical Eye Examination SkillsDocument8 pagesEvaluating The Effectiveness of Small-Group Training in Teaching Medical Students Integral Clinical Eye Examination SkillsWalisson 5No ratings yet
- 4Document10 pages4Walisson 5No ratings yet
- Prospective, Randomized Trial Comparing Simulator-Based Versus Traditional Teaching of Direct Ophthalmoscopy For Medical StudentsDocument10 pagesProspective, Randomized Trial Comparing Simulator-Based Versus Traditional Teaching of Direct Ophthalmoscopy For Medical StudentsWalisson 5No ratings yet
- Flexible E-Learning Video Approach To Improve Fundus Examination Skills For Medical Students: A Mixed-Methods StudyDocument9 pagesFlexible E-Learning Video Approach To Improve Fundus Examination Skills For Medical Students: A Mixed-Methods StudyWalisson 5No ratings yet
- Analisis Penerapan Metode Activity Based Costing (ABC) Dalam Menentukan Tarif Jasa Rawat Inap Di RSUD Kota PrabumulihDocument12 pagesAnalisis Penerapan Metode Activity Based Costing (ABC) Dalam Menentukan Tarif Jasa Rawat Inap Di RSUD Kota PrabumulihAffira AfriNo ratings yet
- Ultrarunning MagDocument60 pagesUltrarunning MagLynseyNo ratings yet
- Syngoplaza ProchureDocument49 pagesSyngoplaza ProchurehajerbenNo ratings yet
- 10besar Kode PenyakitDocument5 pages10besar Kode PenyakitDEWINo ratings yet
- SynopsisDocument8 pagesSynopsisarunNo ratings yet
- Activity #1: ETHICAL CASE Name: Date: Year/Section: Grade/scoreDocument4 pagesActivity #1: ETHICAL CASE Name: Date: Year/Section: Grade/scoreJovie FabrosNo ratings yet
- Determination 446 Pesticides Residue by GC Ms and LC MsDocument32 pagesDetermination 446 Pesticides Residue by GC Ms and LC MsMohammed ELAbadsaNo ratings yet
- Firefly Prime Mobile AppDocument7 pagesFirefly Prime Mobile Appmukh bhaNo ratings yet
- The Manual of Ethiopian Medical History - People To People PDFDocument60 pagesThe Manual of Ethiopian Medical History - People To People PDFShiferaw Biru100% (1)
- Impact of Covid19 On The Indian Stock MarketDocument6 pagesImpact of Covid19 On The Indian Stock MarketB31 Viraj PatilNo ratings yet
- Hormones ImbalanceDocument3 pagesHormones ImbalanceKiran KhanNo ratings yet
- November 2009 Final EditionDocument45 pagesNovember 2009 Final Editionaajo136No ratings yet
- Soal D3 Bidan HermanDocument2 pagesSoal D3 Bidan HermanMidwifeDeviFadhaNo ratings yet
- PHENYLKETONURIADocument3 pagesPHENYLKETONURIAMiwa IshiiNo ratings yet
- "After All, There Is Nothing As Interesting As People, and One Can Never Study Them Enough" Vincent Van GoghDocument38 pages"After All, There Is Nothing As Interesting As People, and One Can Never Study Them Enough" Vincent Van GoghAnonymous 1gH7ra9ANo ratings yet
- A Review On Various Uses of N-Acetyl CysteineDocument7 pagesA Review On Various Uses of N-Acetyl CysteineMudrikaNo ratings yet
- Stresses and Challenges For New Graduates in HospitalsDocument6 pagesStresses and Challenges For New Graduates in HospitalskitsilNo ratings yet
- Maternity Nursing ReviewDocument37 pagesMaternity Nursing Reviewshenric16No ratings yet
- Justin PT NanguneriDocument53 pagesJustin PT NanguneriJustin Xaviour dhasNo ratings yet
- Bilal Ahmad Khan CVDocument2 pagesBilal Ahmad Khan CVfr.faisal8265No ratings yet
- One Minute Push Up TestDocument5 pagesOne Minute Push Up Testayieeeee03No ratings yet
- Mark The Letter A, B, C, or D On Your Answer Sheet To Indicate The Correct Answer To Each of The Following QuestionsDocument5 pagesMark The Letter A, B, C, or D On Your Answer Sheet To Indicate The Correct Answer To Each of The Following QuestionsVăn phú NguyễnNo ratings yet
- Data SecuityDocument15 pagesData Secuitybikram160106No ratings yet
- IELTS Cause-Problem and Effect-Solution Model EssayDocument17 pagesIELTS Cause-Problem and Effect-Solution Model EssaySayaf RashadNo ratings yet
- Community Resilience: Integrating Hazard Management and Community EngagementDocument21 pagesCommunity Resilience: Integrating Hazard Management and Community EngagementJavier Gonzales IwanciwNo ratings yet
- How To Prevent BullyingDocument4 pagesHow To Prevent BullyingLiezel-jheng Apostol LozadaNo ratings yet
- Ayurvedic Medicine For Bhutansha RasaDocument6 pagesAyurvedic Medicine For Bhutansha RasaKolluri RajeshNo ratings yet
- Medical Condition Report Free PDF TemplateDocument2 pagesMedical Condition Report Free PDF Templateapi-340236228No ratings yet