Download as docx, pdf, or txt
You might also like
- This Study Resource Was: Urinary Elimination Case StudyDocument5 pagesThis Study Resource Was: Urinary Elimination Case StudyAnna Marie Oligo OcheaNo ratings yet
- Nursing Care Plan For Upper Resrpiratory Tract InfectionDocument2 pagesNursing Care Plan For Upper Resrpiratory Tract Infectionmariejo87% (31)
- Valdez Reflective-Questions PDFDocument3 pagesValdez Reflective-Questions PDFDexel Lorren ValdezNo ratings yet
- Medication - ALT-Template - Albuterol Sulfate PDFDocument1 pageMedication - ALT-Template - Albuterol Sulfate PDFNancyAmissah100% (1)
- Laryngeal MassDocument36 pagesLaryngeal MassJayson de GuzmanNo ratings yet
- 2Document4 pages2Emmyr JohnNo ratings yet
- Physiological Changes in Elderly RespiDocument23 pagesPhysiological Changes in Elderly RespiIrwan M. IskoberNo ratings yet
- Propanolol and Spironolactone Drug StudyDocument2 pagesPropanolol and Spironolactone Drug StudyLisette Castillo91% (11)
- Psychiatry Rating ScalesDocument4 pagesPsychiatry Rating ScalesRafaila Tony100% (1)
- CDC Covering The Basics Rhetorical Analysis EssayDocument4 pagesCDC Covering The Basics Rhetorical Analysis EssayAllechia JonesNo ratings yet
- Nursing Diagnosis (1) (1) .Finalgid NiyaDocument30 pagesNursing Diagnosis (1) (1) .Finalgid NiyaReadcast EFNo ratings yet
- Case Study 2 NCPDocument1 pageCase Study 2 NCPJayson SamonteNo ratings yet
- HypertensionDocument3 pagesHypertensionAgnes Marie RendonNo ratings yet
- Plan of Care For:: Nursing Diagnosis: Excess Fluid VolumeDocument3 pagesPlan of Care For:: Nursing Diagnosis: Excess Fluid VolumeKenji CadizNo ratings yet
- Pex 03 07Document6 pagesPex 03 07aexillis100% (3)
- 4.3 Respi. Percussion VibrationDocument8 pages4.3 Respi. Percussion VibrationRiza Angela BarazanNo ratings yet
- Practice Summary Paper For PortfolioDocument9 pagesPractice Summary Paper For Portfolioapi-290938460No ratings yet
- Nursing Care PlanDocument2 pagesNursing Care Planusama_salaymehNo ratings yet
- Caring For Children Receiving Chemotherapy, Antimicrobial Therapy and Long-Term Insulin TherapyDocument34 pagesCaring For Children Receiving Chemotherapy, Antimicrobial Therapy and Long-Term Insulin TherapyRubinaNo ratings yet
- Concept Map 2Document1 pageConcept Map 2lanrevoiceNo ratings yet
- Dhan Chan NCPDocument3 pagesDhan Chan NCPDhaneanne Marie ChanNo ratings yet
- Nursing Interventions CHFDocument3 pagesNursing Interventions CHFbanyenye25100% (1)
- GRP 3 2 Renal Nephrectomy NCPDocument6 pagesGRP 3 2 Renal Nephrectomy NCPPam RomeroNo ratings yet
- NGT Procedure With RationaleDocument4 pagesNGT Procedure With Rationaleyuuki konnoNo ratings yet
- Drug Dosage, Frequency, Route Indication Action Drug Interaction Contraindication Adverse Effects Nursing Consideration Generic Name: Brand NameDocument3 pagesDrug Dosage, Frequency, Route Indication Action Drug Interaction Contraindication Adverse Effects Nursing Consideration Generic Name: Brand NameRobert Martin Rivera PuertaNo ratings yet
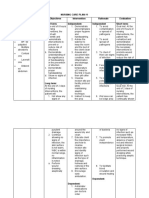
- Nursing Care Plan #1 Cues Nursing Diagnosis Objectives Intervention Rationale Evaluation Subjective: Short Term: Independent: Independent Short TermDocument5 pagesNursing Care Plan #1 Cues Nursing Diagnosis Objectives Intervention Rationale Evaluation Subjective: Short Term: Independent: Independent Short TermAlmer OstreaNo ratings yet
- University of Luzon College of Nursing Ns-Ii2 P Oxygenation ProblemsDocument10 pagesUniversity of Luzon College of Nursing Ns-Ii2 P Oxygenation ProblemsAhmad BaolayyanNo ratings yet
- The Process of OxygenationDocument7 pagesThe Process of OxygenationMich CercadoNo ratings yet
- Anes Drugs TableDocument20 pagesAnes Drugs TableKathleen Grace ManiagoNo ratings yet
- Appendicitis - NCPDocument5 pagesAppendicitis - NCPEarl Joseph Deza100% (1)
- Activity Intolerance Care Plan For CFDocument8 pagesActivity Intolerance Care Plan For CFapi-314197645No ratings yet
- All The Questions in The Quiz Along With Their Answers Are Shown BelowDocument7 pagesAll The Questions in The Quiz Along With Their Answers Are Shown BelowArlene FerrerNo ratings yet
- MCN Exam 2 Study Guide - CompleteDocument87 pagesMCN Exam 2 Study Guide - CompleteColin MacKenzie100% (1)
- Impaired SwallowingDocument2 pagesImpaired SwallowingfaizaNo ratings yet
- Chapter - 021 Case StudyDocument2 pagesChapter - 021 Case Studydonnam86No ratings yet
- Nursing Care Plan - MergedDocument13 pagesNursing Care Plan - MergedJuls Flares SycaycoNo ratings yet
- Clinical Learning Skills Laboratory: College of NursingDocument3 pagesClinical Learning Skills Laboratory: College of NursingBeverly DatuNo ratings yet
- Nursing Practice IDocument9 pagesNursing Practice INeenya SisonNo ratings yet
- C. Diet Date Ordered Date Performed Date Changed General Description Indications Specific Foods Taken Client's Reaction And/or Reaction To The DietDocument35 pagesC. Diet Date Ordered Date Performed Date Changed General Description Indications Specific Foods Taken Client's Reaction And/or Reaction To The Dieteuqilegna_13No ratings yet
- Chapter 10: Nursing Care Related To Psychological and Physiologic Changes of PregnancyDocument4 pagesChapter 10: Nursing Care Related To Psychological and Physiologic Changes of PregnancyAlyssaGrandeMontimorNo ratings yet
- Electrolyte ImbalanceDocument4 pagesElectrolyte ImbalanceDoneva Lyn MedinaNo ratings yet
- NCPDocument2 pagesNCPMelissa David100% (1)
- RLE Checklist Administering Oxygen by Cannula or FacemaskDocument2 pagesRLE Checklist Administering Oxygen by Cannula or FacemaskQuantum XavierNo ratings yet
- Cesarean Section PDFDocument9 pagesCesarean Section PDFIeien MuthmainnahNo ratings yet
- Fundamentals of Nursing NCLEX Practice Questions Quiz 1Document39 pagesFundamentals of Nursing NCLEX Practice Questions Quiz 1Regine Mae Encinada100% (1)
- Influenza VirusDocument17 pagesInfluenza Virusapi-458845511No ratings yet
- NCM 112 Computation 2021Document3 pagesNCM 112 Computation 2021Marie Kelsey Acena Macaraig100% (1)
- Part 2 Gastro New NotesDocument12 pagesPart 2 Gastro New NotesanreilegardeNo ratings yet
- Types of Diagnosis:: Problem-Focused Nursing Diagnoses Have Three Components: (1) Nursing DiagnosisDocument4 pagesTypes of Diagnosis:: Problem-Focused Nursing Diagnoses Have Three Components: (1) Nursing DiagnosisDaisy MellaNo ratings yet
- Cultural Diversity in HealthDocument23 pagesCultural Diversity in HealthYemaya84No ratings yet
- Health PromotionDocument5 pagesHealth Promotionapi-433917537No ratings yet
- Desires - How Are You Feeling Today Sir? If Huminto Po Si PT, Iallow Po Natin Siya & Bigyan Siya NG Time To Fully Undertand What He Is Feeling Right Now.Document19 pagesDesires - How Are You Feeling Today Sir? If Huminto Po Si PT, Iallow Po Natin Siya & Bigyan Siya NG Time To Fully Undertand What He Is Feeling Right Now.melodia gandezaNo ratings yet
- Asthma Impaired Gas ExchangeDocument2 pagesAsthma Impaired Gas ExchangeAndrea Chua BuadoNo ratings yet
- Pex 02 07 PDFDocument6 pagesPex 02 07 PDFIlya Viner80% (5)
- Common Medical AbbreviationsDocument3 pagesCommon Medical AbbreviationsBráian Tzéims άλμπαNo ratings yet
- Ladybelle P. Gototos Geriatric Nursing Bsn3 Set1 NCPDocument2 pagesLadybelle P. Gototos Geriatric Nursing Bsn3 Set1 NCPLadybelle GototosNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainSian Grace AsadaNo ratings yet
- Maternal Notes Google DocsDocument24 pagesMaternal Notes Google DocsOracion, Bernette Meiji B.No ratings yet
- Medication - ALT-Template Polythene GlycolDocument1 pageMedication - ALT-Template Polythene GlycolNancyAmissahNo ratings yet
- Surgical Handwashing Name: Renebeth Caye I. Buaya Grade: - Year and Section: BSN II - C Date: September 15, 2021 LegendDocument16 pagesSurgical Handwashing Name: Renebeth Caye I. Buaya Grade: - Year and Section: BSN II - C Date: September 15, 2021 LegendMierre SiriusNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Cu 4Document3 pagesCu 4Paul SahagunNo ratings yet
- Dr. Ziad Arandi (Psychiatric MCQS)Document16 pagesDr. Ziad Arandi (Psychiatric MCQS)Firas Anaya100% (1)
- Betty NeumanDocument15 pagesBetty NeumanNunung Syamsuddin100% (1)
- Discoid Lupus Erythematosus - Background, Etiology, EpidemiologyDocument8 pagesDiscoid Lupus Erythematosus - Background, Etiology, EpidemiologyJair MathewsNo ratings yet
- General Treatment of PoisoningDocument4 pagesGeneral Treatment of PoisoningmahnoorNo ratings yet
- Major Depressive DisorderDocument3 pagesMajor Depressive Disorderregz1No ratings yet
- Deficiency LetterDocument1 pageDeficiency LetterTanmoy Pal ChowdhuryNo ratings yet
- Schallware (Watermark)Document9 pagesSchallware (Watermark)mat koolNo ratings yet
- Research PaperDocument95 pagesResearch PaperJest BmtNo ratings yet
- TECH 614 Full Spine I (Castellucci)Document10 pagesTECH 614 Full Spine I (Castellucci)Robert StraubNo ratings yet
- PIN2213 Occipital Nerve BlockDocument3 pagesPIN2213 Occipital Nerve BlockBob AdleNo ratings yet
- Cerebral Salt Wasting SyndromeDocument6 pagesCerebral Salt Wasting SyndromeBrian BaileyNo ratings yet
- Purpose: Be Able To Explain Definition of AnemiaDocument59 pagesPurpose: Be Able To Explain Definition of AnemiamelimindNo ratings yet
- Bionet BM3PatientMonitor - Service ManualDocument61 pagesBionet BM3PatientMonitor - Service ManualIvan Berino0% (1)
- PESCI /physical ExaminationsDocument5 pagesPESCI /physical ExaminationslaureeateNo ratings yet
- Global DiagnosisDocument5 pagesGlobal DiagnosisdrsmritiNo ratings yet
- Oncology NursingDocument18 pagesOncology NursingMichael Urrutia100% (1)
- Ca2 Mood Disorder Q&ADocument7 pagesCa2 Mood Disorder Q&AgeejeiNo ratings yet
- Medical TourismDocument74 pagesMedical TourismAndri FerdianNo ratings yet
- Case Report Lip BumperDocument10 pagesCase Report Lip Bumperalya noorNo ratings yet
- N A B H PDFDocument92 pagesN A B H PDFtapan_tsgNo ratings yet
- QuadramedDocument19 pagesQuadramedapi-282833051No ratings yet
- Second Announcement Sunshine 2019Document20 pagesSecond Announcement Sunshine 2019alvinNo ratings yet
- Drug Therapeutic Record: Naval State UniversityDocument6 pagesDrug Therapeutic Record: Naval State UniversityJuliusSerdeñaTrapalNo ratings yet
- Pulmonary Rehabilitation ExercisesDocument28 pagesPulmonary Rehabilitation ExercisesAdrian AlzNo ratings yet
- Dentaltown 2018marchDocument113 pagesDentaltown 2018marchDanutz BalanNo ratings yet
- NCP For FractureDocument4 pagesNCP For FracturePeejay Padigdig Feliciano100% (2)
- Non Opioid AnalgesicsDocument5 pagesNon Opioid AnalgesicsIsa AdelaNo ratings yet