Download as pdf or txt
You might also like
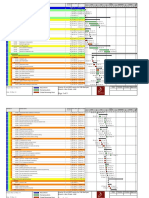
- PM Schedule Interior Fit Out Works For DIB Baniyas Branch Abu Dhabi UAE PDFDocument5 pagesPM Schedule Interior Fit Out Works For DIB Baniyas Branch Abu Dhabi UAE PDFXozan100% (1)
- Beginners Guide To Blackwork by Lesley Wilkins2 PDFDocument63 pagesBeginners Guide To Blackwork by Lesley Wilkins2 PDFSCP100% (4)
- Top 300 Drugs Pocket Reference Guide (2021 Edition)From EverandTop 300 Drugs Pocket Reference Guide (2021 Edition)Rating: 5 out of 5 stars5/5 (1)
- Multigrade Lesson Plan in Science Grade 3 and 4Document3 pagesMultigrade Lesson Plan in Science Grade 3 and 4Mayumi Solatre100% (9)
- Louis Hardan Mobile Dental Photography Part I ViaDocument9 pagesLouis Hardan Mobile Dental Photography Part I ViaMuchlis Fauzi ENo ratings yet
- Poisoning and Drug OverdoseDocument95 pagesPoisoning and Drug OverdoseMohammed Younis Shaheen100% (2)
- Opium poisoningDocument32 pagesOpium poisoningyolorafa768No ratings yet
- Opium and Its DerivativesDocument40 pagesOpium and Its DerivativesAswin KennedyNo ratings yet
- Cerebral Poison - OpiumDocument19 pagesCerebral Poison - Opiumlegendsinsider7781No ratings yet
- Somniferous Poisons: DR M. Malleswari Asso. Prof Nri Medical CollegeDocument58 pagesSomniferous Poisons: DR M. Malleswari Asso. Prof Nri Medical CollegeSudheera RachamallaNo ratings yet
- Drugs of Abuse: OpioidDocument35 pagesDrugs of Abuse: Opioidmalak amerNo ratings yet
- Opium HEROIN BARBITURATES HallucinogensDocument34 pagesOpium HEROIN BARBITURATES HallucinogensanuchahalNo ratings yet
- PoisoningDocument97 pagesPoisoningmaruf47774No ratings yet
- PoisoningDocument2 pagesPoisoningAkshay ShindeNo ratings yet
- (L14) Drug AddictionDocument49 pages(L14) Drug AddictionPrachiNo ratings yet
- Poisoning in ChildrenDocument44 pagesPoisoning in ChildrenYohanes FirmansyahNo ratings yet
- OpiumDocument30 pagesOpiumzainshNo ratings yet
- Opioid AnalgesicDocument12 pagesOpioid AnalgesicFaria Islam JuhiNo ratings yet
- Toxicological Hazards On BoardDocument17 pagesToxicological Hazards On Boardthetaungmoe79No ratings yet
- Drugs and Their AbusesDocument23 pagesDrugs and Their AbusesAkshaya SuruthiNo ratings yet
- Opioids AbuseDocument24 pagesOpioids Abusenurtasya mufridaNo ratings yet
- Organophosphoruspoisoning 180211164511Document21 pagesOrganophosphoruspoisoning 180211164511Happy chifundaNo ratings yet
- Discussion On Substance AbuseDocument33 pagesDiscussion On Substance AbuseTiong NeeNo ratings yet
- KeracunanDocument49 pagesKeracunanNi Made Dwiki AndriyaniNo ratings yet
- Mechanisms of Opioid AddictionDocument10 pagesMechanisms of Opioid AddictionAisha ShahzadNo ratings yet
- Presented byDocument71 pagesPresented byRun HajNo ratings yet
- 10e Kerosene and PetroleumDocument20 pages10e Kerosene and PetroleumShruthiNo ratings yet
- Opioids - An IntroductionDocument48 pagesOpioids - An IntroductionPranathi PrasadNo ratings yet
- Pesticide PoisoningDocument34 pagesPesticide PoisoningappealingashishNo ratings yet
- OP PoisoningDocument14 pagesOP PoisoningAnmol KudalNo ratings yet
- 2 AnticholinesterasesDocument55 pages2 AnticholinesterasesSudhakar LakavathNo ratings yet
- Drug AbuseDocument38 pagesDrug AbuseARIF-UR-REHMAN100% (4)
- Opoid AnalgesicsDocument29 pagesOpoid AnalgesicsShivsharan100% (1)
- PoisoningDocument39 pagesPoisoningNatnael ShifferawNo ratings yet
- Pharmacology Respiratory DrugsDocument51 pagesPharmacology Respiratory DrugsAngel DamoNo ratings yet
- Pesticide PoisoningDocument37 pagesPesticide PoisoningShorouk selimmNo ratings yet
- Antipsychotic DrugsDocument4 pagesAntipsychotic DrugsClareNo ratings yet
- Reviewer 6Document6 pagesReviewer 6asdfdjfeonaNo ratings yet
- Opium Poisoning: Pooja Yadav 19M6805 Roll - No:14Document20 pagesOpium Poisoning: Pooja Yadav 19M6805 Roll - No:14Pooja YadavNo ratings yet
- Organophosphorus PoisoningDocument15 pagesOrganophosphorus PoisoningtaufiAmaneeNo ratings yet
- Opioids PoisoningDocument34 pagesOpioids PoisoningRashmi Nayaka100% (6)
- Pesticide PoisoningDocument34 pagesPesticide PoisoningpreethiNo ratings yet
- Organophosphorus PoisoningDocument6 pagesOrganophosphorus PoisoningNishaAhsin0% (1)
- Drug DependenceDocument6 pagesDrug DependenceDomie AbataNo ratings yet
- General Drug PresentationDocument41 pagesGeneral Drug PresentationImran HasanNo ratings yet
- Pengantar Toksikologi Dan ToxindromeDocument29 pagesPengantar Toksikologi Dan ToxindromeCalvin Tanuwijaya Stick BolaNo ratings yet
- Opioid Analgesics: Dr. D. K. Brahma Department of Pharmacology, NEIGRIHMS Shillong, Meghalaya, ImdiaDocument48 pagesOpioid Analgesics: Dr. D. K. Brahma Department of Pharmacology, NEIGRIHMS Shillong, Meghalaya, ImdiaAmiraBenhammou100% (1)
- OpioidsDocument29 pagesOpioidsHassan Jahangir100% (1)
- Management of Acute Poisoning ANISH FINALDocument92 pagesManagement of Acute Poisoning ANISH FINALAnish JoshiNo ratings yet
- Pharmacology Bullet ReviewDocument36 pagesPharmacology Bullet ReviewNa Young You100% (1)
- Alex& Anteneh 1Document41 pagesAlex& Anteneh 1Amanuel LemiNo ratings yet
- Organophosphate Poisoning (Reference Material For OSCE)Document29 pagesOrganophosphate Poisoning (Reference Material For OSCE)hovico3936No ratings yet
- Organophosphates and Carbamates PoisoningDocument34 pagesOrganophosphates and Carbamates PoisoningMuhammad Hammad Maahi100% (1)
- Carbamate PoisoningDocument18 pagesCarbamate PoisoningJulie Ann TrinidadNo ratings yet
- Opioid AnalgesicsDocument16 pagesOpioid AnalgesicsSanthosh Krishna RajanNo ratings yet
- DrugsDocument22 pagesDrugsChase BallesterosNo ratings yet
- Agricultural PoisonDocument25 pagesAgricultural Poisons.shreevarshiniNo ratings yet
- Case Study No. 1 The Polydrug Overdose: Medical TermsDocument15 pagesCase Study No. 1 The Polydrug Overdose: Medical TermsMylz MendozaNo ratings yet
- CH 54 UpperDocument41 pagesCH 54 UpperKate Angelique RodriguezNo ratings yet
- Narcotic AnalgesicsDocument34 pagesNarcotic AnalgesicsScribdTranslationsNo ratings yet
- Narcotics Abuse Spring 2021Document51 pagesNarcotics Abuse Spring 2021Fatma HishamNo ratings yet
- CC3 Finals Toxicology of The Drugs of Abuse-1Document4 pagesCC3 Finals Toxicology of The Drugs of Abuse-1Gabriel QuillNo ratings yet
- OpiodsDocument117 pagesOpiodsTaniya GuptaNo ratings yet
- Pancretic Neuroendocrine Tumors - BasisDocument1 pagePancretic Neuroendocrine Tumors - BasisUsmanNo ratings yet
- CorticosteroidsDocument4 pagesCorticosteroidsUsmanNo ratings yet
- Hyper and Hypothyroidisim DrugsDocument3 pagesHyper and Hypothyroidisim DrugsUsmanNo ratings yet
- Drugs For DiabetesDocument8 pagesDrugs For DiabetesUsmanNo ratings yet
- EndocrineDocument17 pagesEndocrineUsmanNo ratings yet
- Forensic LawsDocument2 pagesForensic LawsUsmanNo ratings yet
- GIT and Liver TopicsDocument4 pagesGIT and Liver TopicsUsmanNo ratings yet
- DiureticsDocument5 pagesDiureticsUsmanNo ratings yet
- GIT and LiverDocument28 pagesGIT and LiverUsmanNo ratings yet
- Coupling - Machine DesignDocument73 pagesCoupling - Machine DesignAk GamingNo ratings yet
- SRS For Hotel Management SystemDocument16 pagesSRS For Hotel Management SystemAdarsh SinghNo ratings yet
- PeriodontitisDocument14 pagesPeriodontitisDanni MontielNo ratings yet
- House of ConcreteDocument9 pagesHouse of ConcreteArkyadeep ChowdhuryNo ratings yet
- Speaking/Conversation Placement-Test Interview: From Commonsense-Esl. ComDocument3 pagesSpeaking/Conversation Placement-Test Interview: From Commonsense-Esl. ComEmilia VoNo ratings yet
- Photo Essay PDFDocument2 pagesPhoto Essay PDFMartha Glorie Manalo WallisNo ratings yet
- ATV930 950 Installation Manual EN NHA80932 01Document129 pagesATV930 950 Installation Manual EN NHA80932 01ahilsergeyNo ratings yet
- Forest Laws and Their Impact On Adivasi Economy in Colonial India1Document12 pagesForest Laws and Their Impact On Adivasi Economy in Colonial India1NidhiNo ratings yet
- Safar Ki Dua - Travel SupplicationinvocationDocument1 pageSafar Ki Dua - Travel SupplicationinvocationShamshad Begum ShaikNo ratings yet
- 1.socio Economic Determinants of HealthDocument64 pages1.socio Economic Determinants of HealthdenekeNo ratings yet
- Rogalsky - The Working Poor and What GIS Reveals About The Possibilities of Public Transit PDFDocument12 pagesRogalsky - The Working Poor and What GIS Reveals About The Possibilities of Public Transit PDFMiaNo ratings yet
- 2.2 Evaluating Economic PerformanceDocument12 pages2.2 Evaluating Economic PerformanceMissDangNo ratings yet
- Topic 7 Reference Group and Word-Of-MouthDocument20 pagesTopic 7 Reference Group and Word-Of-MouthKhang Nguyen DuyNo ratings yet
- Mutation CancellationDocument4 pagesMutation Cancellationkamran wahabNo ratings yet
- Wedding Venue List 1Document53 pagesWedding Venue List 1Vivek Kumar GuptaNo ratings yet
- Student Handbook 2019-2020Document30 pagesStudent Handbook 2019-2020Gaetan HammondNo ratings yet
- Sublimatex Company ProfileDocument17 pagesSublimatex Company ProfileMohamed MahmoudNo ratings yet
- Istanbul TurkeyDocument7 pagesIstanbul Turkeynoe mayanaNo ratings yet
- Literature Book: The Poem Dulce Et Decorum Est by Wilfred Owen PDFDocument8 pagesLiterature Book: The Poem Dulce Et Decorum Est by Wilfred Owen PDFIRFAN TANHANo ratings yet
- Secondary Research of Telecom SectorDocument3 pagesSecondary Research of Telecom SectorVikram BhadauriaNo ratings yet
- Haytham Abd Allah Ezbawy ResumeDocument3 pagesHaytham Abd Allah Ezbawy Resumehayssam ezbawyNo ratings yet
- Diploma in Creative Writing in English Project DCE-06 in IGNOUDocument7 pagesDiploma in Creative Writing in English Project DCE-06 in IGNOUTelika RamuNo ratings yet
- Lectures On The Mechanical Foundations of ThermodynamicsDocument99 pagesLectures On The Mechanical Foundations of ThermodynamicsMarta HerranzNo ratings yet
- Med Chem IV Sem Pre RuhsDocument1 pageMed Chem IV Sem Pre Ruhsabhay sharmaNo ratings yet
- Conflict Management, Team Coordination, and Performance Within Multicultural Temporary Projects: Evidence From The Construction IndustryDocument14 pagesConflict Management, Team Coordination, and Performance Within Multicultural Temporary Projects: Evidence From The Construction Industryjaveria khanNo ratings yet
- Chapter 4Document29 pagesChapter 4Jelan AlanoNo ratings yet