
Apss Vap
Apss Vap
You might also like
- 38t GEI41047 PDocument28 pages38t GEI41047 PJorge DiazNo ratings yet
- National Infection Control Guidelines - 2016 Draft For ConsultationDocument341 pagesNational Infection Control Guidelines - 2016 Draft For Consultationlimiya vargheseNo ratings yet
- Patient Safety Initiative Hospital Executive and Physician Leadership StrategiesDocument39 pagesPatient Safety Initiative Hospital Executive and Physician Leadership StrategiesDian Kharisma100% (1)
- ArcadiaDocument28 pagesArcadiaCristianApostolNo ratings yet
- Clinical Review: Checklists - Translating Evidence Into PracticeDocument9 pagesClinical Review: Checklists - Translating Evidence Into Practicehwchong5476No ratings yet
- Case Study 1Document4 pagesCase Study 1languha NgatiNo ratings yet
- Checklist Patient SafetyDocument15 pagesChecklist Patient SafetyKatherine Conlu Bengan100% (1)
- Hisi Aug07Document16 pagesHisi Aug07Nikesh ShahNo ratings yet
- VAP PreventionDocument8 pagesVAP PreventionJbl2328No ratings yet
- European Association of Hospital Pharmacists - Abstracts and Learning Objectives - Seminar 2 - 2017-08-02Document11 pagesEuropean Association of Hospital Pharmacists - Abstracts and Learning Objectives - Seminar 2 - 2017-08-02SIUSANTO HadiNo ratings yet
- Care Nurse As Well As The Institute For Healthcare Improvement (IHI) Website WereDocument10 pagesCare Nurse As Well As The Institute For Healthcare Improvement (IHI) Website WerenanikNo ratings yet
- Acute Care Implementation GuideDocument4 pagesAcute Care Implementation GuideEnrique AlonsoNo ratings yet
- Pre-And Postoperative Management Techniques. Before and After. Part 1: Medical MorbiditiesDocument6 pagesPre-And Postoperative Management Techniques. Before and After. Part 1: Medical MorbiditiesMostafa FayadNo ratings yet
- Ann Deerhake, MS, RN, CNL, CCRN: CNL USF Conference Logo 2011Document35 pagesAnn Deerhake, MS, RN, CNL, CCRN: CNL USF Conference Logo 2011Paolo VegaNo ratings yet
- Making Health Care Safer.2Document9 pagesMaking Health Care Safer.2YANNo ratings yet
- Evidence Based RUADocument12 pagesEvidence Based RUAAsma AliNo ratings yet
- JournalDocument5 pagesJournalCris TanNo ratings yet
- NCM 119 Module Safety Part 2 Standards Lesson Safety National Quality Forum 2009Document59 pagesNCM 119 Module Safety Part 2 Standards Lesson Safety National Quality Forum 2009Maria Victoria A. PraxidesNo ratings yet
- NR520 Module 3 Assessment Project Area of Interest FormDocument5 pagesNR520 Module 3 Assessment Project Area of Interest Form96rubadiri96No ratings yet
- Literature Review On Surgical Safety ChecklistDocument11 pagesLiterature Review On Surgical Safety Checklistfut0mipujeg3100% (1)
- Joint Commission Research PaperDocument8 pagesJoint Commission Research Paperuzypvhhkf100% (1)
- Integrated Care PathwayDocument3 pagesIntegrated Care PathwayFitri EmiNo ratings yet
- Removal of Sharp Object Patient SaftyDocument6 pagesRemoval of Sharp Object Patient SaftyAlibaba AlihaihaiNo ratings yet
- Guide To Infection Prevention For Outpatient Settings:: Minimum Expectations For Safe CareDocument42 pagesGuide To Infection Prevention For Outpatient Settings:: Minimum Expectations For Safe Caresalcais9042No ratings yet
- Ventilator Acquired Pneumonia - EditeDocument5 pagesVentilator Acquired Pneumonia - EditegggNo ratings yet
- Guide To Infection Prevention in Outpatient Settings: Minimum Expectations For Safe CareDocument16 pagesGuide To Infection Prevention in Outpatient Settings: Minimum Expectations For Safe CareJun Anteola100% (1)
- Leadership Analysis PaperDocument8 pagesLeadership Analysis Paperapi-238680155No ratings yet
- Research Paper On Ventilator Associated PneumoniaDocument8 pagesResearch Paper On Ventilator Associated PneumoniakwbfbzundNo ratings yet
- Chapter 1defining Patient Safety and Quality CareDocument6 pagesChapter 1defining Patient Safety and Quality CareErinNo ratings yet
- Quality Improvement ProcessDocument8 pagesQuality Improvement Processapi-283424486No ratings yet
- International Patient Safety GoalsDocument30 pagesInternational Patient Safety GoalsMuvenn Kannan50% (2)
- Clinical GovernanceDocument9 pagesClinical GovernanceSajid Rahman100% (1)
- Literature Review On Patient FallsDocument7 pagesLiterature Review On Patient Fallsaflsiosbe100% (1)
- Standatds of Ambulatory Care 7 2011Document17 pagesStandatds of Ambulatory Care 7 2011nikky costeNo ratings yet
- Ipsg # 2017 PDFDocument30 pagesIpsg # 2017 PDFDARRYLARANHA100% (1)
- Ambulatory-Carechecklist 508 11 2015 PDFDocument42 pagesAmbulatory-Carechecklist 508 11 2015 PDFAli GhanemNo ratings yet
- Ebp Project 5 FinalDocument6 pagesEbp Project 5 Finalapi-315880679No ratings yet
- Introduction To Patient SafetyDocument10 pagesIntroduction To Patient SafetyAshenafi TigabuNo ratings yet
- Infection Control NHS PolicyDocument12 pagesInfection Control NHS PolicyYahya Salem100% (1)
- VAP BundleDocument13 pagesVAP BundleVen DeeNo ratings yet
- Adverse Event or Near-Miss AnalysisDocument10 pagesAdverse Event or Near-Miss Analysisjahxtow safariNo ratings yet
- @EVIDENCE BASED PRACTICE - EditedDocument5 pages@EVIDENCE BASED PRACTICE - EditedSir Ben MwauNo ratings yet
- Blood Borne Pathogens PolicyDocument8 pagesBlood Borne Pathogens PolicyChris KristoffersonNo ratings yet
- Organization Name Occupational Health Service: OrganizatitionaDocument16 pagesOrganization Name Occupational Health Service: OrganizatitionaSA RAINo ratings yet
- Patient Safety Thesis PDFDocument6 pagesPatient Safety Thesis PDFasiagroverprovo67% (3)
- Fall Prevention Research PaperDocument8 pagesFall Prevention Research Paperorlfgcvkg100% (1)
- Early Mobility Guide For Reducing Ventilator-Associated Events in Mechanically Ventilated PatientsDocument28 pagesEarly Mobility Guide For Reducing Ventilator-Associated Events in Mechanically Ventilated PatientsRosmira Agreda CabreraNo ratings yet
- Introducing Quality Patient Safety ProgramDocument15 pagesIntroducing Quality Patient Safety ProgramfitriNo ratings yet
- ASE Reintro Statement FINALDocument14 pagesASE Reintro Statement FINALIrina Cabac-PogoreviciNo ratings yet
- Quality Improvement Paper FinalDocument11 pagesQuality Improvement Paper Finalapi-291740538No ratings yet
- Question of Acute CareDocument11 pagesQuestion of Acute CareKuberAiranNo ratings yet
- CF Rca TemplateDocument8 pagesCF Rca TemplateEsteban García EcheverryNo ratings yet
- HandOff PolicyGuidanceDocument3 pagesHandOff PolicyGuidanceMaria Francesca MapaNo ratings yet
- Advanced Practice and Leadership in Radiology NursingFrom EverandAdvanced Practice and Leadership in Radiology NursingKathleen A. GrossNo ratings yet
- NEUK 1464 (Revised) 1 (Updated)Document21 pagesNEUK 1464 (Revised) 1 (Updated)Sameen ShafaatNo ratings yet
- Residents Ai Example ProjectsDocument5 pagesResidents Ai Example ProjectsTrinidad InspectionNo ratings yet
- Vap Care Bundle FinalDocument4 pagesVap Care Bundle FinalMother of Mercy Hospital -Tacloban Inc.No ratings yet
- 10 Patient Safety and Invasive ProceduresDocument4 pages10 Patient Safety and Invasive Proceduresanojan100% (1)
- Quality Tools SRPDocument7 pagesQuality Tools SRPSaraNo ratings yet
- Sample Research ProposalDocument43 pagesSample Research ProposalLuis LazaroNo ratings yet
- Managemen MutuDocument8 pagesManagemen MutuMerty TaolinNo ratings yet
- Anti-Inflammatory and Analgesic Activities of Flavonoid and Saponin Fractions From Zizyphus Lotus (L.) LamDocument5 pagesAnti-Inflammatory and Analgesic Activities of Flavonoid and Saponin Fractions From Zizyphus Lotus (L.) LamDaris UntoroNo ratings yet
- Chain of InfectionDocument8 pagesChain of Infectionkim mimiNo ratings yet
- Iq TestDocument18 pagesIq TestAmrita BawaNo ratings yet
- Comparative Study Based On Thermal Efficiency of Solar Air HeatersDocument6 pagesComparative Study Based On Thermal Efficiency of Solar Air Heatershicham El FeroualiNo ratings yet
- Kala-2000 LedDocument2 pagesKala-2000 LedJohnNo ratings yet
- Mathilde III.: MaterialsDocument10 pagesMathilde III.: MaterialsMaria Jose Lopez Needham100% (1)
- World's TallestDocument6 pagesWorld's TallestMaryNo ratings yet
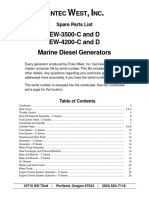
- EW-3500-C and D EW-4200-C and D Marine Diesel Generators: Ntec EST NCDocument27 pagesEW-3500-C and D EW-4200-C and D Marine Diesel Generators: Ntec EST NCGeorgiNo ratings yet
- Keratin TreatmentDocument2 pagesKeratin TreatmentDilinika PriyadarshaniNo ratings yet
- Standard Moisture Regain and Moisture Content of FibersDocument3 pagesStandard Moisture Regain and Moisture Content of Fibersff fixNo ratings yet
- Fitgurlmel's 365 Food Guide by Melissa AlcantaraDocument27 pagesFitgurlmel's 365 Food Guide by Melissa AlcantaraSinem YukselNo ratings yet
- AsDocument777 pagesAsCristhian QuimizNo ratings yet
- The New India Assurance Co. LTDDocument3 pagesThe New India Assurance Co. LTDsarath potnuriNo ratings yet
- Elements of Weather Climate Quarter 4 Week 3 Day 1-Day 41Document89 pagesElements of Weather Climate Quarter 4 Week 3 Day 1-Day 41BENJ AMINNo ratings yet
- Aquatic Games With BallsDocument13 pagesAquatic Games With BallsTet LopezNo ratings yet
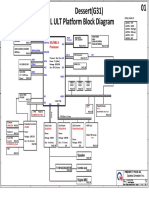
- Quanta G31a Dag31amb6d0 Y61x-6l Rev 1aDocument49 pagesQuanta G31a Dag31amb6d0 Y61x-6l Rev 1aKrystian PalaciosNo ratings yet
- Bar Graph Unit MonthDocument2 pagesBar Graph Unit MonthHimansh ChaprodNo ratings yet
- Acg01 IntroDocument34 pagesAcg01 IntroGiang T.C. TranNo ratings yet
- Assignment 1 Art HistoryDocument4 pagesAssignment 1 Art HistoryFarhanNo ratings yet
- Piplović - Dioklecijanova Palača U Splitu Nakon Careve SmrtiDocument32 pagesPiplović - Dioklecijanova Palača U Splitu Nakon Careve SmrtisliverhandNo ratings yet
- Alchemist Guide ProductionsDocument23 pagesAlchemist Guide ProductionsNovi NovianNo ratings yet
- Fluorescence Insitu HybridisationDocument9 pagesFluorescence Insitu Hybridisationtorseeker1100% (1)
- JTEC Manuscript Template v5Document3 pagesJTEC Manuscript Template v5علي عدنانNo ratings yet
- Lakhmir Singh Solutions Class 9 Feb 22 Chemistry Chapter 1 Matter in Our SurroundingsDocument13 pagesLakhmir Singh Solutions Class 9 Feb 22 Chemistry Chapter 1 Matter in Our SurroundingsDarshilNo ratings yet
- Transformer Protection Final Rev.01 PDFDocument2 pagesTransformer Protection Final Rev.01 PDFNader Asgar Pangarungan MamarobaNo ratings yet
- Chapter 10: Frequency Response Techniques 1Document60 pagesChapter 10: Frequency Response Techniques 1CesarNo ratings yet
- TAD531GE: Volvo Penta Genset EngineDocument2 pagesTAD531GE: Volvo Penta Genset EngineMATS DIVISIONNo ratings yet
- MushroomDocument64 pagesMushroomDelfa CastillaNo ratings yet
























































































Download as pdf or txt
You might also like
- 38t GEI41047 PDocument28 pages38t GEI41047 PJorge DiazNo ratings yet
- National Infection Control Guidelines - 2016 Draft For ConsultationDocument341 pagesNational Infection Control Guidelines - 2016 Draft For Consultationlimiya vargheseNo ratings yet
- Patient Safety Initiative Hospital Executive and Physician Leadership StrategiesDocument39 pagesPatient Safety Initiative Hospital Executive and Physician Leadership StrategiesDian Kharisma100% (1)
- ArcadiaDocument28 pagesArcadiaCristianApostolNo ratings yet
- Clinical Review: Checklists - Translating Evidence Into PracticeDocument9 pagesClinical Review: Checklists - Translating Evidence Into Practicehwchong5476No ratings yet
- Case Study 1Document4 pagesCase Study 1languha NgatiNo ratings yet
- Checklist Patient SafetyDocument15 pagesChecklist Patient SafetyKatherine Conlu Bengan100% (1)
- Hisi Aug07Document16 pagesHisi Aug07Nikesh ShahNo ratings yet
- VAP PreventionDocument8 pagesVAP PreventionJbl2328No ratings yet
- European Association of Hospital Pharmacists - Abstracts and Learning Objectives - Seminar 2 - 2017-08-02Document11 pagesEuropean Association of Hospital Pharmacists - Abstracts and Learning Objectives - Seminar 2 - 2017-08-02SIUSANTO HadiNo ratings yet
- Care Nurse As Well As The Institute For Healthcare Improvement (IHI) Website WereDocument10 pagesCare Nurse As Well As The Institute For Healthcare Improvement (IHI) Website WerenanikNo ratings yet
- Acute Care Implementation GuideDocument4 pagesAcute Care Implementation GuideEnrique AlonsoNo ratings yet
- Pre-And Postoperative Management Techniques. Before and After. Part 1: Medical MorbiditiesDocument6 pagesPre-And Postoperative Management Techniques. Before and After. Part 1: Medical MorbiditiesMostafa FayadNo ratings yet
- Ann Deerhake, MS, RN, CNL, CCRN: CNL USF Conference Logo 2011Document35 pagesAnn Deerhake, MS, RN, CNL, CCRN: CNL USF Conference Logo 2011Paolo VegaNo ratings yet
- Making Health Care Safer.2Document9 pagesMaking Health Care Safer.2YANNo ratings yet
- Evidence Based RUADocument12 pagesEvidence Based RUAAsma AliNo ratings yet
- JournalDocument5 pagesJournalCris TanNo ratings yet
- NCM 119 Module Safety Part 2 Standards Lesson Safety National Quality Forum 2009Document59 pagesNCM 119 Module Safety Part 2 Standards Lesson Safety National Quality Forum 2009Maria Victoria A. PraxidesNo ratings yet
- NR520 Module 3 Assessment Project Area of Interest FormDocument5 pagesNR520 Module 3 Assessment Project Area of Interest Form96rubadiri96No ratings yet
- Literature Review On Surgical Safety ChecklistDocument11 pagesLiterature Review On Surgical Safety Checklistfut0mipujeg3100% (1)
- Joint Commission Research PaperDocument8 pagesJoint Commission Research Paperuzypvhhkf100% (1)
- Integrated Care PathwayDocument3 pagesIntegrated Care PathwayFitri EmiNo ratings yet
- Removal of Sharp Object Patient SaftyDocument6 pagesRemoval of Sharp Object Patient SaftyAlibaba AlihaihaiNo ratings yet
- Guide To Infection Prevention For Outpatient Settings:: Minimum Expectations For Safe CareDocument42 pagesGuide To Infection Prevention For Outpatient Settings:: Minimum Expectations For Safe Caresalcais9042No ratings yet
- Ventilator Acquired Pneumonia - EditeDocument5 pagesVentilator Acquired Pneumonia - EditegggNo ratings yet
- Guide To Infection Prevention in Outpatient Settings: Minimum Expectations For Safe CareDocument16 pagesGuide To Infection Prevention in Outpatient Settings: Minimum Expectations For Safe CareJun Anteola100% (1)
- Leadership Analysis PaperDocument8 pagesLeadership Analysis Paperapi-238680155No ratings yet
- Research Paper On Ventilator Associated PneumoniaDocument8 pagesResearch Paper On Ventilator Associated PneumoniakwbfbzundNo ratings yet
- Chapter 1defining Patient Safety and Quality CareDocument6 pagesChapter 1defining Patient Safety and Quality CareErinNo ratings yet
- Quality Improvement ProcessDocument8 pagesQuality Improvement Processapi-283424486No ratings yet
- International Patient Safety GoalsDocument30 pagesInternational Patient Safety GoalsMuvenn Kannan50% (2)
- Clinical GovernanceDocument9 pagesClinical GovernanceSajid Rahman100% (1)
- Literature Review On Patient FallsDocument7 pagesLiterature Review On Patient Fallsaflsiosbe100% (1)
- Standatds of Ambulatory Care 7 2011Document17 pagesStandatds of Ambulatory Care 7 2011nikky costeNo ratings yet
- Ipsg # 2017 PDFDocument30 pagesIpsg # 2017 PDFDARRYLARANHA100% (1)
- Ambulatory-Carechecklist 508 11 2015 PDFDocument42 pagesAmbulatory-Carechecklist 508 11 2015 PDFAli GhanemNo ratings yet
- Ebp Project 5 FinalDocument6 pagesEbp Project 5 Finalapi-315880679No ratings yet
- Introduction To Patient SafetyDocument10 pagesIntroduction To Patient SafetyAshenafi TigabuNo ratings yet
- Infection Control NHS PolicyDocument12 pagesInfection Control NHS PolicyYahya Salem100% (1)
- VAP BundleDocument13 pagesVAP BundleVen DeeNo ratings yet
- Adverse Event or Near-Miss AnalysisDocument10 pagesAdverse Event or Near-Miss Analysisjahxtow safariNo ratings yet
- @EVIDENCE BASED PRACTICE - EditedDocument5 pages@EVIDENCE BASED PRACTICE - EditedSir Ben MwauNo ratings yet
- Blood Borne Pathogens PolicyDocument8 pagesBlood Borne Pathogens PolicyChris KristoffersonNo ratings yet
- Organization Name Occupational Health Service: OrganizatitionaDocument16 pagesOrganization Name Occupational Health Service: OrganizatitionaSA RAINo ratings yet
- Patient Safety Thesis PDFDocument6 pagesPatient Safety Thesis PDFasiagroverprovo67% (3)
- Fall Prevention Research PaperDocument8 pagesFall Prevention Research Paperorlfgcvkg100% (1)
- Early Mobility Guide For Reducing Ventilator-Associated Events in Mechanically Ventilated PatientsDocument28 pagesEarly Mobility Guide For Reducing Ventilator-Associated Events in Mechanically Ventilated PatientsRosmira Agreda CabreraNo ratings yet
- Introducing Quality Patient Safety ProgramDocument15 pagesIntroducing Quality Patient Safety ProgramfitriNo ratings yet
- ASE Reintro Statement FINALDocument14 pagesASE Reintro Statement FINALIrina Cabac-PogoreviciNo ratings yet
- Quality Improvement Paper FinalDocument11 pagesQuality Improvement Paper Finalapi-291740538No ratings yet
- Question of Acute CareDocument11 pagesQuestion of Acute CareKuberAiranNo ratings yet
- CF Rca TemplateDocument8 pagesCF Rca TemplateEsteban García EcheverryNo ratings yet
- HandOff PolicyGuidanceDocument3 pagesHandOff PolicyGuidanceMaria Francesca MapaNo ratings yet
- Advanced Practice and Leadership in Radiology NursingFrom EverandAdvanced Practice and Leadership in Radiology NursingKathleen A. GrossNo ratings yet
- NEUK 1464 (Revised) 1 (Updated)Document21 pagesNEUK 1464 (Revised) 1 (Updated)Sameen ShafaatNo ratings yet
- Residents Ai Example ProjectsDocument5 pagesResidents Ai Example ProjectsTrinidad InspectionNo ratings yet
- Vap Care Bundle FinalDocument4 pagesVap Care Bundle FinalMother of Mercy Hospital -Tacloban Inc.No ratings yet
- 10 Patient Safety and Invasive ProceduresDocument4 pages10 Patient Safety and Invasive Proceduresanojan100% (1)
- Quality Tools SRPDocument7 pagesQuality Tools SRPSaraNo ratings yet
- Sample Research ProposalDocument43 pagesSample Research ProposalLuis LazaroNo ratings yet
- Managemen MutuDocument8 pagesManagemen MutuMerty TaolinNo ratings yet
- Anti-Inflammatory and Analgesic Activities of Flavonoid and Saponin Fractions From Zizyphus Lotus (L.) LamDocument5 pagesAnti-Inflammatory and Analgesic Activities of Flavonoid and Saponin Fractions From Zizyphus Lotus (L.) LamDaris UntoroNo ratings yet
- Chain of InfectionDocument8 pagesChain of Infectionkim mimiNo ratings yet
- Iq TestDocument18 pagesIq TestAmrita BawaNo ratings yet
- Comparative Study Based On Thermal Efficiency of Solar Air HeatersDocument6 pagesComparative Study Based On Thermal Efficiency of Solar Air Heatershicham El FeroualiNo ratings yet
- Kala-2000 LedDocument2 pagesKala-2000 LedJohnNo ratings yet
- Mathilde III.: MaterialsDocument10 pagesMathilde III.: MaterialsMaria Jose Lopez Needham100% (1)
- World's TallestDocument6 pagesWorld's TallestMaryNo ratings yet
- EW-3500-C and D EW-4200-C and D Marine Diesel Generators: Ntec EST NCDocument27 pagesEW-3500-C and D EW-4200-C and D Marine Diesel Generators: Ntec EST NCGeorgiNo ratings yet
- Keratin TreatmentDocument2 pagesKeratin TreatmentDilinika PriyadarshaniNo ratings yet
- Standard Moisture Regain and Moisture Content of FibersDocument3 pagesStandard Moisture Regain and Moisture Content of Fibersff fixNo ratings yet
- Fitgurlmel's 365 Food Guide by Melissa AlcantaraDocument27 pagesFitgurlmel's 365 Food Guide by Melissa AlcantaraSinem YukselNo ratings yet
- AsDocument777 pagesAsCristhian QuimizNo ratings yet
- The New India Assurance Co. LTDDocument3 pagesThe New India Assurance Co. LTDsarath potnuriNo ratings yet
- Elements of Weather Climate Quarter 4 Week 3 Day 1-Day 41Document89 pagesElements of Weather Climate Quarter 4 Week 3 Day 1-Day 41BENJ AMINNo ratings yet
- Aquatic Games With BallsDocument13 pagesAquatic Games With BallsTet LopezNo ratings yet
- Quanta G31a Dag31amb6d0 Y61x-6l Rev 1aDocument49 pagesQuanta G31a Dag31amb6d0 Y61x-6l Rev 1aKrystian PalaciosNo ratings yet
- Bar Graph Unit MonthDocument2 pagesBar Graph Unit MonthHimansh ChaprodNo ratings yet
- Acg01 IntroDocument34 pagesAcg01 IntroGiang T.C. TranNo ratings yet
- Assignment 1 Art HistoryDocument4 pagesAssignment 1 Art HistoryFarhanNo ratings yet
- Piplović - Dioklecijanova Palača U Splitu Nakon Careve SmrtiDocument32 pagesPiplović - Dioklecijanova Palača U Splitu Nakon Careve SmrtisliverhandNo ratings yet
- Alchemist Guide ProductionsDocument23 pagesAlchemist Guide ProductionsNovi NovianNo ratings yet
- Fluorescence Insitu HybridisationDocument9 pagesFluorescence Insitu Hybridisationtorseeker1100% (1)
- JTEC Manuscript Template v5Document3 pagesJTEC Manuscript Template v5علي عدنانNo ratings yet
- Lakhmir Singh Solutions Class 9 Feb 22 Chemistry Chapter 1 Matter in Our SurroundingsDocument13 pagesLakhmir Singh Solutions Class 9 Feb 22 Chemistry Chapter 1 Matter in Our SurroundingsDarshilNo ratings yet
- Transformer Protection Final Rev.01 PDFDocument2 pagesTransformer Protection Final Rev.01 PDFNader Asgar Pangarungan MamarobaNo ratings yet
- Chapter 10: Frequency Response Techniques 1Document60 pagesChapter 10: Frequency Response Techniques 1CesarNo ratings yet
- TAD531GE: Volvo Penta Genset EngineDocument2 pagesTAD531GE: Volvo Penta Genset EngineMATS DIVISIONNo ratings yet
- MushroomDocument64 pagesMushroomDelfa CastillaNo ratings yet