Download as pdf or txt
You might also like
- Sample CPJE: Finasteride 1 MG Tablets #30 1 Tab P.O. Daily For Benign Prostatic HyperplasiaDocument12 pagesSample CPJE: Finasteride 1 MG Tablets #30 1 Tab P.O. Daily For Benign Prostatic HyperplasiaHerne Balberde78% (9)
- Case Study On Pre EclampsiaDocument21 pagesCase Study On Pre EclampsiaKavi rajput96% (24)
- Antimicrobial Photodynamic Therapy With Diode Laser and Methylene Blue As An Adjunct To Scaling and Root Planning A Clinical TrialDocument5 pagesAntimicrobial Photodynamic Therapy With Diode Laser and Methylene Blue As An Adjunct To Scaling and Root Planning A Clinical TrialFelipe AraujoNo ratings yet
- The Clinical Effect of Diode Laser in The Treatment of The Periodontal Pockets in Comparison With The Use of Photodynamic TherapyDocument18 pagesThe Clinical Effect of Diode Laser in The Treatment of The Periodontal Pockets in Comparison With The Use of Photodynamic TherapyAthenaeum Scientific PublishersNo ratings yet
- Yutaro Kitanaka Article PDFDocument23 pagesYutaro Kitanaka Article PDFNay AungNo ratings yet
- Effectiveness of Antimicrobial Photodynamic Therapy in The Periodontis Systematic ReviewDocument42 pagesEffectiveness of Antimicrobial Photodynamic Therapy in The Periodontis Systematic ReviewreizkayNo ratings yet
- 2 PDFDocument6 pages2 PDFEmaNo ratings yet
- JR PERIO Evaluation of The ReactiveDocument7 pagesJR PERIO Evaluation of The ReactivemediyantiNo ratings yet
- J PDPDT 2017 11 018Document15 pagesJ PDPDT 2017 11 018Yusuf DiansyahNo ratings yet
- Microorganisms 09 00713 v2Document15 pagesMicroorganisms 09 00713 v2Delia Guadalupe Gardea ContrerasNo ratings yet
- 9548 67097 1 PB PDFDocument7 pages9548 67097 1 PB PDFKarim KhedimNo ratings yet
- Periodontal Tray Application of Chlorine Dioxide Gel As An Adjunct To Scaling and Root Planing in The Treatment of Chronic PeriodontitisDocument6 pagesPeriodontal Tray Application of Chlorine Dioxide Gel As An Adjunct To Scaling and Root Planing in The Treatment of Chronic PeriodontitisPhuong ThaoNo ratings yet
- Life 12 00370Document10 pagesLife 12 00370Mind Mapping Dept of Cons & EndoNo ratings yet
- Analyze The Clinical Effect of YAG Laser CombinedDocument9 pagesAnalyze The Clinical Effect of YAG Laser CombinedJose Luis AnayaNo ratings yet
- Javed 2013Document7 pagesJaved 2013Peter von TanNo ratings yet
- 10835-Article Text-51780-1-10-20220425Document9 pages10835-Article Text-51780-1-10-20220425Wilma Nurul AzizahNo ratings yet
- The Effect of Injectable Platelet-Rich Fibrin Use in TheDocument6 pagesThe Effect of Injectable Platelet-Rich Fibrin Use in TheNurul Fajriah YunitaNo ratings yet
- Comparison Between Antimicrobial Photodynamic Therapy and Low-Level Laser Therapy On Non-Surgical Periodontal Treatment A Clinical StudyDocument6 pagesComparison Between Antimicrobial Photodynamic Therapy and Low-Level Laser Therapy On Non-Surgical Periodontal Treatment A Clinical StudyFelipe AraujoNo ratings yet
- Photodiagnosis and Photodynamic Therapy: ReviewDocument7 pagesPhotodiagnosis and Photodynamic Therapy: ReviewCristian AndriescuNo ratings yet
- Comparison of Efficacy of Probiotics Versus.9Document6 pagesComparison of Efficacy of Probiotics Versus.9samanvi badriNo ratings yet
- Photo-Biomodulation in EndodonticsDocument7 pagesPhoto-Biomodulation in EndodonticsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Багрила концентрацииDocument12 pagesБагрила концентрацииМихаил ТаневNo ratings yet
- Comparative Evaluation of Locally Delivered.12Document7 pagesComparative Evaluation of Locally Delivered.12samanvi badriNo ratings yet
- ParoDocument8 pagesParoOctavian BoaruNo ratings yet
- J Clinic Periodontology - 2020 - Sanz - Treatment of Stage I III Periodontitis The EFP S3 Level Clinical Practice GuidelineDocument57 pagesJ Clinic Periodontology - 2020 - Sanz - Treatment of Stage I III Periodontitis The EFP S3 Level Clinical Practice GuidelineKeHuyDietNo ratings yet
- Efficacy of Xanthan Based Chlorhexidine Gel As AnDocument5 pagesEfficacy of Xanthan Based Chlorhexidine Gel As AnMai ThúyNo ratings yet
- Chiniforush2016 PDT PDFDocument10 pagesChiniforush2016 PDT PDFShriya ShahuNo ratings yet
- Clinical Effectiveness of Diode Laser Therapy As An Adjunct To Non-Surgical Periodontal Treatment: A Randomized Clinical StudyDocument7 pagesClinical Effectiveness of Diode Laser Therapy As An Adjunct To Non-Surgical Periodontal Treatment: A Randomized Clinical StudyAnea MlinarNo ratings yet
- 1 s2.0 S1572100021003562 MainDocument6 pages1 s2.0 S1572100021003562 MainEduardo FernandezNo ratings yet
- Grzech-Leśniak2018 Article LaserReductionOfSpecificMicrooDocument10 pagesGrzech-Leśniak2018 Article LaserReductionOfSpecificMicrooeliasNo ratings yet
- Photobiomodulation in Endodontic, Restorative, and Prosthetic Dentistry: A Review of The LiteratureDocument18 pagesPhotobiomodulation in Endodontic, Restorative, and Prosthetic Dentistry: A Review of The LiteratureAbhishek NaikNo ratings yet
- Photobiomodulation in Endodontic, Restorative, and Prosthetic Dentistry: A Review of The LiteratureDocument18 pagesPhotobiomodulation in Endodontic, Restorative, and Prosthetic Dentistry: A Review of The LiteratureAbhishek NaikNo ratings yet
- OzonearticleDocument9 pagesOzonearticleسامر مضحيNo ratings yet
- Antibacterial Efficacy PH EWN Periodontal TreatmentDocument5 pagesAntibacterial Efficacy PH EWN Periodontal TreatmentSayabil AvendañoNo ratings yet
- Jurnal 2Document6 pagesJurnal 2Endy TiasNo ratings yet
- Wjoud 11 221Document5 pagesWjoud 11 221ReshmaaRajendranNo ratings yet
- Recent Advances in Clinical Periodontal DiagnosisDocument6 pagesRecent Advances in Clinical Periodontal DiagnosisSharmika SavanthNo ratings yet
- Toledano 2021 - Efficacy of Local Antibiotic Therapy in The Treatment of Peri-Implantitis A Systematic Review and Meta-AnalysisDocument9 pagesToledano 2021 - Efficacy of Local Antibiotic Therapy in The Treatment of Peri-Implantitis A Systematic Review and Meta-Analysissamusm.smNo ratings yet
- (PDF) Piperacillin-Tazobactam As An Adjuvant in The Mechanical Treatment of Patients With Periodontitis - A Randomized Clinical StudyDocument12 pages(PDF) Piperacillin-Tazobactam As An Adjuvant in The Mechanical Treatment of Patients With Periodontitis - A Randomized Clinical StudyAmruta MahajanNo ratings yet
- 5232 ArticleText 16212 2 10 201909291 PDFDocument5 pages5232 ArticleText 16212 2 10 201909291 PDFPutiNo ratings yet
- 2023 Efficacy of Adjunctive Measures in The Non-Surgical Treatment of Peri-Implantitis A Systematic ReviewDocument20 pages2023 Efficacy of Adjunctive Measures in The Non-Surgical Treatment of Peri-Implantitis A Systematic Reviewmatias cofreNo ratings yet
- Comparative Evaluation PF 1 Curcumin Solution and o 2 Chlorhexidine IrrigationDocument7 pagesComparative Evaluation PF 1 Curcumin Solution and o 2 Chlorhexidine Irrigationsamanvi badriNo ratings yet
- 2 ND JC PDF - SindhuDocument8 pages2 ND JC PDF - SindhuDadi SindhuNo ratings yet
- Probing Pocket Depth Reduction After Non Surgical Periodontal TherapyDocument11 pagesProbing Pocket Depth Reduction After Non Surgical Periodontal Therapymartesebastian081No ratings yet
- Impact of Periodontal Pocket Depth On The EfficienDocument7 pagesImpact of Periodontal Pocket Depth On The EfficienRonaldo PutraNo ratings yet
- Treatment Stage I-Iii J Clinic Periodontology - 2020 - Sanz - Treatment of Stage I III Periodontitis The EFP S3 Level Clinical Practice GuidelineDocument57 pagesTreatment Stage I-Iii J Clinic Periodontology - 2020 - Sanz - Treatment of Stage I III Periodontitis The EFP S3 Level Clinical Practice GuidelineSofia Zaematul ArifahNo ratings yet
- Supportive Periodontal Therapy: July 2018Document8 pagesSupportive Periodontal Therapy: July 2018Alaghen VespanathanNo ratings yet
- Journal Homepage: - : IntroductionDocument9 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Reconstructive Surgical Therapy of Peri-Implantitis: A Multicenter Randomized Controlled Clinical TrialDocument24 pagesReconstructive Surgical Therapy of Peri-Implantitis: A Multicenter Randomized Controlled Clinical Trialrmartins76No ratings yet
- Locally Administered Probiotic, RCT-articleDocument7 pagesLocally Administered Probiotic, RCT-articleDebjyoti DebnathNo ratings yet
- Jctres07202105003 EpubDocument18 pagesJctres07202105003 Epubسامر مضحيNo ratings yet
- Treatment of Stage I-III Periodontitis-The EFP S3 Level Clinical Practice GuidelineDocument57 pagesTreatment of Stage I-III Periodontitis-The EFP S3 Level Clinical Practice GuidelinePaulina Müller100% (1)
- 2794Document11 pages2794RodolfoDamásioNunesNo ratings yet
- Regeneration in Chronicperiodontitis-Casereports of OurdifferentproceduresDocument9 pagesRegeneration in Chronicperiodontitis-Casereports of Ourdifferentproceduresvishrutha purushothamNo ratings yet
- Cap 5Document22 pagesCap 5Elena DimitriuNo ratings yet
- Journal of Periodontology - 2022 - Andere - Open Flap Debridement Compared To Repeated Applications of Photodynamic TherapyDocument11 pagesJournal of Periodontology - 2022 - Andere - Open Flap Debridement Compared To Repeated Applications of Photodynamic TherapySalma HelmyNo ratings yet
- Chlorhexidine Oral Rinse Vs Povidone IodineDocument9 pagesChlorhexidine Oral Rinse Vs Povidone Iodineapi-733087623No ratings yet
- Systematic Review of Orthodontic Treatment ManagementDocument7 pagesSystematic Review of Orthodontic Treatment ManagementJuan AndradeNo ratings yet
- 1 s2.0 S0020653922001708 MainDocument11 pages1 s2.0 S0020653922001708 MainHONG JIN TANNo ratings yet
- Article MetaDocument13 pagesArticle MetaAkanksha SinghNo ratings yet
- Clinical Applications of Nuclear Medicine Targeted TherapyFrom EverandClinical Applications of Nuclear Medicine Targeted TherapyEmilio BombardieriNo ratings yet
- 978 613 4 99100 1Document69 pages978 613 4 99100 1salman khawarNo ratings yet
- Stain1 PDFDocument6 pagesStain1 PDFsalman khawarNo ratings yet
- Stain 2Document4 pagesStain 2salman khawarNo ratings yet
- New Doc 2019-02-08 10.51.43Document11 pagesNew Doc 2019-02-08 10.51.43salman khawarNo ratings yet
- Ijpi 2 (4) 136-140Document5 pagesIjpi 2 (4) 136-140salman khawarNo ratings yet
- Nsaids in PeriodontologyDocument7 pagesNsaids in Periodontologysalman khawarNo ratings yet
- Pengaruh Terapi Akupresur Dan Pijat Oksitosin Terhadap Peningkatan Produksi Asi Pada Ibu Postpartum Di Rsud JombangDocument10 pagesPengaruh Terapi Akupresur Dan Pijat Oksitosin Terhadap Peningkatan Produksi Asi Pada Ibu Postpartum Di Rsud Jombangriska yuniartiNo ratings yet
- Emergency Evacuation Plan For CradleDocument5 pagesEmergency Evacuation Plan For CradleAbraar AhmedhNo ratings yet
- Intermediate UveitisDocument33 pagesIntermediate UveitismitaamayNo ratings yet
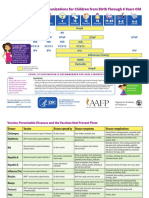
- Parent Ver SCH 0 6yrsDocument2 pagesParent Ver SCH 0 6yrsSrinivasamurthy KamarthiNo ratings yet
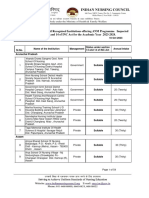
- Anm 10102023Document53 pagesAnm 10102023MANISHNo ratings yet
- LeprosyDocument34 pagesLeprosySubhashish DasNo ratings yet
- Attending Physicians Statement-Death ClaimDocument2 pagesAttending Physicians Statement-Death ClaimKen CelesteNo ratings yet
- FddfsDocument3 pagesFddfshlkuy tiutytyNo ratings yet
- NHMSFAP As Post Anesthesia CareDocument11 pagesNHMSFAP As Post Anesthesia CareOktavia PutriNo ratings yet
- Essay About ObesityDocument1 pageEssay About ObesityNgọc Thảo0% (1)
- Potential Conflicts of Interest. All Authors:: Clinical Infectious Diseases 2018 66 (8) :1316-7Document2 pagesPotential Conflicts of Interest. All Authors:: Clinical Infectious Diseases 2018 66 (8) :1316-7Chikondi TemboNo ratings yet
- Tuberculous Mastitis A Case ReportDocument4 pagesTuberculous Mastitis A Case ReportLmao DNo ratings yet
- Chakra - Factors Associated With Complications of C DiffDocument8 pagesChakra - Factors Associated With Complications of C DiffCherry SmileNo ratings yet
- Letter To EditorDocument1 pageLetter To EditorPARIJAT CHAKRABORTYNo ratings yet
- ACHONDROPLASIADocument18 pagesACHONDROPLASIAJennie Mayaute AllcaNo ratings yet
- Standard Operating Procedure (SOP) Niacin TestDocument5 pagesStandard Operating Procedure (SOP) Niacin TestSuci IrianiNo ratings yet
- Medical Home: Care Coordination: The Patient-CenteredDocument23 pagesMedical Home: Care Coordination: The Patient-CenteredDwi Suranto100% (1)
- CefepimeDocument1 pageCefepimeTracy Megan RusillonNo ratings yet
- Electrocardiographic Monitoring 2017Document72 pagesElectrocardiographic Monitoring 2017Mirela Marina BlajNo ratings yet
- Smoking CessationDocument4 pagesSmoking CessationAimee GutierrezNo ratings yet
- Emotion Release ChiroDocument12 pagesEmotion Release ChiroEurico GonçalvesNo ratings yet
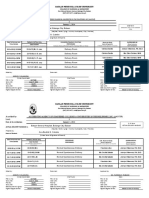
- 3 Date of Accreditation: January 1, 2014 Bataan General Hospital, Balanga City, BataanDocument3 pages3 Date of Accreditation: January 1, 2014 Bataan General Hospital, Balanga City, BataanArra BeatrizNo ratings yet
- Dental Students' Motivations and Perceptions of Dental Professional Career in IndiaDocument8 pagesDental Students' Motivations and Perceptions of Dental Professional Career in IndiaNiel Robert UyNo ratings yet
- Teks PidatoDocument5 pagesTeks Pidatorezpector9100% (1)
- 5 Minute Spotlight - Vacuum Extraction and Forceps DeliveryDocument2 pages5 Minute Spotlight - Vacuum Extraction and Forceps DeliveryMikeNo ratings yet
- 58-File Utama Naskah-62-1-10-20200928Document8 pages58-File Utama Naskah-62-1-10-20200928Alfaera Rahma FarestyNo ratings yet
- Case 6 Abnormal PsychologyDocument4 pagesCase 6 Abnormal PsychologyPrincess Hannah Nicole LATNo ratings yet
- 664 8537 1 PBDocument5 pages664 8537 1 PBMICHAEL NUGROHONo ratings yet