
Validation of Clinical Prediction Models What Does The Calibration PDF
Validation of Clinical Prediction Models What Does The Calibration PDF
You might also like
- Cte-Btvted - Syl-Edtm 158: Disclaimer: Reproduction of This Document Is Allowed SubjectDocument9 pagesCte-Btvted - Syl-Edtm 158: Disclaimer: Reproduction of This Document Is Allowed SubjectGeraldz Brenzon Agustin92% (12)
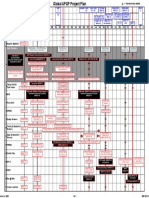
- GM 1927 01 Project PlanDocument1 pageGM 1927 01 Project Planmark100% (2)
- Expt 2Document7 pagesExpt 2toshgangwarNo ratings yet
- A Calibration Hierarchy For Risk ModelsDocument10 pagesA Calibration Hierarchy For Risk ModelsGuilherme MartheNo ratings yet
- The Kappa Statistic in Reliability Studies - Use, Interpretation, and Sample Size Requirements - Sim & Wright (2005) PDFDocument13 pagesThe Kappa Statistic in Reliability Studies - Use, Interpretation, and Sample Size Requirements - Sim & Wright (2005) PDFEduardo Aguirre DávilaNo ratings yet
- (Surgery (Oxford) 2009-Sep Vol. 27 Iss. 9) - MCQs (2009) (10.1016 - J.mpsur.2009.08.016) - Libgen - LiDocument2 pages(Surgery (Oxford) 2009-Sep Vol. 27 Iss. 9) - MCQs (2009) (10.1016 - J.mpsur.2009.08.016) - Libgen - LiSaleh El BarasiNo ratings yet
- Calibration: The Achilles Heel of Predictive Analytics: Opinion Open AccessDocument7 pagesCalibration: The Achilles Heel of Predictive Analytics: Opinion Open Accessandreitacool23No ratings yet
- Concepto de InertidumbreDocument6 pagesConcepto de InertidumbrePaul Avelino CallupeNo ratings yet
- BM28 1 010101Document10 pagesBM28 1 010101s.aliNo ratings yet
- Treatment of Bias in Estimating Measurement Uncertainty: Gregory E. O'Donnell and D. Brynn HibbertDocument9 pagesTreatment of Bias in Estimating Measurement Uncertainty: Gregory E. O'Donnell and D. Brynn HibbertaureaborosNo ratings yet
- Petersen 2010Document8 pagesPetersen 2010Justino WaveleNo ratings yet
- The Brier Score Does Not Evaluate The Clinical Utility of Diagnostic Tests or Prediction ModelsDocument7 pagesThe Brier Score Does Not Evaluate The Clinical Utility of Diagnostic Tests or Prediction ModelsJoão Pedro RibasNo ratings yet
- Reglas de Predicción ClínicaDocument7 pagesReglas de Predicción ClínicaCambriaChicoNo ratings yet
- CCLM Cyclosporin 18 PDFDocument13 pagesCCLM Cyclosporin 18 PDFSebastian SalinasNo ratings yet
- Assessing The Performance of PredictionDocument11 pagesAssessing The Performance of Predictionmamanpanti00No ratings yet
- Confiabilidad, Precisión o ReproducibilidadDocument9 pagesConfiabilidad, Precisión o ReproducibilidadelderNo ratings yet
- Review: Harmonization of Pre-Analytical Quality IndicatorsDocument9 pagesReview: Harmonization of Pre-Analytical Quality IndicatorsadrianaNo ratings yet
- Reliability, Repeatability and Reproducibility: Analysis of Measurement Errors in Continuous VariablesDocument10 pagesReliability, Repeatability and Reproducibility: Analysis of Measurement Errors in Continuous VariablesGregory GiovanardiNo ratings yet
- Sample Size in Diagnostic Accuracy StudiesDocument9 pagesSample Size in Diagnostic Accuracy StudiesSaurabh AgrawalNo ratings yet
- Ni Hms 438237Document21 pagesNi Hms 438237andreitacool23No ratings yet
- 1 s2.0 S2352551720301621 MainDocument15 pages1 s2.0 S2352551720301621 MainadrianaNo ratings yet
- Incertidumbre Rev MEx Pat Clin 19Document7 pagesIncertidumbre Rev MEx Pat Clin 19Lorena Ek MaciasNo ratings yet
- Clinical Examination For Diagnosing Circulatory Shock: ReviewDocument9 pagesClinical Examination For Diagnosing Circulatory Shock: ReviewAna Cláudia LeiteNo ratings yet
- The European Society of Cardiology Cardio-Oncology Guidelines Evidence Base, Actionability, and Relevance To Clinical PracticeDocument4 pagesThe European Society of Cardiology Cardio-Oncology Guidelines Evidence Base, Actionability, and Relevance To Clinical PracticeCsr ArsNo ratings yet
- Part 16 PDFDocument7 pagesPart 16 PDFKarolina PolskaNo ratings yet
- Twelve Tips For BlueprintingDocument4 pagesTwelve Tips For Blueprintingaatir javaidNo ratings yet
- Methodological Standards For The Development and Evaluation of Clinical Prediction Rules A Review of The LiteratureDocument23 pagesMethodological Standards For The Development and Evaluation of Clinical Prediction Rules A Review of The LiteratureTeoh Cherh YunNo ratings yet
- 10.1515@cclm 2018 1321Document2 pages10.1515@cclm 2018 1321Grescia Ramos VegaNo ratings yet
- 1 s2.0 S0895435615000141 MainDocument10 pages1 s2.0 S0895435615000141 MainBarron ManNo ratings yet
- BMJ I6 FullDocument5 pagesBMJ I6 FullRobertoNo ratings yet
- Jurnal Alin Poct Dipstk UrineDocument9 pagesJurnal Alin Poct Dipstk Urineherlina armarianiNo ratings yet
- GROC Review PDFDocument8 pagesGROC Review PDFPilar BralićNo ratings yet
- Clinical Trials CA WhitepaperDocument14 pagesClinical Trials CA WhitepaperNath ForestNo ratings yet
- Use of Recovery and Bias Information in Analytical Chemistry and Estimation of Its Uncertainty ContributionDocument9 pagesUse of Recovery and Bias Information in Analytical Chemistry and Estimation of Its Uncertainty ContributionRodney SalazarNo ratings yet
- Clinical Practice Guidelines in Breast Cancer: N. Kumar Tyagi and S. Dhesy-ThindDocument10 pagesClinical Practice Guidelines in Breast Cancer: N. Kumar Tyagi and S. Dhesy-ThindsanNo ratings yet
- Improving Healthcare Performance Through Activity-Based Costing and Time-Driven Activity-Based CostingDocument15 pagesImproving Healthcare Performance Through Activity-Based Costing and Time-Driven Activity-Based Costinghasan najiNo ratings yet
- Rating The Quality of Evidence-ImprecisionDocument13 pagesRating The Quality of Evidence-ImprecisionGeorgina CNo ratings yet
- Using Embedding-Based Metrics To Expedite Patients Recruitment Process For Clinical TrialsDocument7 pagesUsing Embedding-Based Metrics To Expedite Patients Recruitment Process For Clinical TrialshousseindhNo ratings yet
- PlebaniDocument2 pagesPlebaniGrescia Ramos VegaNo ratings yet
- 009 Analytical Chemistry at TheDocument8 pages009 Analytical Chemistry at TheRoberto Rolando Bauza FerminNo ratings yet
- BM 27 3 030502Document10 pagesBM 27 3 030502rnbansalNo ratings yet
- Assay Stability, The Missing Component of The Error BudgetDocument9 pagesAssay Stability, The Missing Component of The Error BudgetMezouar AbdennacerNo ratings yet
- cIL Ix1: A Multi-Rule Shewhart Chart For Quality Control in Clinical ChemistryDocument9 pagescIL Ix1: A Multi-Rule Shewhart Chart For Quality Control in Clinical ChemistryJustino WaveleNo ratings yet
- 57 FullDocument6 pages57 Full30. Tyanna Putri MinartiNo ratings yet
- Comparing Treatment Means Overlapping Standard Errors 52odf4albiDocument13 pagesComparing Treatment Means Overlapping Standard Errors 52odf4albiThazin HtayNo ratings yet
- Chapter 17 AuditingDocument48 pagesChapter 17 AuditingMisshtaC0% (1)
- Analytical CalibrationsDocument19 pagesAnalytical CalibrationsAna Carolina SantosNo ratings yet
- Systematic Reviews of Diagnostic Test Accur - 2018 - Clinical Microbiology and IDocument2 pagesSystematic Reviews of Diagnostic Test Accur - 2018 - Clinical Microbiology and IRadia LachehebNo ratings yet
- Poster TemplateDocument1 pagePoster Templateapi-547372251No ratings yet
- Lot-To-Lot Variation and Verification - cclm-2022-1126Document8 pagesLot-To-Lot Variation and Verification - cclm-2022-1126Georgiana Daniela DragomirNo ratings yet
- IQC Planning ImplementationDocument19 pagesIQC Planning ImplementationYashinta SetyandaNo ratings yet
- A Practical Guide To AnalyticalMV MUDocument12 pagesA Practical Guide To AnalyticalMV MUThippaya Junvee Fortune100% (1)
- ClinicalbertDocument9 pagesClinicalbertZhiyuan LNo ratings yet
- Criteria For Judging Precision and Accuracy in Method Development and EvaluationDocument9 pagesCriteria For Judging Precision and Accuracy in Method Development and EvaluationJustino WaveleNo ratings yet
- NormalValuesandReferenceIntervals TIAFT-Bulletin OhneTurtle 2018-2Document6 pagesNormalValuesandReferenceIntervals TIAFT-Bulletin OhneTurtle 2018-2Sanober JalaliNo ratings yet
- Utility of Shaking Chills As A Diagnostic Sign For Bacteremia in Adults: A Systematic Review and Meta-AnalysisDocument18 pagesUtility of Shaking Chills As A Diagnostic Sign For Bacteremia in Adults: A Systematic Review and Meta-Analysissoy_humanaNo ratings yet
- On Cleaning Validation Recovery Studies: Common MisconceptionsDocument9 pagesOn Cleaning Validation Recovery Studies: Common MisconceptionsMiguel Angel Pacahuala CristobalNo ratings yet
- On Cleaning Validation Recovery Studies: Common MisconceptionsDocument9 pagesOn Cleaning Validation Recovery Studies: Common MisconceptionsMiguel Angel Pacahuala CristobalNo ratings yet
- Resmeth (Bias PPT) Arianne LetadaDocument35 pagesResmeth (Bias PPT) Arianne LetadaHazel BisaNo ratings yet
- Analytical Chemistry and Quality PDFDocument7 pagesAnalytical Chemistry and Quality PDFAbdullah Sabry AzzamNo ratings yet
- 6379-Article Text - 22695-1-10-20191225Document7 pages6379-Article Text - 22695-1-10-20191225JorgeNo ratings yet
- Validity of Prediction Models: When Is A Model Clinically Useful?Document20 pagesValidity of Prediction Models: When Is A Model Clinically Useful?Jesse Helmut Hansen-BartelNo ratings yet
- The Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewFrom EverandThe Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewNo ratings yet
- Palladium-Catalyzed Addition of Diaryl Disulfides and Diselenides To Terminal Alkynes in Room Temperature Ionic Liquids (Document5 pagesPalladium-Catalyzed Addition of Diaryl Disulfides and Diselenides To Terminal Alkynes in Room Temperature Ionic Liquids (SORIN AVRAMESCUNo ratings yet
- Journal of Hazardous MaterialsDocument6 pagesJournal of Hazardous MaterialsSORIN AVRAMESCUNo ratings yet
- 2010 - Formation of Nano Hydroxyapatite CrystalDocument9 pages2010 - Formation of Nano Hydroxyapatite CrystalSORIN AVRAMESCUNo ratings yet
- 42319delta MsiDocument12 pages42319delta MsiSORIN AVRAMESCUNo ratings yet
- 1330 Kashparov Icce 2017 NewDocument38 pages1330 Kashparov Icce 2017 NewSORIN AVRAMESCUNo ratings yet
- 2020 57585 Moesm1 EsmDocument4 pages2020 57585 Moesm1 EsmSORIN AVRAMESCUNo ratings yet
- Asymmetric Alkylation of Malonic Diester Under Phase-Transfer ConditionsDocument5 pagesAsymmetric Alkylation of Malonic Diester Under Phase-Transfer ConditionsSORIN AVRAMESCUNo ratings yet
- Validation of An HPLC Method For Determination of Bisphenol-A PDFDocument7 pagesValidation of An HPLC Method For Determination of Bisphenol-A PDFSORIN AVRAMESCUNo ratings yet
- 1330 HernandezDocument22 pages1330 HernandezSORIN AVRAMESCUNo ratings yet
- Long-Term Field Evaluation of Low-Cost Particulate Matter Sensors in NanjingDocument12 pagesLong-Term Field Evaluation of Low-Cost Particulate Matter Sensors in NanjingSORIN AVRAMESCUNo ratings yet
- Important Polyphenols in Countercurrent Chromatography PDFDocument9 pagesImportant Polyphenols in Countercurrent Chromatography PDFSORIN AVRAMESCUNo ratings yet
- 1330 Ingrid Berger BritoDocument24 pages1330 Ingrid Berger BritoSORIN AVRAMESCUNo ratings yet
- Work Function Based CO Gas Sensing Using Metal Oxide Nanoparticles at Room TemperatureDocument6 pagesWork Function Based CO Gas Sensing Using Metal Oxide Nanoparticles at Room TemperatureSORIN AVRAMESCUNo ratings yet
- ESPR-D-22-21958 Recent Advances On Conducting Polymer Based Magnetic Nanosorbents PDFDocument86 pagesESPR-D-22-21958 Recent Advances On Conducting Polymer Based Magnetic Nanosorbents PDFSORIN AVRAMESCUNo ratings yet
- Journal of Food Engineering: Fangyuan Chen, Alexander D. Warning, Ashim K. Datta, Xing ChenDocument14 pagesJournal of Food Engineering: Fangyuan Chen, Alexander D. Warning, Ashim K. Datta, Xing ChenSORIN AVRAMESCUNo ratings yet
- Artificial Intelligence For Hydrogen-Based Hybrid Renewable Energy Systems: A Review With Case StudyDocument10 pagesArtificial Intelligence For Hydrogen-Based Hybrid Renewable Energy Systems: A Review With Case StudySORIN AVRAMESCUNo ratings yet
- Chemical Engineering Journal: Sylvia Yang Liu, Matthew Ming-Lok Leung, James Kar-Hei Fang, Song Lin ChuaDocument10 pagesChemical Engineering Journal: Sylvia Yang Liu, Matthew Ming-Lok Leung, James Kar-Hei Fang, Song Lin ChuaSORIN AVRAMESCUNo ratings yet
- A Sweet Introduction To The Mathematical Analysis of Time PDFDocument11 pagesA Sweet Introduction To The Mathematical Analysis of Time PDFSORIN AVRAMESCUNo ratings yet
- Important Phytosterols That Are Naturally Present in Commercial Corn Oil PDFDocument5 pagesImportant Phytosterols That Are Naturally Present in Commercial Corn Oil PDFSORIN AVRAMESCU0% (1)
- Bifunctional Superparamagnetic Surface Molecularly Imprinted Polymer PDFDocument3 pagesBifunctional Superparamagnetic Surface Molecularly Imprinted Polymer PDFSORIN AVRAMESCUNo ratings yet
- Determination of Morphine Morphine 3 GluDocument6 pagesDetermination of Morphine Morphine 3 GluSORIN AVRAMESCUNo ratings yet
- Liquid Chromatography Mass SpectrometryDocument50 pagesLiquid Chromatography Mass SpectrometrySORIN AVRAMESCUNo ratings yet
- Development of A Targeted GC MS ScreeninDocument10 pagesDevelopment of A Targeted GC MS ScreeninSORIN AVRAMESCUNo ratings yet
- Preparation of Fatty Acid Methyl EstersDocument9 pagesPreparation of Fatty Acid Methyl EstersSORIN AVRAMESCUNo ratings yet
- Recent NMR Methodological Developments For Chiral Analysis in Isotropic SolutionsDocument33 pagesRecent NMR Methodological Developments For Chiral Analysis in Isotropic SolutionsSORIN AVRAMESCUNo ratings yet
- Drug Analysis by Capillary ElectrophoresDocument14 pagesDrug Analysis by Capillary ElectrophoresSORIN AVRAMESCUNo ratings yet
- Properties of Electrosynthesized Cobalt Doped Zinc Selenide ThinDocument17 pagesProperties of Electrosynthesized Cobalt Doped Zinc Selenide ThinSORIN AVRAMESCUNo ratings yet
- OTC-26384-MS Development and Application of Ultra-High Temperature Drilling Fluids in Offshore Oilfield Around Bohai Sea Bay Basin, ChinaDocument23 pagesOTC-26384-MS Development and Application of Ultra-High Temperature Drilling Fluids in Offshore Oilfield Around Bohai Sea Bay Basin, ChinaSORIN AVRAMESCUNo ratings yet
- Development of A Second Generation AntiDocument32 pagesDevelopment of A Second Generation AntiSORIN AVRAMESCUNo ratings yet
- Peak Deconvolution With Photodiode ArrayDocument2 pagesPeak Deconvolution With Photodiode ArraySORIN AVRAMESCUNo ratings yet
- Accelerated Construction of Urban Intersections With Portlandcement Concrete Pavement (PCCP)Document3 pagesAccelerated Construction of Urban Intersections With Portlandcement Concrete Pavement (PCCP)A-16 RUSHALINo ratings yet
- Construction PlanningDocument198 pagesConstruction PlanningHajarath Prasad AbburuNo ratings yet
- SuperWale Data SheetDocument8 pagesSuperWale Data SheetMagnum CompositesNo ratings yet
- 1 s2.0 S0920586123000196 MainDocument13 pages1 s2.0 S0920586123000196 Mainsofch2011No ratings yet
- Chapter 03 - Louwers 5eDocument23 pagesChapter 03 - Louwers 5eMonique GordonNo ratings yet
- Complete Retro Kenner Action Figure Checklist - ReAction, Warpo, Amok Time, Zica ToysDocument6 pagesComplete Retro Kenner Action Figure Checklist - ReAction, Warpo, Amok Time, Zica ToysJadBeanNo ratings yet
- Object-Oriented Systems Analysis and DesignDocument8 pagesObject-Oriented Systems Analysis and DesignAmar KulkarniNo ratings yet
- CA Level 1Document43 pagesCA Level 1Cikya ComelNo ratings yet
- Regresi OrdinalDocument3 pagesRegresi Ordinalwahyuni salsabilaNo ratings yet
- Ede Micro Project For Tyco StudentsDocument10 pagesEde Micro Project For Tyco StudentsAditya YadavNo ratings yet
- Surekha 4Document11 pagesSurekha 4himanshu kumarNo ratings yet
- Schema Refinement and Normal Forms: Database Management Systems, 3ed, R. Ramakrishnan and J. Gehrke 1Document19 pagesSchema Refinement and Normal Forms: Database Management Systems, 3ed, R. Ramakrishnan and J. Gehrke 1PRADNYA KASHIKARNo ratings yet
- Fixturlaser Documenter User ManualDocument58 pagesFixturlaser Documenter User ManualMicroficheNo ratings yet
- Vietnam SPC - Vinyl Price ListDocument9 pagesVietnam SPC - Vinyl Price ListThe Cultural CommitteeNo ratings yet
- Development of Automated Aerial Pesticide SprayerDocument6 pagesDevelopment of Automated Aerial Pesticide SprayeresatjournalsNo ratings yet
- RTN 29.2023 - 2023 Annual AG Show - 2023 April 27 To April 29Document2 pagesRTN 29.2023 - 2023 Annual AG Show - 2023 April 27 To April 29Anonymous UpWci5No ratings yet
- Mbm-Italien EnuDocument285 pagesMbm-Italien EnuRadwan AL TrougNo ratings yet
- Chapter 1: Scientific Understanding of Behavior: Learning ObjectivesDocument13 pagesChapter 1: Scientific Understanding of Behavior: Learning Objectiveshallo BroNo ratings yet
- Ecm 9Document1 pageEcm 9Misa GamezNo ratings yet
- Carbon Dioxide CO2 SensorDocument4 pagesCarbon Dioxide CO2 SensorgouttNo ratings yet
- Harris Ts100 User ManualDocument24 pagesHarris Ts100 User ManualMiguel Alfonso Ruiz MendezNo ratings yet
- Comparative and Superlative AdjectivesDocument5 pagesComparative and Superlative AdjectivesYoussef BrsNo ratings yet
- 3VA22255HL420AA0 Datasheet enDocument7 pages3VA22255HL420AA0 Datasheet enBensonNo ratings yet
- Business ResearchsampleDocument38 pagesBusiness Researchsamplebasma ezzatNo ratings yet
- Cooling TowerDocument2 pagesCooling TowerLance Darren GalorportNo ratings yet
- Universiti Pendidikan Sultan Idris Mid-Term Test SEMESTER 1 SESSION 2020/2021Document3 pagesUniversiti Pendidikan Sultan Idris Mid-Term Test SEMESTER 1 SESSION 2020/2021rusnah chungNo ratings yet
- Gosat Gs 7055 Hdi FirmwareDocument3 pagesGosat Gs 7055 Hdi FirmwareAntoinetteNo ratings yet





















































































































Download as pdf or txt
You might also like
- Cte-Btvted - Syl-Edtm 158: Disclaimer: Reproduction of This Document Is Allowed SubjectDocument9 pagesCte-Btvted - Syl-Edtm 158: Disclaimer: Reproduction of This Document Is Allowed SubjectGeraldz Brenzon Agustin92% (12)
- GM 1927 01 Project PlanDocument1 pageGM 1927 01 Project Planmark100% (2)
- Expt 2Document7 pagesExpt 2toshgangwarNo ratings yet
- A Calibration Hierarchy For Risk ModelsDocument10 pagesA Calibration Hierarchy For Risk ModelsGuilherme MartheNo ratings yet
- The Kappa Statistic in Reliability Studies - Use, Interpretation, and Sample Size Requirements - Sim & Wright (2005) PDFDocument13 pagesThe Kappa Statistic in Reliability Studies - Use, Interpretation, and Sample Size Requirements - Sim & Wright (2005) PDFEduardo Aguirre DávilaNo ratings yet
- (Surgery (Oxford) 2009-Sep Vol. 27 Iss. 9) - MCQs (2009) (10.1016 - J.mpsur.2009.08.016) - Libgen - LiDocument2 pages(Surgery (Oxford) 2009-Sep Vol. 27 Iss. 9) - MCQs (2009) (10.1016 - J.mpsur.2009.08.016) - Libgen - LiSaleh El BarasiNo ratings yet
- Calibration: The Achilles Heel of Predictive Analytics: Opinion Open AccessDocument7 pagesCalibration: The Achilles Heel of Predictive Analytics: Opinion Open Accessandreitacool23No ratings yet
- Concepto de InertidumbreDocument6 pagesConcepto de InertidumbrePaul Avelino CallupeNo ratings yet
- BM28 1 010101Document10 pagesBM28 1 010101s.aliNo ratings yet
- Treatment of Bias in Estimating Measurement Uncertainty: Gregory E. O'Donnell and D. Brynn HibbertDocument9 pagesTreatment of Bias in Estimating Measurement Uncertainty: Gregory E. O'Donnell and D. Brynn HibbertaureaborosNo ratings yet
- Petersen 2010Document8 pagesPetersen 2010Justino WaveleNo ratings yet
- The Brier Score Does Not Evaluate The Clinical Utility of Diagnostic Tests or Prediction ModelsDocument7 pagesThe Brier Score Does Not Evaluate The Clinical Utility of Diagnostic Tests or Prediction ModelsJoão Pedro RibasNo ratings yet
- Reglas de Predicción ClínicaDocument7 pagesReglas de Predicción ClínicaCambriaChicoNo ratings yet
- CCLM Cyclosporin 18 PDFDocument13 pagesCCLM Cyclosporin 18 PDFSebastian SalinasNo ratings yet
- Assessing The Performance of PredictionDocument11 pagesAssessing The Performance of Predictionmamanpanti00No ratings yet
- Confiabilidad, Precisión o ReproducibilidadDocument9 pagesConfiabilidad, Precisión o ReproducibilidadelderNo ratings yet
- Review: Harmonization of Pre-Analytical Quality IndicatorsDocument9 pagesReview: Harmonization of Pre-Analytical Quality IndicatorsadrianaNo ratings yet
- Reliability, Repeatability and Reproducibility: Analysis of Measurement Errors in Continuous VariablesDocument10 pagesReliability, Repeatability and Reproducibility: Analysis of Measurement Errors in Continuous VariablesGregory GiovanardiNo ratings yet
- Sample Size in Diagnostic Accuracy StudiesDocument9 pagesSample Size in Diagnostic Accuracy StudiesSaurabh AgrawalNo ratings yet
- Ni Hms 438237Document21 pagesNi Hms 438237andreitacool23No ratings yet
- 1 s2.0 S2352551720301621 MainDocument15 pages1 s2.0 S2352551720301621 MainadrianaNo ratings yet
- Incertidumbre Rev MEx Pat Clin 19Document7 pagesIncertidumbre Rev MEx Pat Clin 19Lorena Ek MaciasNo ratings yet
- Clinical Examination For Diagnosing Circulatory Shock: ReviewDocument9 pagesClinical Examination For Diagnosing Circulatory Shock: ReviewAna Cláudia LeiteNo ratings yet
- The European Society of Cardiology Cardio-Oncology Guidelines Evidence Base, Actionability, and Relevance To Clinical PracticeDocument4 pagesThe European Society of Cardiology Cardio-Oncology Guidelines Evidence Base, Actionability, and Relevance To Clinical PracticeCsr ArsNo ratings yet
- Part 16 PDFDocument7 pagesPart 16 PDFKarolina PolskaNo ratings yet
- Twelve Tips For BlueprintingDocument4 pagesTwelve Tips For Blueprintingaatir javaidNo ratings yet
- Methodological Standards For The Development and Evaluation of Clinical Prediction Rules A Review of The LiteratureDocument23 pagesMethodological Standards For The Development and Evaluation of Clinical Prediction Rules A Review of The LiteratureTeoh Cherh YunNo ratings yet
- 10.1515@cclm 2018 1321Document2 pages10.1515@cclm 2018 1321Grescia Ramos VegaNo ratings yet
- 1 s2.0 S0895435615000141 MainDocument10 pages1 s2.0 S0895435615000141 MainBarron ManNo ratings yet
- BMJ I6 FullDocument5 pagesBMJ I6 FullRobertoNo ratings yet
- Jurnal Alin Poct Dipstk UrineDocument9 pagesJurnal Alin Poct Dipstk Urineherlina armarianiNo ratings yet
- GROC Review PDFDocument8 pagesGROC Review PDFPilar BralićNo ratings yet
- Clinical Trials CA WhitepaperDocument14 pagesClinical Trials CA WhitepaperNath ForestNo ratings yet
- Use of Recovery and Bias Information in Analytical Chemistry and Estimation of Its Uncertainty ContributionDocument9 pagesUse of Recovery and Bias Information in Analytical Chemistry and Estimation of Its Uncertainty ContributionRodney SalazarNo ratings yet
- Clinical Practice Guidelines in Breast Cancer: N. Kumar Tyagi and S. Dhesy-ThindDocument10 pagesClinical Practice Guidelines in Breast Cancer: N. Kumar Tyagi and S. Dhesy-ThindsanNo ratings yet
- Improving Healthcare Performance Through Activity-Based Costing and Time-Driven Activity-Based CostingDocument15 pagesImproving Healthcare Performance Through Activity-Based Costing and Time-Driven Activity-Based Costinghasan najiNo ratings yet
- Rating The Quality of Evidence-ImprecisionDocument13 pagesRating The Quality of Evidence-ImprecisionGeorgina CNo ratings yet
- Using Embedding-Based Metrics To Expedite Patients Recruitment Process For Clinical TrialsDocument7 pagesUsing Embedding-Based Metrics To Expedite Patients Recruitment Process For Clinical TrialshousseindhNo ratings yet
- PlebaniDocument2 pagesPlebaniGrescia Ramos VegaNo ratings yet
- 009 Analytical Chemistry at TheDocument8 pages009 Analytical Chemistry at TheRoberto Rolando Bauza FerminNo ratings yet
- BM 27 3 030502Document10 pagesBM 27 3 030502rnbansalNo ratings yet
- Assay Stability, The Missing Component of The Error BudgetDocument9 pagesAssay Stability, The Missing Component of The Error BudgetMezouar AbdennacerNo ratings yet
- cIL Ix1: A Multi-Rule Shewhart Chart For Quality Control in Clinical ChemistryDocument9 pagescIL Ix1: A Multi-Rule Shewhart Chart For Quality Control in Clinical ChemistryJustino WaveleNo ratings yet
- 57 FullDocument6 pages57 Full30. Tyanna Putri MinartiNo ratings yet
- Comparing Treatment Means Overlapping Standard Errors 52odf4albiDocument13 pagesComparing Treatment Means Overlapping Standard Errors 52odf4albiThazin HtayNo ratings yet
- Chapter 17 AuditingDocument48 pagesChapter 17 AuditingMisshtaC0% (1)
- Analytical CalibrationsDocument19 pagesAnalytical CalibrationsAna Carolina SantosNo ratings yet
- Systematic Reviews of Diagnostic Test Accur - 2018 - Clinical Microbiology and IDocument2 pagesSystematic Reviews of Diagnostic Test Accur - 2018 - Clinical Microbiology and IRadia LachehebNo ratings yet
- Poster TemplateDocument1 pagePoster Templateapi-547372251No ratings yet
- Lot-To-Lot Variation and Verification - cclm-2022-1126Document8 pagesLot-To-Lot Variation and Verification - cclm-2022-1126Georgiana Daniela DragomirNo ratings yet
- IQC Planning ImplementationDocument19 pagesIQC Planning ImplementationYashinta SetyandaNo ratings yet
- A Practical Guide To AnalyticalMV MUDocument12 pagesA Practical Guide To AnalyticalMV MUThippaya Junvee Fortune100% (1)
- ClinicalbertDocument9 pagesClinicalbertZhiyuan LNo ratings yet
- Criteria For Judging Precision and Accuracy in Method Development and EvaluationDocument9 pagesCriteria For Judging Precision and Accuracy in Method Development and EvaluationJustino WaveleNo ratings yet
- NormalValuesandReferenceIntervals TIAFT-Bulletin OhneTurtle 2018-2Document6 pagesNormalValuesandReferenceIntervals TIAFT-Bulletin OhneTurtle 2018-2Sanober JalaliNo ratings yet
- Utility of Shaking Chills As A Diagnostic Sign For Bacteremia in Adults: A Systematic Review and Meta-AnalysisDocument18 pagesUtility of Shaking Chills As A Diagnostic Sign For Bacteremia in Adults: A Systematic Review and Meta-Analysissoy_humanaNo ratings yet
- On Cleaning Validation Recovery Studies: Common MisconceptionsDocument9 pagesOn Cleaning Validation Recovery Studies: Common MisconceptionsMiguel Angel Pacahuala CristobalNo ratings yet
- On Cleaning Validation Recovery Studies: Common MisconceptionsDocument9 pagesOn Cleaning Validation Recovery Studies: Common MisconceptionsMiguel Angel Pacahuala CristobalNo ratings yet
- Resmeth (Bias PPT) Arianne LetadaDocument35 pagesResmeth (Bias PPT) Arianne LetadaHazel BisaNo ratings yet
- Analytical Chemistry and Quality PDFDocument7 pagesAnalytical Chemistry and Quality PDFAbdullah Sabry AzzamNo ratings yet
- 6379-Article Text - 22695-1-10-20191225Document7 pages6379-Article Text - 22695-1-10-20191225JorgeNo ratings yet
- Validity of Prediction Models: When Is A Model Clinically Useful?Document20 pagesValidity of Prediction Models: When Is A Model Clinically Useful?Jesse Helmut Hansen-BartelNo ratings yet
- The Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewFrom EverandThe Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewNo ratings yet
- Palladium-Catalyzed Addition of Diaryl Disulfides and Diselenides To Terminal Alkynes in Room Temperature Ionic Liquids (Document5 pagesPalladium-Catalyzed Addition of Diaryl Disulfides and Diselenides To Terminal Alkynes in Room Temperature Ionic Liquids (SORIN AVRAMESCUNo ratings yet
- Journal of Hazardous MaterialsDocument6 pagesJournal of Hazardous MaterialsSORIN AVRAMESCUNo ratings yet
- 2010 - Formation of Nano Hydroxyapatite CrystalDocument9 pages2010 - Formation of Nano Hydroxyapatite CrystalSORIN AVRAMESCUNo ratings yet
- 42319delta MsiDocument12 pages42319delta MsiSORIN AVRAMESCUNo ratings yet
- 1330 Kashparov Icce 2017 NewDocument38 pages1330 Kashparov Icce 2017 NewSORIN AVRAMESCUNo ratings yet
- 2020 57585 Moesm1 EsmDocument4 pages2020 57585 Moesm1 EsmSORIN AVRAMESCUNo ratings yet
- Asymmetric Alkylation of Malonic Diester Under Phase-Transfer ConditionsDocument5 pagesAsymmetric Alkylation of Malonic Diester Under Phase-Transfer ConditionsSORIN AVRAMESCUNo ratings yet
- Validation of An HPLC Method For Determination of Bisphenol-A PDFDocument7 pagesValidation of An HPLC Method For Determination of Bisphenol-A PDFSORIN AVRAMESCUNo ratings yet
- 1330 HernandezDocument22 pages1330 HernandezSORIN AVRAMESCUNo ratings yet
- Long-Term Field Evaluation of Low-Cost Particulate Matter Sensors in NanjingDocument12 pagesLong-Term Field Evaluation of Low-Cost Particulate Matter Sensors in NanjingSORIN AVRAMESCUNo ratings yet
- Important Polyphenols in Countercurrent Chromatography PDFDocument9 pagesImportant Polyphenols in Countercurrent Chromatography PDFSORIN AVRAMESCUNo ratings yet
- 1330 Ingrid Berger BritoDocument24 pages1330 Ingrid Berger BritoSORIN AVRAMESCUNo ratings yet
- Work Function Based CO Gas Sensing Using Metal Oxide Nanoparticles at Room TemperatureDocument6 pagesWork Function Based CO Gas Sensing Using Metal Oxide Nanoparticles at Room TemperatureSORIN AVRAMESCUNo ratings yet
- ESPR-D-22-21958 Recent Advances On Conducting Polymer Based Magnetic Nanosorbents PDFDocument86 pagesESPR-D-22-21958 Recent Advances On Conducting Polymer Based Magnetic Nanosorbents PDFSORIN AVRAMESCUNo ratings yet
- Journal of Food Engineering: Fangyuan Chen, Alexander D. Warning, Ashim K. Datta, Xing ChenDocument14 pagesJournal of Food Engineering: Fangyuan Chen, Alexander D. Warning, Ashim K. Datta, Xing ChenSORIN AVRAMESCUNo ratings yet
- Artificial Intelligence For Hydrogen-Based Hybrid Renewable Energy Systems: A Review With Case StudyDocument10 pagesArtificial Intelligence For Hydrogen-Based Hybrid Renewable Energy Systems: A Review With Case StudySORIN AVRAMESCUNo ratings yet
- Chemical Engineering Journal: Sylvia Yang Liu, Matthew Ming-Lok Leung, James Kar-Hei Fang, Song Lin ChuaDocument10 pagesChemical Engineering Journal: Sylvia Yang Liu, Matthew Ming-Lok Leung, James Kar-Hei Fang, Song Lin ChuaSORIN AVRAMESCUNo ratings yet
- A Sweet Introduction To The Mathematical Analysis of Time PDFDocument11 pagesA Sweet Introduction To The Mathematical Analysis of Time PDFSORIN AVRAMESCUNo ratings yet
- Important Phytosterols That Are Naturally Present in Commercial Corn Oil PDFDocument5 pagesImportant Phytosterols That Are Naturally Present in Commercial Corn Oil PDFSORIN AVRAMESCU0% (1)
- Bifunctional Superparamagnetic Surface Molecularly Imprinted Polymer PDFDocument3 pagesBifunctional Superparamagnetic Surface Molecularly Imprinted Polymer PDFSORIN AVRAMESCUNo ratings yet
- Determination of Morphine Morphine 3 GluDocument6 pagesDetermination of Morphine Morphine 3 GluSORIN AVRAMESCUNo ratings yet
- Liquid Chromatography Mass SpectrometryDocument50 pagesLiquid Chromatography Mass SpectrometrySORIN AVRAMESCUNo ratings yet
- Development of A Targeted GC MS ScreeninDocument10 pagesDevelopment of A Targeted GC MS ScreeninSORIN AVRAMESCUNo ratings yet
- Preparation of Fatty Acid Methyl EstersDocument9 pagesPreparation of Fatty Acid Methyl EstersSORIN AVRAMESCUNo ratings yet
- Recent NMR Methodological Developments For Chiral Analysis in Isotropic SolutionsDocument33 pagesRecent NMR Methodological Developments For Chiral Analysis in Isotropic SolutionsSORIN AVRAMESCUNo ratings yet
- Drug Analysis by Capillary ElectrophoresDocument14 pagesDrug Analysis by Capillary ElectrophoresSORIN AVRAMESCUNo ratings yet
- Properties of Electrosynthesized Cobalt Doped Zinc Selenide ThinDocument17 pagesProperties of Electrosynthesized Cobalt Doped Zinc Selenide ThinSORIN AVRAMESCUNo ratings yet
- OTC-26384-MS Development and Application of Ultra-High Temperature Drilling Fluids in Offshore Oilfield Around Bohai Sea Bay Basin, ChinaDocument23 pagesOTC-26384-MS Development and Application of Ultra-High Temperature Drilling Fluids in Offshore Oilfield Around Bohai Sea Bay Basin, ChinaSORIN AVRAMESCUNo ratings yet
- Development of A Second Generation AntiDocument32 pagesDevelopment of A Second Generation AntiSORIN AVRAMESCUNo ratings yet
- Peak Deconvolution With Photodiode ArrayDocument2 pagesPeak Deconvolution With Photodiode ArraySORIN AVRAMESCUNo ratings yet
- Accelerated Construction of Urban Intersections With Portlandcement Concrete Pavement (PCCP)Document3 pagesAccelerated Construction of Urban Intersections With Portlandcement Concrete Pavement (PCCP)A-16 RUSHALINo ratings yet
- Construction PlanningDocument198 pagesConstruction PlanningHajarath Prasad AbburuNo ratings yet
- SuperWale Data SheetDocument8 pagesSuperWale Data SheetMagnum CompositesNo ratings yet
- 1 s2.0 S0920586123000196 MainDocument13 pages1 s2.0 S0920586123000196 Mainsofch2011No ratings yet
- Chapter 03 - Louwers 5eDocument23 pagesChapter 03 - Louwers 5eMonique GordonNo ratings yet
- Complete Retro Kenner Action Figure Checklist - ReAction, Warpo, Amok Time, Zica ToysDocument6 pagesComplete Retro Kenner Action Figure Checklist - ReAction, Warpo, Amok Time, Zica ToysJadBeanNo ratings yet
- Object-Oriented Systems Analysis and DesignDocument8 pagesObject-Oriented Systems Analysis and DesignAmar KulkarniNo ratings yet
- CA Level 1Document43 pagesCA Level 1Cikya ComelNo ratings yet
- Regresi OrdinalDocument3 pagesRegresi Ordinalwahyuni salsabilaNo ratings yet
- Ede Micro Project For Tyco StudentsDocument10 pagesEde Micro Project For Tyco StudentsAditya YadavNo ratings yet
- Surekha 4Document11 pagesSurekha 4himanshu kumarNo ratings yet
- Schema Refinement and Normal Forms: Database Management Systems, 3ed, R. Ramakrishnan and J. Gehrke 1Document19 pagesSchema Refinement and Normal Forms: Database Management Systems, 3ed, R. Ramakrishnan and J. Gehrke 1PRADNYA KASHIKARNo ratings yet
- Fixturlaser Documenter User ManualDocument58 pagesFixturlaser Documenter User ManualMicroficheNo ratings yet
- Vietnam SPC - Vinyl Price ListDocument9 pagesVietnam SPC - Vinyl Price ListThe Cultural CommitteeNo ratings yet
- Development of Automated Aerial Pesticide SprayerDocument6 pagesDevelopment of Automated Aerial Pesticide SprayeresatjournalsNo ratings yet
- RTN 29.2023 - 2023 Annual AG Show - 2023 April 27 To April 29Document2 pagesRTN 29.2023 - 2023 Annual AG Show - 2023 April 27 To April 29Anonymous UpWci5No ratings yet
- Mbm-Italien EnuDocument285 pagesMbm-Italien EnuRadwan AL TrougNo ratings yet
- Chapter 1: Scientific Understanding of Behavior: Learning ObjectivesDocument13 pagesChapter 1: Scientific Understanding of Behavior: Learning Objectiveshallo BroNo ratings yet
- Ecm 9Document1 pageEcm 9Misa GamezNo ratings yet
- Carbon Dioxide CO2 SensorDocument4 pagesCarbon Dioxide CO2 SensorgouttNo ratings yet
- Harris Ts100 User ManualDocument24 pagesHarris Ts100 User ManualMiguel Alfonso Ruiz MendezNo ratings yet
- Comparative and Superlative AdjectivesDocument5 pagesComparative and Superlative AdjectivesYoussef BrsNo ratings yet
- 3VA22255HL420AA0 Datasheet enDocument7 pages3VA22255HL420AA0 Datasheet enBensonNo ratings yet
- Business ResearchsampleDocument38 pagesBusiness Researchsamplebasma ezzatNo ratings yet
- Cooling TowerDocument2 pagesCooling TowerLance Darren GalorportNo ratings yet
- Universiti Pendidikan Sultan Idris Mid-Term Test SEMESTER 1 SESSION 2020/2021Document3 pagesUniversiti Pendidikan Sultan Idris Mid-Term Test SEMESTER 1 SESSION 2020/2021rusnah chungNo ratings yet
- Gosat Gs 7055 Hdi FirmwareDocument3 pagesGosat Gs 7055 Hdi FirmwareAntoinetteNo ratings yet