Download as pdf or txt
You might also like
- Female Genitalia PDFDocument57 pagesFemale Genitalia PDFElleNo ratings yet
- 3.7 Types of Protein Exam QuestionDocument3 pages3.7 Types of Protein Exam QuestionjnfjngsdjNo ratings yet
- SAE J434 1986 Automotive Ductile Iron Castings Nodular Iron CastingsDocument10 pagesSAE J434 1986 Automotive Ductile Iron Castings Nodular Iron Castingsvinicius_bacellarNo ratings yet
- Cypt CHT Puberty Presentation V1.1enDocument35 pagesCypt CHT Puberty Presentation V1.1enRenz Dela Cruz Arellano100% (1)
- Gynecology Case Discussion History & Clinical Examination: DR - Ketaki Junnare DR - Shweta DR - Priyadarshini Dr. NamrataDocument36 pagesGynecology Case Discussion History & Clinical Examination: DR - Ketaki Junnare DR - Shweta DR - Priyadarshini Dr. Namratapriyadarshini adsulNo ratings yet
- Assessing The BreastDocument37 pagesAssessing The BreastHyacinth Jane Dela PeñaNo ratings yet
- 4.tests To Determine OvulationDocument56 pages4.tests To Determine Ovulationlovelots12340% (1)
- Women'S Health Talk Kozri Lo Lasante Madanm: DR Annabelle D. Marie MO Ministry of Health SeychellesDocument32 pagesWomen'S Health Talk Kozri Lo Lasante Madanm: DR Annabelle D. Marie MO Ministry of Health SeychellesAnna Diana MariaNo ratings yet
- The Sexual Self 2 PDFDocument31 pagesThe Sexual Self 2 PDFAisa Mae EllaNo ratings yet
- Male HealthDocument63 pagesMale Healthminlinguan06No ratings yet
- Presentations of FGMDocument36 pagesPresentations of FGMzuzuyasi65No ratings yet
- History Taking and Physical Examination in GynaecologyDocument41 pagesHistory Taking and Physical Examination in GynaecologygimNo ratings yet
- Uterine ProlapseDocument44 pagesUterine ProlapseMoi Mendoza83% (6)
- Puberty ProblemsDocument38 pagesPuberty ProblemsDapot SianiparNo ratings yet
- The Sexual SelfDocument39 pagesThe Sexual SelfJinkei Jane Negosa100% (1)
- Uts Sexual Behavior and HealthDocument25 pagesUts Sexual Behavior and HealthGrace Ragos RetigNo ratings yet
- Chapter 27 - GU Female SystemDocument13 pagesChapter 27 - GU Female SystemAnnetta AronovaNo ratings yet
- Lesson 101 Reproductive SystemDocument52 pagesLesson 101 Reproductive SystemtheacielaNo ratings yet
- BAGsDocument5 pagesBAGsSalma NazarNo ratings yet
- Module 5 Sexual SelfDocument86 pagesModule 5 Sexual SelfSindac, Maria Celiamel Gabrielle C.No ratings yet
- Delayed Puberty - A Disorder in TimingDocument31 pagesDelayed Puberty - A Disorder in TimingadinayNo ratings yet
- Three Dimensions of Human SexualityDocument26 pagesThree Dimensions of Human SexualityMark Gabriel DomingoNo ratings yet
- Assessing The Genitourinary SystemDocument110 pagesAssessing The Genitourinary SystemHyacinth Jane Dela Peña100% (1)
- UterusDocument18 pagesUterusdeepikanarasimhan1No ratings yet
- Offering Service, Antenatal CareDocument24 pagesOffering Service, Antenatal CareUte DoriNo ratings yet
- Male Female Anatomy ReproductivDocument44 pagesMale Female Anatomy ReproductivWiedNo ratings yet
- Gine 2p - MergedDocument30 pagesGine 2p - MergedHeidy MagañaNo ratings yet
- DAY 7 GenitaliaDocument30 pagesDAY 7 GenitaliaApril Mae Magos LabradorNo ratings yet
- Case Presentation C Section Group 1Document22 pagesCase Presentation C Section Group 1Anthony jesusNo ratings yet
- NSG 123 Module 2Document128 pagesNSG 123 Module 2rigasanaorayNo ratings yet
- Case Presentation (Acute Lymphoblastic Leukemia)Document95 pagesCase Presentation (Acute Lymphoblastic Leukemia)Prativa DhitalNo ratings yet
- Female Reproductive SystemDocument30 pagesFemale Reproductive Systemsaranya amuNo ratings yet
- Reproductive System Power Point Health 2022Document27 pagesReproductive System Power Point Health 2022mrey9839No ratings yet
- Female Reproductive System SlidesDocument30 pagesFemale Reproductive System SlidesNyakie MotlalaneNo ratings yet
- Assessing The Male Genitourinary SystemDocument46 pagesAssessing The Male Genitourinary SystemJonah nyachae100% (1)
- Well Being Woman: Sharing Discussion Approaching Wellness For Every Season of A Woman's LifeDocument52 pagesWell Being Woman: Sharing Discussion Approaching Wellness For Every Season of A Woman's LifeWidya Dwi RahmadhaniNo ratings yet
- Postnatal AssessmentDocument8 pagesPostnatal Assessmentamrutha pkNo ratings yet
- Female Reproductive System: Sexual Health UnitDocument47 pagesFemale Reproductive System: Sexual Health UnitСухоставець Наталія ПетрівнаNo ratings yet
- Health Body A) Puberty: CommonDocument14 pagesHealth Body A) Puberty: CommonMarilyn Castro LaquindanumNo ratings yet
- Product PresentationDocument32 pagesProduct Presentationapi-295416618No ratings yet
- Canvas Sexual SelfDocument17 pagesCanvas Sexual Selfzendaya kim100% (1)
- Girls Booklet gr5 6 enDocument24 pagesGirls Booklet gr5 6 enMariaNo ratings yet
- The Female History & ExamDocument68 pagesThe Female History & Examdanskip1025100% (1)
- Assesment of The Reproductive SystemDocument56 pagesAssesment of The Reproductive SystemSandeep KumarNo ratings yet
- Sexual SelfDocument46 pagesSexual SelfRoxanna Mhae Agarin VidamoNo ratings yet
- Female Infertility: DR Jaqueline Sudiman, PHDDocument21 pagesFemale Infertility: DR Jaqueline Sudiman, PHDGlorio Absalom PuaNo ratings yet
- Midwifery Short NotesDocument552 pagesMidwifery Short NotesChika JonesNo ratings yet
- Adolescent Reproductive and Sexual HealthDocument42 pagesAdolescent Reproductive and Sexual HealthMuhammad Abbas WaliNo ratings yet
- Transgender Patients: From The Transgender Day of Awareness Health EducationDocument15 pagesTransgender Patients: From The Transgender Day of Awareness Health Educationluckyswiss7776848No ratings yet
- Sexual Self2Document39 pagesSexual Self2Larr SumalpongNo ratings yet
- Virginity, Pregnancy and DeliveryDocument65 pagesVirginity, Pregnancy and DeliveryHemanthSairamNo ratings yet
- Caring For The Reproductive SystemDocument15 pagesCaring For The Reproductive SystemMERYL SALOMINA FRANCISCONo ratings yet
- Assessment of The Breast and AxillaeDocument39 pagesAssessment of The Breast and AxillaeKarylle Petil100% (1)
- ChirDocument41 pagesChirSayuridark5No ratings yet
- Liggo NG KabataanDocument33 pagesLiggo NG KabataanChristine VadilloNo ratings yet
- Uterine AnomaliesDocument24 pagesUterine AnomaliesAnaNo ratings yet
- Obstetric History & ExaminationDocument4 pagesObstetric History & ExaminationalifisallahNo ratings yet
- SexualDocument73 pagesSexualKate Angelique RodriguezNo ratings yet
- Chapter 2.2. Sexual-SelfDocument44 pagesChapter 2.2. Sexual-SelfRenier CornelioNo ratings yet
- Preparation For Parenthood: Peggy Korman MA CNM Assistant ProfessorDocument114 pagesPreparation For Parenthood: Peggy Korman MA CNM Assistant ProfessorJyotiNo ratings yet
- Planning and Designing of Bridge Over Solani RiverDocument5 pagesPlanning and Designing of Bridge Over Solani RiverCurious RajNo ratings yet
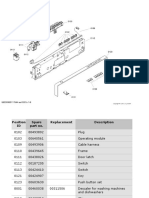
- ΕΓΧΕΙΡΙΔΙΟ ΠΛΥΝΤΗΡΙΟΥ ΠΙΑΤΩΝ - ΑΝΤΑΛΛΑΚΤΙΚΑDocument16 pagesΕΓΧΕΙΡΙΔΙΟ ΠΛΥΝΤΗΡΙΟΥ ΠΙΑΤΩΝ - ΑΝΤΑΛΛΑΚΤΙΚΑΤΣΙΜΠΙΔΗΣ ΠΑΝΑΓΙΩΤΗΣNo ratings yet
- Advanced Earthquake Resistant DesignDocument17 pagesAdvanced Earthquake Resistant Designraju619No ratings yet
- GeneralMathematics11 q1 Mod5b LogarithmicfunctionDocument28 pagesGeneralMathematics11 q1 Mod5b LogarithmicfunctionBrendan Millard Cruda100% (1)
- Utility Request Form (SAP BRP) Revision2Document2 pagesUtility Request Form (SAP BRP) Revision2junaidi100% (1)
- Thrust Block For C12 ZoneDocument6 pagesThrust Block For C12 ZonePrinkle SheteNo ratings yet
- A Guide Book For The Students of Biology (MCAT) : August 2014Document9 pagesA Guide Book For The Students of Biology (MCAT) : August 2014Noor HussainNo ratings yet
- VST Shakti MT 270 Viraat Plus 4WDocument49 pagesVST Shakti MT 270 Viraat Plus 4Wbharath100% (1)
- Final Dayak PDFDocument25 pagesFinal Dayak PDFKevin Marco100% (1)
- Din en Iso 1302Document51 pagesDin en Iso 1302Akshay Patil100% (1)
- Jan 24 Homework Solutions Math 151, Winter 2012 Chapter 3 Problems (Pages 102-110)Document7 pagesJan 24 Homework Solutions Math 151, Winter 2012 Chapter 3 Problems (Pages 102-110)Pei JingNo ratings yet
- The Art of Living in WartimeDocument284 pagesThe Art of Living in WartimeMonsta XNo ratings yet
- 5WG1527 1AB41 Siemens PDFDocument2 pages5WG1527 1AB41 Siemens PDFsamim_khNo ratings yet
- Aereal PhotogrammetryDocument13 pagesAereal PhotogrammetryJuan GarzonNo ratings yet
- Isopropyl Alcohol Solution 91, 400682 - HLK - SDSDocument7 pagesIsopropyl Alcohol Solution 91, 400682 - HLK - SDSAman BaigNo ratings yet
- Physic Lab Report 6: Sherry Carentona GalinDocument6 pagesPhysic Lab Report 6: Sherry Carentona GalinNurl AinaNo ratings yet
- Summer Training Report On: "Consumer Perception Towards Online Shopping"Document83 pagesSummer Training Report On: "Consumer Perception Towards Online Shopping"Swati TanwarNo ratings yet
- Lista Noviembre16Document10 pagesLista Noviembre16Avraham ZentliNo ratings yet
- NN ST661 (CPH)Document42 pagesNN ST661 (CPH)Patrice PaulNo ratings yet
- RedoDocument1 pageRedogmpzgamerNo ratings yet
- GRI 180-12-B-W1K Data SheetDocument3 pagesGRI 180-12-B-W1K Data SheetJMAC SupplyNo ratings yet
- Personality Development Module #3 Assessment: Best Describes Each ItemDocument2 pagesPersonality Development Module #3 Assessment: Best Describes Each ItemAshierah MontasNo ratings yet
- Creutzfeldt-Jakob DiseaseDocument18 pagesCreutzfeldt-Jakob DiseaseJussel Vazquez MarquezNo ratings yet
- Agri Sample Csec Ag Sci Sba Crop Livestock Investigative Projects - 05.06.2017 3Document53 pagesAgri Sample Csec Ag Sci Sba Crop Livestock Investigative Projects - 05.06.2017 3Shakwan Waterman100% (1)
- Ground Floor Plan: Nitin SidhpuraDocument14 pagesGround Floor Plan: Nitin SidhpuraRam PatelNo ratings yet
- Foxboro Evo™ Process Automation System: Product SpecificationsDocument12 pagesFoxboro Evo™ Process Automation System: Product SpecificationsSukdeb MaityNo ratings yet
- Lesson 1: Physical Fitness Fitt PrinciplesDocument2 pagesLesson 1: Physical Fitness Fitt PrinciplesJamaica JaneNo ratings yet
- Observation Report: Analytical ChemistryDocument8 pagesObservation Report: Analytical ChemistryLindsay BulgerNo ratings yet