Professional Documents
Culture Documents
PD - Examination of The Eye
PD - Examination of The Eye
Uploaded by
John TecsonOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
PD - Examination of The Eye
PD - Examination of The Eye
Uploaded by
John TecsonCopyright:
Available Formats
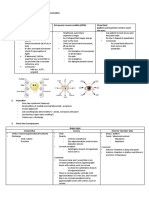
Examination of the Eye • Tear fluid
Overview: o Protects the conjunctiva and cornea from drying
o Review of Anatomy and Physiology o Inhibits microbial growth
o History Taking: o Gives a smooth optical surface to the cornea
▪ Preliminary Data o Comes from the:
▪ Chief Complaints ▪ Meibomian gland
▪ History of Presenting Illness ▪ Conjunctival glands
▪ Negative History ▪ Lacrimal gland
▪ Treatment History (for presenting illness) o Spreads across the eye and drains medially through
▪ Past History two tiny holes (lacrimal puncta)
▪ Personal History o Pathway:
▪ Family History → Either of the three glands
o Important Areas of Examination → Lacrimal puncta (lies atop the small elevation
o Procedures and the Associated Abnormalities of the medial lower lid medially)
o Ophthalmoscopic Examination → Lacrimal sac (rests in a small depression
inside the bony orbit, not visible)
Anatomy and Physiology of the Eye → Nasolacrimal duct
• Lacrimal gland
o Lies mostly
within the
bony orbit,
superior and
lateral to the
eyeball
• Eyeball
o Spherical
structure
o Focuses light
on the
neurosensory
elements
within the
retina
• Palpebral fissure • Muscles of the iris
o Opening between the eyelids o Control
• White sclera pupillary size
o Buff-colored at its periphery • Muscles of the ciliary
• Conjunctiva body
o A clear mucous o Control the thickness of the lens
membrane with two o Allows the eye to focus on near or distant objects
easily visible • Aqueous humor
components o Clear fluid that fills the anterior and posterior chambers
o Bulbar conjunctiva of the eye
▪ Covers most o Produced by the ciliary body
of the o Circulates from the posterior chamber through the
anterior pupil → anterior chamber → drains out through the
eyeball canal of Schlemm
▪ Adheres o Function: helps to control pressure inside the eye
loosely to
the tissue
▪ Meets the
cornea at
the limbus
o Palpebral
conjunctiva
▪ Lines the
eyelids
o These two merge in a
folded recess that
permits the eyeball movement.
• Tarsal plates
o Firm strips of connective tissue that lie within the eyelids
o Each contains meibomian glands (opens on the lid
margin)
• Levator palpebrae
o Muscle that raises the upper eyelid • Optic fundus
o Innervated by the oculomotor nerve (CN III) o Posterior portion of the eye
o Note: smooth muscle – innervated by sympathetic o Seen through the ophthalmoscope
nervous system → lid elevation o Structures:
▪ Retina
▪ Choroid
▪ Fovea
[AFGC] Checked by: [Transhead] Page 1 of 8
Physical Diagnosis
▪ Macula
▪ Optic disc
▪ Retinal vessels
• Optic nerve (along with its retinal vessels)
o Enters the eyeball posteriorly
o Located at the optic disc (visible through the
ophthalmoscope)
• Optic disc
o Contains the optic nerve
o Lateral and slightly inferior to this disc lies a small
depression in the retinal surface which marks the point
of central vision
• Fovea (a.k.a. Central Fovea/ fovea centralis)
o Darkened circular area (point of central vision)
• Macula
o Roughly circular
o Surrounds the fovea
o No discernable margins Visual Pathways
• Vitreous body
o Transparent mass of gelatinous material
o Fills the eyeball behind the lens
o Helps to maintain the shape of the eye
• To see an image, light reflected from the target must:
o pass through the pupil and;
o be focused on photoreceptors of the retina
• Image projected on the photoreceptors – upside down and
reversed right to left
• An image from the upper nasal visual field strikes the lower
temporal quadrant of the retina
• Nerve impulses, stimulated by light, are conducted through the
following:
→ Retina
→ Optic nerve (CN II)
→ Optic tract on each side
Visual Fields → Optic radiation (curving tract)
• It is the entire area seen by an eye when it looks at a central point o Visual cortex – part of the occipital lobe, where the
• Diagrammed on circles from the patient’s point of view nerve impulses end
• The center of the circle represents the focus of gaze.
• Circumference from the line of gaze: 90° Pupillary Reactions
• Each visual field is divided into 4 quadrants (white areas, see photo • Pupillary size changes in response to light and to the effort of
below) focusing on a near object.
• Light reactions
1. Direct light reaction
▪ Pupillary constriction of both eyes, when a
light beam shines onto one retina
2. Consensual light reaction
▪ Pupillary constriction in contralateral eye,
when a light beam shines onto one retina
o Initial sensory pathways are similar with the vision:
▪ Retina → optic nerve (CN II) → optic tract
▪ Diverges in the midbrain
▪ Oculomotor nerve (CN III) – transmits
impulses back to the constrictor muscles of the
• Fields extend farthest on the temporal sides iris
• Visual fields are normally limited by the:
o Brows above
o Cheeks below
o Nose medially
• Lack of retinal receptors at the optic disc → oval blind spot in the
normal field of each eye (15° temporal to the line of gaze)
• The use of both eyes produces a binocular vision wherein the two
visual fields overlap.
o Laterally, vision is mononuclear.
[AFGC] Checked by: [Transhead] Page 2 of 8
Physical Diagnosis
Extraocular Movements
• Six muscles that control the eye:
o 4 rectus muscles
o 2 oblique muscles
• To test the function of each muscle and its CN innervation:
o Ask the patient to move the eye in the direction controlled
by that muscle
• Six Cardinal Directions (see image below):
• Example of abnormality:
o Diplopia (double vision)
▪ Damaged CN IV (trochlear nerve) due to head
trauma, congenital causes or central lesions
▪ Causes dysfunction of the superior oblique
muscle
• Near Reaction
o pupil constricts when a person shifts gaze from a far
object to a near object.
o Mediated by the oculomotor nerve (CN III)
o Coincident but not part of the pupillary constriction: HISTORY TAKING
▪ Convergence of the eyes (medial rectus
movement) Preliminary Data
▪ Accommodation – increased convexity of the
• Name
lenses caused by contraction of the ciliary
• Age/sex
muscles (near objects are more focused)
• Address
• Occupation
• Date of Admission
Chief Complaints
• Chief complaints should be in Patient’s words.
• They should be in a chronological order.
Autonomic Nerve Supply to the Eyes o i.e., the one which appeared first in timeline should be
written first.
• Parasympathetics
• Diminution of vision in left eye since last 2 years
o Fibers travelling in the oculomotor nerve (CN III) and
produces pupillary constriction • Watering in left eye since last 1 year
• Sympathetics • Pain in both eyes since last 6 months
o Pupillary dilation and raising of upper eyelid (superior
tarsal muscle) History of Present Illness
o This pathway starts in the hypothalamus → down • Describe all the chief complaints.
through the brainstem and cervical cord → neck → • Example: Diminution of vision can be described under the following
carotid artery/its branches → orbit heads:
o Onset
▪ lesion on this pathway → may impair
o Duration
sympathetic effects that dilate the pupil
o Progression
o Pattern
• Pain can also be described under the following heads: (OLD
CARTS)
o Onset
o Location
o Duration
o Character
o Aggravating factors
o Relieving factors
o Time
o Severity
• The patient was apparently well (TIME), back when he/she started
having pain in the (LOCATION). The pain is (CHARACTER), and
aggravated on ________ and is relieved by _______. It is
continuous/intermittent etc.
• Subsequently, he/she also started having diminished vision in the
left eye. It was constant in nature, and more for long distances
than near distance. It is progressing.
Negative History
• Rule out factors
• Ask for history of:
o Trauma
o Discharge
[AFGC] Checked by: [Transhead] Page 3 of 8
Physical Diagnosis
o Floaters o Patient unable to read the largest letter may be
o Redness on white of eye positioned closer to the chart (note the intervening
o White on black of eye distance).
o Insensitivity to light (Photophobia) o Identify the smallest line of print where the patient can
o Glare identify more than half the letters
o Halos o Record the visual acuity designated at the side of this
o Painful movement of eye line, along with use of glasses (if any).
o Flashes of light • Expressed as two (2) numbers
• Micropsia, macropsia o Example: 20/30
▪ 20 – indicates the distance of the patient from
Treatment History the chart
• Ask if the patient has taken any treatment for the presenting ▪ 30 – distance at which a normal eye can read
illness. the line of letters
• This is important because sometimes a physician has tried first line • Hand-held card
of drugs and then the patient comes to you, it gives you liberty to o Used for testing near vision
directly use second line drugs. o Help identify the need for reading glasses or bifocals in
patient >45 years old.
Past History o Can be used for testing visual acuity at bedside
• It is divided into four heads: o Held 14 inches from the patient’s eyes
o Ocular Medical • Example of abnormalities:
▪ Ask about any previous disease of the eye and o Vision of 20/200
medications take for it. ▪ Means at 20 feet the patient can read print that
o Ocular Surgical a person with normal vision can read at 200
▪ Ask if the patient has undergone any ocular feet.
surgeries before. ▪ Larger the second number, the worse the
▪ If Yes, take detailed history of that surgery. vision.
o Systemic Medical ▪ 20/40 corrected – means the patient could
▪ Ask patient about any significant systemic read the 20/40 line with glasses
disease that he/she has. o Myopia (nearsightedness)
o Systemic Surgical ▪ Causes focusing problems for distance vision
▪ Any surgeries in the past. o Presbyopia
• Ask the patient if the patient has the following diseases: ▪ Causes focusing problems for near vison
o Diabetes Mellitus ▪ Middle-aged and older adults
o Hypertension ▪ Sees better when the card is farther away.
o Ischemic Heart Disease • If there’s no chart → screen visual acuity with any available print
o Tuberculosis • If patient can’t read even the largest letters → test ability to count
o Bronchial Asthma your upraised fingers and distinguish light from the dark
o Drug Allergies • Legal blindness
o Results from a constricted field of vision: 20° or less in
Personal History the better eye
• Ask for: o In the U.S., a person is considered legally blind when
o Bowel and bladder movement vision on the better eye, corrected with glasses is 20/200
o Currently on any medications or not or less.
o Addictions
o Diet Visual Fields by Confrontation
o Menstrual History
• A valuable screening technique for detection of lesions in the
Family History anterior and posterior visual pathway.
• Genetic diseases • To achieve best results, two tests are recommended:
• Hereditary diseases o Static finger wiggle test
o Kinetic red target test
• Diseases that run in the family
• Humphrey visual field
• Ask for any history of the following diseases in the family:
o Definitive diagnosis of a visual field
o Squint
• Causes of anterior pathway defects:
o Congenital cataract
o Glaucoma
o Ptosis
o Optic neuropathy
o Glaucoma
o Optic neuritis
o Glioma
EXAMINATION AND TECHNIQUES • Causes of posterior pathway defects:
o Stroke
Important Areas of Examination o Chiasmal tumors
• Visual acuity • Field defects (all or partly temporal):
• Visual fields
• Conjunctiva and sclera
• Cornea, lens and pupils
• Extraocular movements
• Fundi, including: optic disc and cup, retina, and retinal vessels
Visual Acuity
• Procedure:
o Use a well-lit Snellen chart
o Position patient 20 feet from the chart
o Patients wearing glasses other than for reading should
put them on.
o Ask patient to cover one eye with a card
▪ To prevent looking through the fingers
o Ask the patient to read smallest print possible
[AFGC] Checked by: [Transhead] Page 4 of 8
Physical Diagnosis
Static Finger Wiggle Test o Adequacy of eyelid closure
• Procedure: ▪ Failure of the eyelids to close exposes the
o Position yourself about corneas to serious damage
an arm’s length away
from the patient Lacrimal Apparatus
o Close one eye and • Briefly inspect the regions of the lacrimal gland and lacrimal sac for
have the patient cover swelling.
the opposite eye while • Check for excessive tearing or dryness of the eyes.
staring at your open • Assessment of dryness may require special testing
eye o Sjögren syndrome – impaired secretion
o Place you hands about • Excessive tearing maybe from:
2 feet apart out of the o increased production caused by:
patient’s view, lateral ▪ Conjunctival inflammation
to the patient’s ears. ▪ Corneal irritation
o While in this position, wiggle your fingers and slowly o Impaired drainage caused by:
bring your moving fingers forward into the patient’s ▪ Ectropion
center of view ▪ Nasolacrimal duct obstruction
o Ask the patient to tell you as soon as he/she sees your
finger movement.
o Test each clock hour or at least each quadrant. Conjunctiva and Sclera
o Test each eye individually • Procedure:
o Record the extent of visits in each area o Ask patient look up as you depress both lower lids with
o Note any abnormal “field cuts” your thumbs
o Inspect the sclera and palpebral conjunctiva for color
• Example of abnormality: o Note vascular pattern against the white scleral
o Left Homonymous hemianopsia background
▪ Patient’s left eye repeatedly does not see your o Look for any nodules or swelling
fingers until they have crossed the line of gaze o For a fuller view of the eye:
▪ Diagrammed from the patient’s viewpoint: (see ▪ Rest your thumb on the cheekbones and
image below) finger on the brows
▪ Spread the lids
o Ask the patient to look each side and down
▪ For a clearer view of the sclera and bulbar
conjunctiva of the upper lid
▪ For the palpebral conjunctiva of the upper lid –
evert the lid
Kinetic Red Target Test • Jaundice – yellow sclera
• Procedure:
o Facing the patient, move a 5-mm red-topped pin inward Nodular episcleritis
from beyond the boundary of each quadrant along a line - Local redness
bisecting the horizontal and vertical meridians - Also seen in RA
o Ask the patient when the pin first appears to be red. and SLE
• Enlarged blind spot occurs in conditions that affect the optic
nerve:
o Glaucoma
o Optic neuritis
o Papilledema Cornea and Lens
• Procedure:
Position and Alignment of the Eyes o Inspect the cornea of each eye for opacities (use
• Procedure: oblique lighting)
o Stand in front of the patient
o Survey the eyes for position and alignment Iris
o If one or both eyes seem to protrude, assess them from • Same time with the inspection of the cornea and lens
above. • Markings should be clearly defined
• Shine light directly from the temporal side
Eyebrows o Look for a crescentic shadow (abnormal) on the medial
• Inspect the eyebrows and note the following: side of the iris
o Fullness ▪ Narrow angle increases the risk for acute
o Hair distribution narrow-angle glaucoma – sudden increase
o Any scaliness of the underlying skin in IOP when aqueous humor drainage is
▪ Occurs in seborrheic dermatitis, lateral blocked
sparseness in hypothyroidism o Normal: iris is fairly flat and forms an open angle with the
cornea – lighting casts no shadow
Eyelids • Open-angle glaucoma
o Common form of glaucoma
• Note the position of the lids o The normal spatial relation between the iris and cornea
• Inspect for the following: is preserved and the iris is fully lit
o Width of the palpebral fissures
▪ Upslanting palpebral fissure – Down
Syndrome
o Edema of the lids
o Color of the lids
▪ Blepharitis – red inflamed lid margins which
often occur with crusting
o Lesions
o Condition and direction of the eyelashes
[AFGC] Checked by: [Transhead] Page 5 of 8
Physical Diagnosis
Pupils o Asses the EOMs, look for:
• Procedure: 1) Normal conjugate movements of the eyes in
o In a dim light, inspect both pupils for the following: each direction
▪ Size - Note any deviation/ dysconjugate gaze
▪ Shape ▪ Nystagmus – fine rhythmic oscillation of the
▪ Symmetry eyes
o Measure the pupils with a card showing black circles of - Normal: A few beats on extreme lateral
varying sizes, test the light reaction gaze (bring finger in to within the field of
o Note if pupils are: binocular vision)
▪ Large – > 5mm ▪ Lid lag – as the eyes move from up and down
▪ Small – < 3mm - In hyperthyroidism – a rim of sclera is
▪ Unequal visible above the iris with downward gaze
• Cover-uncover test
o May reveal a slight or latent muscle imbalance, not
otherwise seen
o Useful in examining children
• Sustained nystagmus within the binocular field of gaze:
• Miosis – refers to constriction of pupils o Congenital disorders
• Mydriasis – dilation of pupils o Labyrinthitis
• Simple anisocoria o Cerebellar disorders
o Difference in pupillary diameter 0.4mm or greater without o Drug toxicity
a known pathologic cause • Test Six EOMs
o Benign if it is equal in dim and bright light and there is o Ask the patient to follow your finger or pencil as you
brisk pupillary constriction to light (light reaction) sweep through the six cardinal directions of gaze.
o Making a wide H in the air, lead the patient’s gaze:
Light Reaction 1) To patient’s extreme right,
2) To the right and upward and,
• Done in dim light
3) Down on the right; then
• Procedure:
4) Without pausing in the middle, to the extreme
o Ask patient to look into distance
left,
o Shine a bright light obliquely into each pupil in turn
5) To the left and upward, and
o Both the distant gaze and oblique lighting help to prevent
6) Down on the left
a near reaction
o To detect Nystagmus – Pause during upward and
o Look for:
lateral gaze
▪ Direct reaction – pupillary constriction of the
o Move finger or pencil at a comfortable distance from the
same eye
patient.
▪ Consensual reaction – pupillary constriction
o Increase distance – middle-aged or older adults as they
of the opposite eye
may have difficulty focusing on near objects
o Always darken the room and use a bright light
o Hold the head – should be in the proper midline
(especially useful if patient
Near Reaction
tends to follow with their head)
• If light reaction is impaired or questionable → test the near reaction o CN VI paralysis (right)
in both dim and normal light ▪ Eyes are conjugated
• Test one eye at a time in right lateral gaze
o Easier to concentrate on pupillary responses, without the but not in left lateral
distraction of the EOM gaze
• Procedure:
o Hold you finger or pencil 10 cm from the patient’s eye
o Ask the patient to look alternately at it and into the
distance directly behind it
o Watch for pupillary constriction with near effort and
convergence of the eyes • If lid lag or hyperthyroidism is suspected,
o Accommodation of the lens that brings near object into o Ask patient to follow your finger again as you move it
focus is not visible slowly from up to down in the midline
• Helpful in diagnosing Argyll Robertson and tonic (Adie) pupils o Normal: upper eyelid overlaps the iris slightly throughout
the movement (left image below)
Extraocular Muscles o Abnormal: Proptosis – rim of sclera is visible (right image)
▪ It is an abnormal protrusion of the eyeballs in
hyperthyroidism
▪ “stare” on frontal gaze
▪ If unilateral – orbital tumor or retrobulbar
hemorrhage from trauma may be suspected
• Procedure:
o Stand 2 feet directly in front of the patient
o Shine a light into the patient’s eyes
o Ask patient to look at it
o Inspect the light reflection in the corneas
1) Should be visible slightly nasal to the center of
the pupils
[AFGC] Checked by: [Transhead] Page 6 of 8
Physical Diagnosis
• Test for Convergence (if near reaction test has not been done) • Hold the ophthalmoscope firmly braced against the medial aspect
o Ask the patient to follow your finger or pencil as you of your bony orbit, with the handle tilted laterally at about a 20-
move it in toward the bridge of the nose. degree slant from the vertical.
o Normal: Converging eyes follow the object to within 5 cm o Check to make sure you can see clearly through the
to 8 cm of the nose aperture.
o Poor in hyperthyroidism o Instruct the patient to look slightly up and over your
shoulder at a point directly ahead on the wall.
• Place yourself about 15 inches away from
the patient and at an angle 15 degrees
lateral to the patient’s line of vision.
o Shine the light beam on the
pupil and look for the orange
glow in the pupil—the red reflex.
o Note any opacities interrupting
Ophthalmoscopic Examination the red reflex.
• Examining patient’s eyes without ▪ Absence of Red
dilating their pupils can obscure Reflex – opacities of
important neurologic findings. the lens (cataracts) or
o View becomes limited to possibly of the
the posterior structures vitreous
of the retina - Less commonly
• Refer the patient to an seen in detached retina/ in children with
ophthalmologist, for pupillary retinoblastoma
dilatation with mydriatic drops. - Artificial eye has no red reflex
o To see more peripheral • Now, place the thumb of your other hand across the patient’s
structures eyebrow.
o To evaluate the macula o helps keep you steady but is not essential
well • Keeping the light beam focused on the red reflex, move in with the
o To investigate ophthalmoscope on the 15-degree angle toward the pupil until you
unexplained visual loss are very close to it, almost touching the patient’s eyelashes.
• Contraindications for mydriatic drops:
o Head injury and coma • Try to keep both eyes open and relaxed, as if gazing into the
▪ observation of pupillary reaction should be distance
continuous o help minimize any fluctuating blurriness as your eyes
o any suspicion of narrow-angle glaucoma attempt to accommodate.
• PanOptic Ophthalmoscope • You may need to lower the brightness of the light beam
o Allows clinician to view the retina, even when the pupils o make the examination more comfortable for the patient,
are undilated o avoid hippus (spasm of the pupil)
o Provides a five-fold greater view of the fundus o improve your observations.
o Enables 25° field of view
o Increases the examining distance between patient and Steps for Examining the Optic Disc and the Retina
clinician Optic Disc – round, yellow-orange to creamy pink structure with a pink
• Visualizing the fundus via a traditional ophthalmoscope neuroretinal rim and central depression that often takes practice to
o One of the most challenging skills of PE locate (diameter: 1.5mm)
o One of the most critical when assessing headache and
changes in mental status
o Remove your glasses unless you are nearsighted or has
severe astigmatism or your refractive error makes it
difficult to see the fundi.
Steps for Using an Ophthalmoscope
• Darken the room. • Look for the optic disc (see description above)
• Switch on the ophthalmoscope light and turn the lens disc until you o You may follow the blood vessel centrally until it enters
see the large round beam of white light. the disc.
• Shine the light on the back of your hand to check the type of light, o Blood vessels becomes progressively larger at each
its desired brightness, and the electrical charge of the branch point as you approach the disc.
ophthalmoscope. • Bring the optic disc into sharp focus by adjusting the lens of
• Turn the lens disc to the 0 diopter. your ophthalmoscope.
o A diopter is a unit that measures the power of a lens to o If both you and the patient have no refractive errors, the
converge or diverge light. retina should be in focus at 0 diopters.
o At this diopter, the lens neither converges nor o Blurred structures – rotate the lens disc until you find
diverges light. the sharpest focus.
o Keep your finger on the edge of the lens disc so you can o Myopic (nearsighted) – rotate the lens disc
turn the disc to focus the lens when you examine the counterclockwise to the minus diopters;
fundus. o Hyperopic (farsighted) patient – move the disc
• Hold the ophthalmoscope in your right hand and use your right eye clockwise to the plus diopters.
to examine the patient’s right eye; hold it in your left hand and use o You can correct your own refractive error in the same
your left eye to examine the patient’s left eye. way.
o To prevent you from bumping the patient’s nose and • Inspect the optic disc. Note the following features:
gives you more mobility and closer range for visualizing o Sharpness or clarity of the disc outline.
the fundus. ▪ Normal: nasal portion of the disc margin may
o At first, you may have difficulty using your nondominant be somewhat blurred
eye, but this will abate with practice. o Color of the disc
▪ Normal: yellowish orange to creamy pink.
White or pigmented crescents may ring the
disc
[AFGC] Checked by: [Transhead] Page 7 of 8
Physical Diagnosis
o Size of the central physiologic cup, if present.
▪ yellowish white
▪ horizontal diameter is usually less than half the
horizontal diameter of the disc.
o Comparative symmetry of the eyes and findings in
the fundi.
• If the lens have been surgically removed:
o Magnifying effect is lost
o Retinal structures will look smaller than usual
o Larger expanse of the fundus
Detecting Papilledema
• It is the swelling of the optic disc and • Inspect the fovea and surrounding macula.
anterior bulging of the physiologic o Direct your light beam laterally or by asking the patient to
cup. look directly into the light.
• Increased intracranial pressure → o Tiny bright reflection at the center of the fovea helps to
transmitted to the optic nerve orient you (younger people);
causing: ▪ shimmering light reflections in the macular
o stasis of axoplasmic flow area are common.
o intra-axonal edema
o swelling of the optic nerve
head.
• signals serious disorders of the
brain:
o meningitis
o subarachnoid hemorrhage
o trauma
o mass lesions
• Searching for this important disorder is a priority during all your
funduscopic examinations.
• Inspect the fundus for spontaneous venous pulsations (SVPs)
o rhythmic variations in the caliber of the retinal veins as
they cross the fundus
o narrower in systole; wider in diastole
o 90% of normal patients. • Inspect the anterior structures.
• Loss of SVPs o Look for opacities in the vitreous or lens.
o occurs with high intracranial pressures (above 190 o Rotate the lens disc progressively to diopters of around
mm H2O) that change the pressure gradient between +10 or +12, so you can focus on the more anterior
cerebral spinal fluid pressure and intraocular pulse structures in the eye.
pressure in the optic disc • Macular degeneration
o important cause of poor central vision in older adults.
The Retina—Arteries, Veins, Fovea, and Macula o Types:
▪ dry atrophic (more common but less severe)
• Inspect the retina, including: ▪ wet exudative (neovascular)
o arteries and veins (as they extend to the periphery) o Drusen – undigested
o arteriovenous crossings
cellular debris
o fovea ▪ may be hard
o macula
and sharply
• Distinguish arteries from veins based on the features listed below. defined, as
seen below, or
Arteries Veins soft and
Color light red Dark red confluent with
Size Smaller Larger altered
(2⁄4 to 3⁄4 the pigmentation
diameter of veins)
Light Reflex Bright Inconspicuous or • Vitreous floaters
(reflection) absent o seen as dark specks or strands between the fundus and
the lens
• Follow the vessels peripherally in each of four directions. Note the • Cataracts – densities in the lens
following:
o relative sizes
o character of the arteriovenous crossings. References:
• Identify any lesions of the surrounding retina. Note the following:
• Bate’s Guide to Physical Examination and History Taking (11th &
o Size
12th)
o Shape
• PPT (History Taking)
o Color
o Distribution
• As you search the retina, move your head and instrument as a unit,
using the patient’s pupil as an imaginary fulcrum.
• At first, you may lose your view of the retina because your light falls
out of the pupil. You will improve with practice.
• Lesions of the retina – measured in terms of “disc diameters”
from the optic disc.
o Cotton-wool patches – are irregular patches
[AFGC] Checked by: [Transhead] Page 8 of 8
You might also like
- Muscle ChartDocument16 pagesMuscle Chartphinee1693% (14)
- Pcog Answer KeyDocument7 pagesPcog Answer KeyJohn Tecson100% (2)
- Top 200 Sorted by Drug ClassDocument3 pagesTop 200 Sorted by Drug Classthompjo2394100% (7)
- Heent ScriptDocument4 pagesHeent ScriptJohn TecsonNo ratings yet
- Answers Orgmed Post TestDocument9 pagesAnswers Orgmed Post TestJohn TecsonNo ratings yet
- Aborigines and Native Americans - A Compare and Contrast EssayDocument6 pagesAborigines and Native Americans - A Compare and Contrast Essaytwihard9360% (5)
- Maternal and Child NCLEX QuestionsDocument3 pagesMaternal and Child NCLEX QuestionsShengxy Ferrer100% (2)
- Auto PEEPDocument9 pagesAuto PEEPJoãoBrasil100% (1)
- 3.1 Anatomy and Physiology of The Eye - Nov. 3 - Dr. CastilloDocument13 pages3.1 Anatomy and Physiology of The Eye - Nov. 3 - Dr. CastilloHanako Sasaki AranillaNo ratings yet
- Special SensesDocument8 pagesSpecial SensesGiane Qeirr Osias TimmalogNo ratings yet
- Anatomy of The Eye - Dr. Lim-Cecilio (2022)Document3 pagesAnatomy of The Eye - Dr. Lim-Cecilio (2022)Patricia ManaliliNo ratings yet
- A&P - 11. Vision, Taste & Smell (15p)Document15 pagesA&P - 11. Vision, Taste & Smell (15p)Gabriel StratulatNo ratings yet
- 1group 1 - Compiled Topics-MergedDocument376 pages1group 1 - Compiled Topics-Mergedwhiskers qtNo ratings yet
- Ophthalmology Final TransDocument51 pagesOphthalmology Final TransPatryk Dionisio100% (1)
- Histology of The Eye Lectured By: Dr. Gonzales Transcribed By: Angelo Louise A. Sayo Proofread By: Kaye Reyes & Erina ValdesDocument12 pagesHistology of The Eye Lectured By: Dr. Gonzales Transcribed By: Angelo Louise A. Sayo Proofread By: Kaye Reyes & Erina ValdesKaye NeeNo ratings yet
- Sensory Disorders Orthopedic NursingDocument10 pagesSensory Disorders Orthopedic Nursingannbautista.infoNo ratings yet
- Eent CompiledDocument15 pagesEent CompiledAlthea Franz DuoNo ratings yet
- Chapter 8 Special SensesDocument5 pagesChapter 8 Special SensesEdralyn EgaelNo ratings yet
- OPTHALMOLOGYDocument17 pagesOPTHALMOLOGYSofia P. PanlilioNo ratings yet
- OPTHA 1.1 ANATOMY OF THE EYEBALL - Dr. CapuchinoDocument4 pagesOPTHA 1.1 ANATOMY OF THE EYEBALL - Dr. CapuchinoPatricia ManaliliNo ratings yet
- 1.1 and 1.2 Eye Anatomy - Examination (Eneganiron) 2Document153 pages1.1 and 1.2 Eye Anatomy - Examination (Eneganiron) 2charmaine.admanaNo ratings yet
- DS Case 2 - SSDocument28 pagesDS Case 2 - SSKaka MaulanaNo ratings yet
- Eye & EarDocument15 pagesEye & EarfatimasulaimanishereNo ratings yet
- Anatomy and Physio HandoutsDocument6 pagesAnatomy and Physio HandoutsKoj LozadaNo ratings yet
- Anatomy and Physiology of The EyeDocument18 pagesAnatomy and Physiology of The EyeMargaretha AdhiningrumNo ratings yet
- Assessing Cranial NerveDocument5 pagesAssessing Cranial Nerve21-54405No ratings yet
- Anatomy of The EyeballDocument3 pagesAnatomy of The EyeballMary Joy OamilNo ratings yet
- The EyeDocument8 pagesThe Eyezyrine jhen100% (1)
- Human EyeDocument32 pagesHuman Eyekaruparthi sripravallikaNo ratings yet
- OPHTHA - Review QuizDocument6 pagesOPHTHA - Review QuizADRIAN TIGLAONo ratings yet
- General Eye Care: Prepared By: Ma. Elena Fe G. Acosta, SN4, HTUDocument26 pagesGeneral Eye Care: Prepared By: Ma. Elena Fe G. Acosta, SN4, HTUmefacostaNo ratings yet
- (OPTHA) Lec 5 - RetinaDocument5 pages(OPTHA) Lec 5 - RetinaPatricia ManaliliNo ratings yet
- LensDocument15 pagesLensS De SilvaNo ratings yet
- DISORDERS of The EYE and EARDocument8 pagesDISORDERS of The EYE and EARAnna Carmela P. MelendezNo ratings yet
- CM3 - Cu16 Assessment of Neurologic System - 316089470Document17 pagesCM3 - Cu16 Assessment of Neurologic System - 316089470KAREN RODASNo ratings yet
- Assessment of The Eyes STUDENTDocument7 pagesAssessment of The Eyes STUDENTRolandNo ratings yet
- Chapter 8-SPECIAL SENSESDocument5 pagesChapter 8-SPECIAL SENSESRishelle Mae Miñoza Pilones100% (1)
- Eent Handouts 1Document6 pagesEent Handouts 1Aliza Abn bklNo ratings yet
- 1.1 HEENT EyesDocument6 pages1.1 HEENT EyesJohn TecsonNo ratings yet
- Week 7 - Assessment of The EyeDocument7 pagesWeek 7 - Assessment of The EyeBLOCK 20 - EULER PABILLONo ratings yet
- 8 EentDocument9 pages8 Eentthe someoneNo ratings yet
- Ocular ExaminationDocument2 pagesOcular ExaminationMuhammad HaziqNo ratings yet
- 025e6f8e7c33e-HUMAN EYE AND NERVOUS SYSTEM PDFDocument37 pages025e6f8e7c33e-HUMAN EYE AND NERVOUS SYSTEM PDFRyuu SSDNo ratings yet
- Anatomy of The Adult and Neonatal SkullDocument8 pagesAnatomy of The Adult and Neonatal SkullkatrizmaervillagantolNo ratings yet
- HA RLE MidtermsDocument7 pagesHA RLE MidtermsKaela ChoiNo ratings yet
- Ocular ExaminationDocument2 pagesOcular ExaminationMuhammad HaziqNo ratings yet
- By Morphology by Morphology: by Sets of TeethDocument112 pagesBy Morphology by Morphology: by Sets of TeethMaryjoy PaladanNo ratings yet
- S3-04 Ophthalmology Chronic Vision Loss PDFDocument12 pagesS3-04 Ophthalmology Chronic Vision Loss PDFAl SyNo ratings yet
- A&P - 10. Special Senses (12p)Document12 pagesA&P - 10. Special Senses (12p)Gabriel StratulatNo ratings yet
- EENT NotesDocument12 pagesEENT NotesMhae TabasaNo ratings yet
- Head 3: Eyelids - Orbit and Content of OrbitDocument14 pagesHead 3: Eyelids - Orbit and Content of OrbitKim RamosNo ratings yet
- Head To Toe Assessment Adult HealthDocument7 pagesHead To Toe Assessment Adult HealthFrancesca LopesNo ratings yet
- Eyes and Ears Maam JezDocument8 pagesEyes and Ears Maam JezJoana DupagonNo ratings yet
- Radiographic Positioning and Radiologic Procedures I FinalsDocument13 pagesRadiographic Positioning and Radiologic Procedures I FinalsrozdhagaNo ratings yet
- 1 Anatomy & Physiology of Eye For Ophthalmic NursesDocument124 pages1 Anatomy & Physiology of Eye For Ophthalmic NursesSMEY204100% (1)
- 4 FaceDocument4 pages4 FaceKimberlee Ced NoolNo ratings yet
- Pediatric Ophthalmology Anatomy and ExaminationDocument21 pagesPediatric Ophthalmology Anatomy and ExaminationGlydenne Gayam100% (1)
- (Ophtha) 1.1 Anatomy of The EyeDocument4 pages(Ophtha) 1.1 Anatomy of The EyePatrick Bautista100% (1)
- L1 - History and Physical ExaminationDocument22 pagesL1 - History and Physical ExaminationConger CongerNo ratings yet
- L05 Special Senses WAnsDocument52 pagesL05 Special Senses WAnsKa Yan LAUNo ratings yet
- Gross HSB A - The Facial MusclesDocument4 pagesGross HSB A - The Facial MusclesAngelo BautistaNo ratings yet
- Eent + OrthoDocument87 pagesEent + OrthoKaris HemmingsNo ratings yet
- Scleral Lens FittingDocument22 pagesScleral Lens FittingJoseph Chipana GutierrezNo ratings yet
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsFrom EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsNo ratings yet
- ForgramDocument1 pageForgramJohn TecsonNo ratings yet
- Rosary Prayers in LatinDocument5 pagesRosary Prayers in LatinJohn Tecson100% (1)
- PD2 Final Exam MergedDocument35 pagesPD2 Final Exam MergedJohn TecsonNo ratings yet
- 1.1 HEENT EyesDocument6 pages1.1 HEENT EyesJohn TecsonNo ratings yet
- Sample Problems in Quality Control 1Document17 pagesSample Problems in Quality Control 1John TecsonNo ratings yet
- Hypertension Walker JNC 8Document10 pagesHypertension Walker JNC 8John TecsonNo ratings yet
- Module 1 Corrections: #20. We Were Told To Shade EDocument4 pagesModule 1 Corrections: #20. We Were Told To Shade EJohn TecsonNo ratings yet
- Pharmacognosy PPT 2ND ShiftDocument105 pagesPharmacognosy PPT 2ND ShiftJohn TecsonNo ratings yet
- ANSWER KEY Opioids Antihistamine NSAIDDocument2 pagesANSWER KEY Opioids Antihistamine NSAIDJohn TecsonNo ratings yet
- Dispensing CA NotesDocument16 pagesDispensing CA NotesJohn TecsonNo ratings yet
- Four Chambers of The HeartDocument7 pagesFour Chambers of The HeartJohn TecsonNo ratings yet
- Four Chambers of The HeartDocument7 pagesFour Chambers of The HeartJohn TecsonNo ratings yet
- Verb Tense - StructureDocument3 pagesVerb Tense - Structureapi-179604969No ratings yet
- Psychiatry Case Presentation: Candice Reyes, MS III Pacific Hospital of Long BeachDocument11 pagesPsychiatry Case Presentation: Candice Reyes, MS III Pacific Hospital of Long BeachMarcel Alexandru GainaNo ratings yet
- Endocrine Disorders Worksheetanskey2012-1Document5 pagesEndocrine Disorders Worksheetanskey2012-1mezuniga1100% (1)
- Bijnor Thesis Research by Pragya SrivastavaDocument291 pagesBijnor Thesis Research by Pragya SrivastavaPragya Srivastava AgrawalNo ratings yet
- Davis, George Carroll - Serrano, Elena Lidia - Food and Nutrition Economics - Fundamentals For Health Sciences-Oxford University Press (2016)Document290 pagesDavis, George Carroll - Serrano, Elena Lidia - Food and Nutrition Economics - Fundamentals For Health Sciences-Oxford University Press (2016)ismi nor azmiNo ratings yet
- Causes of ObesityDocument3 pagesCauses of ObesityKaren Chambre100% (1)
- Research Paper On Ancient Head SurgeryDocument9 pagesResearch Paper On Ancient Head SurgerySourav PandaNo ratings yet
- Facts To Know About Piles and The Scope of Homeopathy Treatment in Piles.Document16 pagesFacts To Know About Piles and The Scope of Homeopathy Treatment in Piles.mhmulticareNo ratings yet
- Soya Based Diets DiabetesDocument4 pagesSoya Based Diets DiabetesYesi Novia AmbaraniNo ratings yet
- A Practical Guide To Diabetes Mellitus 7th Ed - Nihal Thomas, Nitin Kapoor, Jachin Velavan, Senthil Vasan KDocument621 pagesA Practical Guide To Diabetes Mellitus 7th Ed - Nihal Thomas, Nitin Kapoor, Jachin Velavan, Senthil Vasan KconicharlesNo ratings yet
- Addiction To DR-WPS OfficeDocument1 pageAddiction To DR-WPS OfficeFarrah BadillaNo ratings yet
- Poli Dalam Poli Paru: Daftar Diagnosa Penyakit Berdasarkan Icd-10Document6 pagesPoli Dalam Poli Paru: Daftar Diagnosa Penyakit Berdasarkan Icd-10Nannda SuccindaaNo ratings yet
- Poverty and Mental IllnessDocument14 pagesPoverty and Mental Illnessapi-548687321No ratings yet
- VasculittisDocument28 pagesVasculittisBernamai CalamNo ratings yet
- Soal ADocument13 pagesSoal AArvigo ArgaNo ratings yet
- Oregon COVID-19 Weekly Report (Published Oct. 21, 2020)Document33 pagesOregon COVID-19 Weekly Report (Published Oct. 21, 2020)KGW NewsNo ratings yet
- Heart Medicines HomeopathicDocument6 pagesHeart Medicines Homeopathicwaseem_karachiNo ratings yet
- AbortionDocument33 pagesAbortionVinay SahuNo ratings yet
- Turner's SyndromeDocument38 pagesTurner's SyndromeCerry PratiwiNo ratings yet
- Soal MCQ Blok 16Document14 pagesSoal MCQ Blok 16Mira Pandora100% (1)
- E-bOOK Causes-And-Treatment-Of-Vitamin-D-DeficiencyDocument15 pagesE-bOOK Causes-And-Treatment-Of-Vitamin-D-DeficiencyPoongkodi KNo ratings yet
- NclexDocument4 pagesNclexihatetouNo ratings yet
- Merged For PrintDocument141 pagesMerged For PrintBb PrintsNo ratings yet
- LIBERTY's Basic Food HygieneDocument156 pagesLIBERTY's Basic Food Hygienestarlite100% (1)
- Drug Study: Submitted To: Mr. Blas Blasil A. PurgananDocument7 pagesDrug Study: Submitted To: Mr. Blas Blasil A. Purganancharanjit kaurNo ratings yet