Download as pdf or txt
You might also like
- 120lab Report 3Document4 pages120lab Report 3Valerie Mae Librero Areño100% (2)
- Kheniser, K Et Al (2021) Long-Term Weight Loss Strategies For ObesityDocument13 pagesKheniser, K Et Al (2021) Long-Term Weight Loss Strategies For Obesityasdrubal5martinezNo ratings yet
- 2022 - JCEM - Metabolic Efficacy of Time-Restricted Eating in AdultsDocument14 pages2022 - JCEM - Metabolic Efficacy of Time-Restricted Eating in AdultsLuiz Fernando Fonseca VieiraNo ratings yet
- Review ArticleDocument9 pagesReview ArticleottohasibuNo ratings yet
- Obesity Phenotypes and Their Paradoxical Association With Cardiovascular DiseasesDocument64 pagesObesity Phenotypes and Their Paradoxical Association With Cardiovascular DiseasesIkke OppgaveNo ratings yet
- Material 5Document17 pagesMaterial 5Kleivson De Aquinon FerreiraNo ratings yet
- Metabolic and Body Composition Factors in Subgroups of Obesity: What Do We Know?Document7 pagesMetabolic and Body Composition Factors in Subgroups of Obesity: What Do We Know?Jos CanalesNo ratings yet
- Pigłowska 2016Document8 pagesPigłowska 2016Sam Steven Hernandez JañaNo ratings yet
- Tovar Et Al-2017-Molecular Nutrition & Food ResearchDocument12 pagesTovar Et Al-2017-Molecular Nutrition & Food ResearchRal T. BerensNo ratings yet
- Jcem 2952Document9 pagesJcem 2952parta anantamaNo ratings yet
- Articulo Dislipidemias 2Document18 pagesArticulo Dislipidemias 2DANIELA CALDERON SAGAHONNo ratings yet
- Cells 10 03030Document23 pagesCells 10 03030Almir FilsNo ratings yet
- Articulo Dislipidemias 2Document16 pagesArticulo Dislipidemias 2DANIELA CALDERON SAGAHONNo ratings yet
- JCM 08 01645 PDFDocument11 pagesJCM 08 01645 PDFFranklin Howley-Dumit SerulleNo ratings yet
- Babu-Positive Effects of Exercise Intervention Without Weight Loss 2021Document28 pagesBabu-Positive Effects of Exercise Intervention Without Weight Loss 2021markwsheppardhotmail.comNo ratings yet
- Nutrition and Exercise Interventions To Improve Body Composition ForDocument23 pagesNutrition and Exercise Interventions To Improve Body Composition Forivanov.pravnikNo ratings yet
- Am J Clin Nutr 2016 Valsesia Ajcn.116.137646Document10 pagesAm J Clin Nutr 2016 Valsesia Ajcn.116.137646kasabeNo ratings yet
- 10 3390@nu12072005Document19 pages10 3390@nu12072005Maria Isabel LondoñoNo ratings yet
- Definitions, Classification, and Epidemiology of ObesityDocument1 pageDefinitions, Classification, and Epidemiology of ObesityReza RamadhansyahNo ratings yet
- The Impacts of Various Sorts of Weight Control Plans On Large People Determined To Have Type 2 DiabeticsDocument12 pagesThe Impacts of Various Sorts of Weight Control Plans On Large People Determined To Have Type 2 DiabeticsB O J H E S :No ratings yet
- Modulo MetabolicoDocument10 pagesModulo MetabolicoFrancisco Javier Fuentealba UribeNo ratings yet
- JCM 09 02797Document21 pagesJCM 09 02797Steffany Dias LimaNo ratings yet
- Long-Term Effects of Weight Loss With A Very Low Carbohydrate and Low Fat Diet On Vascular Function in Overweight and Obese PatientsDocument10 pagesLong-Term Effects of Weight Loss With A Very Low Carbohydrate and Low Fat Diet On Vascular Function in Overweight and Obese PatientsIyappan SubramaniNo ratings yet
- s13098-021-00762-0Document7 pagess13098-021-00762-020-103-Erick YinartaNo ratings yet
- Accepted Manuscript: Journal of HepatologyDocument31 pagesAccepted Manuscript: Journal of HepatologyNCNo ratings yet
- Are The Associations of Plasma Leptin and Adiponectin With Type 2 Diabetes Independent of Obesity in Older Chinese Adults?Document6 pagesAre The Associations of Plasma Leptin and Adiponectin With Type 2 Diabetes Independent of Obesity in Older Chinese Adults?bogdansoroNo ratings yet
- 1700 Words - Nutritional AssessmentDocument11 pages1700 Words - Nutritional Assessmentmidhat abbasNo ratings yet
- Jurding 4Document7 pagesJurding 4Hocie Trinanda SardiNo ratings yet
- Metabolic Disorders Related ToDocument13 pagesMetabolic Disorders Related TovsdeepsNo ratings yet
- Nutrition and Wellbeing Step1.6 AdditionalReading-OptionalDocument4 pagesNutrition and Wellbeing Step1.6 AdditionalReading-OptionalAlec LiuNo ratings yet
- Sindroma MetabolikDocument7 pagesSindroma MetabolikainindyaNo ratings yet
- 1 s2.0 S0002916522004385 MainDocument11 pages1 s2.0 S0002916522004385 Maincarlos santamariaNo ratings yet
- 10.1007@s11154 019 09514 yDocument12 pages10.1007@s11154 019 09514 ysimonNo ratings yet
- Calorie Restriction With or Without Exercise On Insulin Sensitivity Beta Cell Functions Ectopic LipidDocument8 pagesCalorie Restriction With or Without Exercise On Insulin Sensitivity Beta Cell Functions Ectopic Lipidadibahfauzi85No ratings yet
- Aquila 2020Document40 pagesAquila 2020Juan Daniel Serrano GuerreroNo ratings yet
- Metabolic-Associatedfatty Liverdiseaseanddiabetes: A Double WhammyDocument16 pagesMetabolic-Associatedfatty Liverdiseaseanddiabetes: A Double WhammyFarjana NajninNo ratings yet
- 4-Metabolically Healthy Obesity - Does It ExistDocument9 pages4-Metabolically Healthy Obesity - Does It Existabdeali hazariNo ratings yet
- A Systematic Review and Meta-Analysis of The Effect of Billroth Reconstruction On Type 2 Diabetes: A New Perspective On Old Surgical MethodsDocument11 pagesA Systematic Review and Meta-Analysis of The Effect of Billroth Reconstruction On Type 2 Diabetes: A New Perspective On Old Surgical MethodsAhmed M FriegNo ratings yet
- Exercise Treatment of Obesity - Endotext - NCBI BookshelfDocument10 pagesExercise Treatment of Obesity - Endotext - NCBI BookshelfSameem MunirNo ratings yet
- Effects of A Meal Replacement On Body CompositionDocument10 pagesEffects of A Meal Replacement On Body CompositionGiffariNo ratings yet
- AyunoDocument8 pagesAyunoRaul DavilaNo ratings yet
- Abdominal Obesity and Metabolic Syndrome - Exercise As Medicine - 2018Document16 pagesAbdominal Obesity and Metabolic Syndrome - Exercise As Medicine - 2018Marie GCNo ratings yet
- Metabolic Syndrome XDocument11 pagesMetabolic Syndrome XAndres RiveraNo ratings yet
- Prevention and Treatment of Sarcopenia Obesity (2019)Document24 pagesPrevention and Treatment of Sarcopenia Obesity (2019)Brayam AguilarNo ratings yet
- Metabolic Syndrome Past Present and FutureDocument7 pagesMetabolic Syndrome Past Present and FutureLaura LizarazoNo ratings yet
- Nutrients 12 03774 v3Document21 pagesNutrients 12 03774 v3d6smvtzjnbNo ratings yet
- 1 s2.0 S0026049511003404 MainDocument8 pages1 s2.0 S0026049511003404 MainFrankis De Jesus Vanegas RomeroNo ratings yet
- 2 Year Paleo TrialDocument8 pages2 Year Paleo TrialOfer KulkaNo ratings yet
- Seminario 9 ObesidadDocument11 pagesSeminario 9 Obesidadpau_sebNo ratings yet
- Ketogenic DietsDocument23 pagesKetogenic DietsNorma Edith López DíazGuerreroNo ratings yet
- Articol 1 - The Effectiveness of Dietary Polyphenols in Obesity Management A Systematic Review and Meta-Analysis of Human Clinical TrialsDocument16 pagesArticol 1 - The Effectiveness of Dietary Polyphenols in Obesity Management A Systematic Review and Meta-Analysis of Human Clinical TrialsOfeliaMosteanuNo ratings yet
- Down 2020 5Document16 pagesDown 2020 5Marie GuajardoNo ratings yet
- Is Time-Restricted Eating (8/16) Beneficial For Body Weight and Metabolism of Obese and Overweight Adults? A Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocument14 pagesIs Time-Restricted Eating (8/16) Beneficial For Body Weight and Metabolism of Obese and Overweight Adults? A Systematic Review and Meta-Analysis of Randomized Controlled TrialsEvan LauNo ratings yet
- Evidencia Científica de Dietas para Bajar de Peso Diferente Composición de Macronutrientes, Ayuno Intermitente y Dietas PopularesDocument35 pagesEvidencia Científica de Dietas para Bajar de Peso Diferente Composición de Macronutrientes, Ayuno Intermitente y Dietas PopularesCesar Flores ValleNo ratings yet
- NutrientsDocument17 pagesNutrientsNenden ApriliyantiNo ratings yet
- Effects of Macronutrient Intake in Obesity A Mt-AnalysisDocument16 pagesEffects of Macronutrient Intake in Obesity A Mt-AnalysisJúlia BenckeNo ratings yet
- Abstracts For The Website - pdf1441898071Document166 pagesAbstracts For The Website - pdf1441898071Radu MiricaNo ratings yet
- Mudanças Na Composição Corporal Com Dieta Hipocalórica Combinada Com Atividade Física Sedentária, Moderada e Intensa - Um Ensaio Clínico Randomizado - InglêsDocument21 pagesMudanças Na Composição Corporal Com Dieta Hipocalórica Combinada Com Atividade Física Sedentária, Moderada e Intensa - Um Ensaio Clínico Randomizado - InglêsJuliana MontovaniNo ratings yet
- Is BMI The Best Measure of Obesity?: Anthropometric Measures in AdultsDocument4 pagesIs BMI The Best Measure of Obesity?: Anthropometric Measures in AdultsmuthmainnahNo ratings yet
- Efficacy of Lifestyle Interventions in Patients With Type 2 Diabetes - A Systematic Review and Meta-AnalysisDocument11 pagesEfficacy of Lifestyle Interventions in Patients With Type 2 Diabetes - A Systematic Review and Meta-AnalysisDara Agusti MaulidyaNo ratings yet
- Prolonged Extreme Thrombocytosis in A Postsplenectomy Patient With Hereditary Spherocytosis PDFDocument6 pagesProlonged Extreme Thrombocytosis in A Postsplenectomy Patient With Hereditary Spherocytosis PDFSotir LakoNo ratings yet
- PorphyriaDocument17 pagesPorphyriaSotir LakoNo ratings yet
- Walking Speed, The Functional Vital SignDocument17 pagesWalking Speed, The Functional Vital SignSotir LakoNo ratings yet
- Eosinophilic GastroenteritisDocument7 pagesEosinophilic GastroenteritisSotir LakoNo ratings yet
- Hippocratic Face PDFDocument1 pageHippocratic Face PDFSotir LakoNo ratings yet
- Adherence To The Mediterranean Diet Is Associated With Lower Platelet and Leukocyte CountsDocument8 pagesAdherence To The Mediterranean Diet Is Associated With Lower Platelet and Leukocyte CountsSotir LakoNo ratings yet
- Bridge TherapyDocument2 pagesBridge TherapySotir LakoNo ratings yet
- The Normal DistributionDocument30 pagesThe Normal DistributionJohn Rich CaidicNo ratings yet
- Inverse of A FunctionDocument10 pagesInverse of A Functionnitin30100% (2)
- Mec R2018Document227 pagesMec R2018Kishore Kumar RNo ratings yet
- 5 - Introduction Q-Series Vs2 Customer Version2Document49 pages5 - Introduction Q-Series Vs2 Customer Version2mahreza189100% (1)
- Bsme 3-B: Me 114 - Heat Transfer Bachelor of Science in Mechanical EngineeringDocument3 pagesBsme 3-B: Me 114 - Heat Transfer Bachelor of Science in Mechanical EngineeringJethro Briza GaneloNo ratings yet
- X PPT CH 12 ElectricityDocument12 pagesX PPT CH 12 ElectricityAakriti100% (1)
- CESCCommunityProjectPlan Brgy - MacarioDaconDocument6 pagesCESCCommunityProjectPlan Brgy - MacarioDaconKennedy BalmoriNo ratings yet
- 1 s2.0 S0264127522004105 MainDocument11 pages1 s2.0 S0264127522004105 MainAsimov RiyazNo ratings yet
- 765 KV, 400 KV, 230 KV & 132 KV Grid Network (Existing, U/C & Planned)Document1 page765 KV, 400 KV, 230 KV & 132 KV Grid Network (Existing, U/C & Planned)SSDNo ratings yet
- Annual Report 2014 PDFDocument153 pagesAnnual Report 2014 PDFகோகுல் இராNo ratings yet
- Rakit Lampu LedDocument11 pagesRakit Lampu LedIbnusyam UtihNo ratings yet
- Low Noise Amplifier Basics: by V. M. García-ChocanoDocument4 pagesLow Noise Amplifier Basics: by V. M. García-ChocanoPranjal Jalan100% (1)
- Solution Manual For Fundamentals of Semiconductor Fabrication Gary S May Simon M Sze Isbn 0471232793 Isbn 978-0-471 23279 7 Isbn 9780471232797Document16 pagesSolution Manual For Fundamentals of Semiconductor Fabrication Gary S May Simon M Sze Isbn 0471232793 Isbn 978-0-471 23279 7 Isbn 9780471232797warepneumomxkhf100% (17)
- The Harrod-Domar Growth ModelDocument6 pagesThe Harrod-Domar Growth ModelSimeonNo ratings yet
- Operation Reasrech On IglooDocument18 pagesOperation Reasrech On IglooMd Yeasin ArafatNo ratings yet
- Lecture 4Document24 pagesLecture 4Geeta AroraNo ratings yet
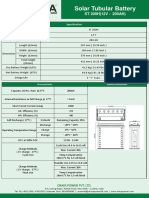
- ST200HDocument2 pagesST200HAnjana DissanayakaNo ratings yet
- Biology Investigatory Project: Malaria: Its Effects and CausesDocument17 pagesBiology Investigatory Project: Malaria: Its Effects and CausesRishi KeshavNo ratings yet
- ToR For Fiberglass Biogas Plants Installation - EOI PDFDocument4 pagesToR For Fiberglass Biogas Plants Installation - EOI PDFmy09No ratings yet
- Gennady Nesis, Leonid Shulman, Malcolm Gesthuysen - Tactics in The King's IndianDocument130 pagesGennady Nesis, Leonid Shulman, Malcolm Gesthuysen - Tactics in The King's Indiancodonauta100% (1)
- Arthur Lumley Davi̇ds-Sultan Ii. Mahmuta-1832Document318 pagesArthur Lumley Davi̇ds-Sultan Ii. Mahmuta-1832cengizozakinciNo ratings yet
- Unit I-Cloud ComputingDocument29 pagesUnit I-Cloud ComputingAR OFFICIALNo ratings yet
- Veins and Hydrothermal DepositsDocument2 pagesVeins and Hydrothermal Depositsalimurtadha100% (1)
- Snag SummmariesDocument171 pagesSnag Summmarieslaltu adgiriNo ratings yet
- Production of Biodegradable Plastics AsDocument6 pagesProduction of Biodegradable Plastics AsEbenezer EffisahNo ratings yet
- Metzeler TDB 2019 LRDocument246 pagesMetzeler TDB 2019 LRGabriel BruschiNo ratings yet
- CD Dye RD0005Document7 pagesCD Dye RD0005Juan CarlosNo ratings yet
- Costing By-Product and Joint ProductsDocument36 pagesCosting By-Product and Joint ProductseltantiNo ratings yet
- Synchronous Generators: Instructional ObjectivesDocument18 pagesSynchronous Generators: Instructional Objectivessanthosh2009No ratings yet