Download as pdf or txt
You might also like
- Anatomy, Imaging and Surgery of The Intracranial Dural Venous SinusesDocument255 pagesAnatomy, Imaging and Surgery of The Intracranial Dural Venous SinusesmuelmiharNo ratings yet
- Cerebellar Dizziness and Vertigo - Etiologies, Diagnostic and TratmentDocument10 pagesCerebellar Dizziness and Vertigo - Etiologies, Diagnostic and Tratmentrafael rocha novaesNo ratings yet
- Function of CerebellumDocument38 pagesFunction of CerebellumNaOMi MiNaMiNo ratings yet
- ATA-PCA BypassDocument4 pagesATA-PCA Bypasskaan_yagmur7711No ratings yet
- Revista Chilena de Neuro-Psiquiatría: Microanatomy of The Posterior Cerebral ArteryDocument20 pagesRevista Chilena de Neuro-Psiquiatría: Microanatomy of The Posterior Cerebral ArterykatemuNo ratings yet
- 10.1007@s12565 012 0166 6Document13 pages10.1007@s12565 012 0166 6San Phạm ĐìnhNo ratings yet
- Sosa 2016Document10 pagesSosa 201616fernandoNo ratings yet
- Transcriptomic Diversity of Cell Types Across TheDocument34 pagesTranscriptomic Diversity of Cell Types Across ThepdmNo ratings yet
- DR Sameeha KhanDocument69 pagesDR Sameeha KhanCristian O. Saavedra RodriguezNo ratings yet
- Basic Knowledge of Stroke Discussion On Classification, Anatomy and ManagementDocument54 pagesBasic Knowledge of Stroke Discussion On Classification, Anatomy and ManagementomyNo ratings yet
- Common Neurologic Disorders: Krista M. GarnerDocument12 pagesCommon Neurologic Disorders: Krista M. GarnerTeda G.No ratings yet
- Benner 2021Document9 pagesBenner 2021Bobby VarkeyNo ratings yet
- Aneurysms of The Posterior Cerebral Artery ClassifDocument9 pagesAneurysms of The Posterior Cerebral Artery ClassifClaudia Ivette Villarreal OvalleNo ratings yet
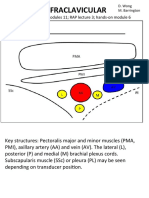
- Infraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6Document4 pagesInfraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6DonkeyManNo ratings yet
- LacZ-reporter Mapping of Dlx5-6 ExpressionDocument54 pagesLacZ-reporter Mapping of Dlx5-6 Expression15905196268No ratings yet
- yZGn9p PaudelDocument4 pagesyZGn9p PaudelAliyah Tofani PawelloiNo ratings yet
- Embryology and Variations of Cerebral Arteries - A Pictorial ReviewDocument33 pagesEmbryology and Variations of Cerebral Arteries - A Pictorial ReviewAngelique NatalieNo ratings yet
- H. StrokeDocument3 pagesH. StrokeKyle VargasNo ratings yet
- Bimbingan BsDocument42 pagesBimbingan BsMohamad NasrullohNo ratings yet
- Tugas Bedah Saraf: Pembimbing: Dr. Arinta Puspita Wati, Sps Oleh: Astri Angelina SitaniapessyDocument42 pagesTugas Bedah Saraf: Pembimbing: Dr. Arinta Puspita Wati, Sps Oleh: Astri Angelina SitaniapessyMohamad NasrullohNo ratings yet
- Cerebrovascular EmbryologyDocument21 pagesCerebrovascular EmbryologyanuroxxxNo ratings yet
- 2020 Evc Isquemico Localizacion ClinicaDocument19 pages2020 Evc Isquemico Localizacion ClinicaJuan Pablo B. FloresNo ratings yet
- Lecture 11: Cerebrum: Neuroscience 1: Cerebral CirculationDocument11 pagesLecture 11: Cerebrum: Neuroscience 1: Cerebral CirculationAudrey Nicole LisingNo ratings yet
- 75631-Anatomy of The Intracranial Vessels and Vascular Territories - JagerDocument10 pages75631-Anatomy of The Intracranial Vessels and Vascular Territories - JagernurlanNo ratings yet
- Lecture Vascular of BrainDocument52 pagesLecture Vascular of BrainAditya Pramana KasidiNo ratings yet
- Subarachnoid BlockDocument25 pagesSubarachnoid BlockScribdTranslationsNo ratings yet
- Midbrain, Pons, and Medulla: Anatomy and SyndromesDocument16 pagesMidbrain, Pons, and Medulla: Anatomy and SyndromesJasper CubiasNo ratings yet
- Review of Functional Neuroanatomy (7) CNS VascularizationDocument38 pagesReview of Functional Neuroanatomy (7) CNS VascularizationUunsariNo ratings yet
- Review Anatomi Fisiologi Sistem PersarafanDocument78 pagesReview Anatomi Fisiologi Sistem PersarafanNisa FathonahNo ratings yet
- Anatomy and Physiology of Intrinsic Cardiac Autonomic Nervous SystemDocument5 pagesAnatomy and Physiology of Intrinsic Cardiac Autonomic Nervous SystemSori B. Requena C.No ratings yet
- Anatomy of The Intracranial - 240401 - 093814Document20 pagesAnatomy of The Intracranial - 240401 - 093814Roberto Hernadez SuarezNo ratings yet
- Ambient CisternDocument8 pagesAmbient CisternAmrutha PCNo ratings yet
- Marcati 2017Document9 pagesMarcati 2017J Alan SantosNo ratings yet
- Brachial PlexusDocument5 pagesBrachial PlexusRajveerNo ratings yet
- Blood Supply of The Brain: by Dr. Noura El TahawyDocument100 pagesBlood Supply of The Brain: by Dr. Noura El TahawySureshNo ratings yet
- Anatomy and Pathology of The Cardiac Conduction SystemDocument16 pagesAnatomy and Pathology of The Cardiac Conduction SystemAngel CVNo ratings yet
- Anatomia Plexului BrahialDocument10 pagesAnatomia Plexului BrahialsuzzixxNo ratings yet
- Blood Supply NeuroDocument60 pagesBlood Supply NeuroFatima FalahNo ratings yet
- Cerebellar Output Motor and Cognitive Channels - TiDocument7 pagesCerebellar Output Motor and Cognitive Channels - Tivikhen0712No ratings yet
- NEUROANATOMYDocument34 pagesNEUROANATOMYRavanno Fanizza HarahapNo ratings yet
- Pure Thalamic Infarctions Clinical FindingsDocument11 pagesPure Thalamic Infarctions Clinical FindingsshofidhiaaaNo ratings yet
- Temporal Lobe Arteriovenous Malformations: Anatomical Subtypes, Surgical Strategy, and OutcomesDocument13 pagesTemporal Lobe Arteriovenous Malformations: Anatomical Subtypes, Surgical Strategy, and OutcomesZeptalanNo ratings yet
- Cardiac AnatomyDocument17 pagesCardiac AnatomyAndreas Erick HaurissaNo ratings yet
- Arndt 1996Document27 pagesArndt 1996M4shroomNo ratings yet
- Anatomy of Brachial Plexus: DR - Sadiq Wadood Siddiqui JR3 Department of AnatomyDocument53 pagesAnatomy of Brachial Plexus: DR - Sadiq Wadood Siddiqui JR3 Department of AnatomySadiq Wadood SiddiquiNo ratings yet
- Fosa PosteriorDocument16 pagesFosa PosteriorCarlos AlvaradoNo ratings yet
- Anatomy of Spinal Blood Supply: Anatomia Da Circulação MedularDocument5 pagesAnatomy of Spinal Blood Supply: Anatomia Da Circulação MedularAnusha SebastianNo ratings yet
- Zhang Et Al 2023Document21 pagesZhang Et Al 2023Ignacio BarbieriNo ratings yet
- Brain Attack Needing ResucitationDocument11 pagesBrain Attack Needing ResucitationCony MaccagnanNo ratings yet
- Lymphatic FilariasisDocument17 pagesLymphatic FilariasisSelvaNo ratings yet
- Brain & Its Surrounding Structures: Anatomi Blok 1.5Document6 pagesBrain & Its Surrounding Structures: Anatomi Blok 1.5RizkiWikantyasningNo ratings yet
- Anatomy Id - Final MergedDocument152 pagesAnatomy Id - Final MergedCastleKGNo ratings yet
- Anatomy, Imaging and Pathologic Conditions of Brachial PlexusDocument67 pagesAnatomy, Imaging and Pathologic Conditions of Brachial PlexusChrista Levina DaniswaraNo ratings yet
- 124 573 1 PBDocument5 pages124 573 1 PBErez Tryaza HimuraNo ratings yet
- Microsurgical Anatomy of The Central LobeDocument16 pagesMicrosurgical Anatomy of The Central LobeWilson WqaNo ratings yet
- Arteries of The Insula: U T, M.D., M. G Y, M.D., O A - M, M.D., D C. H. Y, R.NDocument12 pagesArteries of The Insula: U T, M.D., M. G Y, M.D., O A - M, M.D., D C. H. Y, R.NMihaela AndreiNo ratings yet
- Patterning The Developing DiencephalonDocument10 pagesPatterning The Developing DiencephalonAndres MoraNo ratings yet
- Brainstem CN1-6Document31 pagesBrainstem CN1-6Dhanen Dran100% (1)
- 639 Full PDFDocument10 pages639 Full PDFMeiriyani LembangNo ratings yet
- Symmetry: Symmetry of The Brain Is The Key To RadiologicDocument7 pagesSymmetry: Symmetry of The Brain Is The Key To RadiologicVon HippoNo ratings yet
- Arteries and Veins of The Cerebellum: Original PaperDocument33 pagesArteries and Veins of The Cerebellum: Original PaperCan EkerNo ratings yet
- 1 s2.0 S2666084923005089 MainDocument6 pages1 s2.0 S2666084923005089 MainGabriel JoséNo ratings yet
- External Carotid Artery: Imaging Anatomy Atlas for Endovascular TreatmentFrom EverandExternal Carotid Artery: Imaging Anatomy Atlas for Endovascular TreatmentHiro KiyosueNo ratings yet
- How To Create Slides Like A Even If You'Re: Designer ScientistDocument34 pagesHow To Create Slides Like A Even If You'Re: Designer ScientistmuelmiharNo ratings yet
- (10920684 - Neurosurgical Focus) Heschl's Gyrus Fiber Intersection Area - A New Insight On The Connectivity of The Auditory-Language Hub PDFDocument11 pages(10920684 - Neurosurgical Focus) Heschl's Gyrus Fiber Intersection Area - A New Insight On The Connectivity of The Auditory-Language Hub PDFmuelmiharNo ratings yet
- 2020 - Uz - Anatomic Analysis of The Internal and External Aspects of The PterionDocument5 pages2020 - Uz - Anatomic Analysis of The Internal and External Aspects of The PterionmuelmiharNo ratings yet
- 2017 - Dalkara - Cerebral MicrocirculationDocument5 pages2017 - Dalkara - Cerebral MicrocirculationmuelmiharNo ratings yet
- Thearteryofthecerebellopontine CPNov 20Document52 pagesThearteryofthecerebellopontine CPNov 20muelmiharNo ratings yet
- 2017 - Egemen - Anatomy of Cerebral Veins and Dural SinusesDocument5 pages2017 - Egemen - Anatomy of Cerebral Veins and Dural SinusesmuelmiharNo ratings yet
- 2018 - Ni Et Al - Applied Anatomy and Biomechanics of The Atlantoaxial Joint ComplexDocument12 pages2018 - Ni Et Al - Applied Anatomy and Biomechanics of The Atlantoaxial Joint ComplexmuelmiharNo ratings yet
- 2007 - The Relation Between The Spatial Distribution of Vertebral Artery Compromise and Exposure To Cervical ManipulationDocument7 pages2007 - The Relation Between The Spatial Distribution of Vertebral Artery Compromise and Exposure To Cervical ManipulationmuelmiharNo ratings yet
- The Posterior Cranial FossaDocument297 pagesThe Posterior Cranial FossamuelmiharNo ratings yet
- MCI FMGE Previous Year Solved Question Paper 2007Document0 pagesMCI FMGE Previous Year Solved Question Paper 2007Sharat ChandraNo ratings yet
- IELTS SHARE-IELTS - Practice - Tests - Plus - 3Document56 pagesIELTS SHARE-IELTS - Practice - Tests - Plus - 3Vân Vũ HồngNo ratings yet
- AtaxiaDocument10 pagesAtaxiaosakaNo ratings yet
- The Boxing Debate by The British Medical AssociationDocument132 pagesThe Boxing Debate by The British Medical AssociationTheRealBarrettNo ratings yet
- 09 AfoDocument107 pages09 AfonovitaNo ratings yet
- Lecture Notes Introduction To Nervous SystemDocument8 pagesLecture Notes Introduction To Nervous SystemKirstie Goc-ongNo ratings yet
- Introduction To NeuroanatomyDocument21 pagesIntroduction To Neuroanatomybelete abyuNo ratings yet
- Physio Uhs Solved Past Papers 2nd YearDocument126 pagesPhysio Uhs Solved Past Papers 2nd YearMudassar Roomi100% (3)
- Voluntary Eye Movements PDFDocument14 pagesVoluntary Eye Movements PDFsmdiviNo ratings yet
- Bates CH 17 NeuroDocument11 pagesBates CH 17 NeurokandeeNo ratings yet
- Form 4 Science Chapter 2.4 & 2.5 Muscle, Tendon, Ligament and BrainDocument32 pagesForm 4 Science Chapter 2.4 & 2.5 Muscle, Tendon, Ligament and BraincmeeflyNo ratings yet
- Cerebellar StrokeDocument12 pagesCerebellar StrokewhitecloudsNo ratings yet
- CerebellumDocument28 pagesCerebellumZoya MoraniNo ratings yet
- Etiology of Autism Spectrum Disorders: Genes, Environment, or Both?Document16 pagesEtiology of Autism Spectrum Disorders: Genes, Environment, or Both?Carlos Charlotte SalvadorNo ratings yet
- Chapter 8 - Nervous ReviewerDocument18 pagesChapter 8 - Nervous Reviewerchristian anchetaNo ratings yet
- Lecture - 1 - CNSDocument51 pagesLecture - 1 - CNSKaito Noburu ShinNo ratings yet
- Aumann 1996Document12 pagesAumann 1996M4shroomNo ratings yet
- Etv Perdev 4Document10 pagesEtv Perdev 4Don Angelo De GuzmanNo ratings yet
- Anatomy and Physiology of The Cerebrovascular SystemDocument3 pagesAnatomy and Physiology of The Cerebrovascular SystemNursing Files50% (4)
- Comparison Studies of Moringa Oleifera's Seed Powder and Leaf PowderDocument271 pagesComparison Studies of Moringa Oleifera's Seed Powder and Leaf PowderFahad SiddiquiNo ratings yet
- Neurology MCQ MixDocument53 pagesNeurology MCQ Mixezati pedramNo ratings yet
- Brain Development in Autism Early Overgrowth Followed by Premature Arrest of GrowthDocument6 pagesBrain Development in Autism Early Overgrowth Followed by Premature Arrest of GrowthIoana FarcașNo ratings yet
- Midbrain Activation For AdultsDocument2 pagesMidbrain Activation For AdultsRightBrain PatelNo ratings yet
- Brain Based Gait Assessment FinalDocument13 pagesBrain Based Gait Assessment FinalJESA MARI S SALONGANo ratings yet
- Takakusaki Et Al 2022 - Neurophysiological Mechanisms of Gait Disturbance in Advanced ParkinsonDocument17 pagesTakakusaki Et Al 2022 - Neurophysiological Mechanisms of Gait Disturbance in Advanced ParkinsonlicmarinamaranNo ratings yet
- DR Bhatia Medical Coaching Institute: NeuroanatomyDocument3 pagesDR Bhatia Medical Coaching Institute: NeuroanatomyAastha JainNo ratings yet
- Case Study ChoreaDocument18 pagesCase Study ChoreaKinjalNo ratings yet
- 21.neural Control and CoordinationDocument44 pages21.neural Control and Coordinationg1307No ratings yet