
Diagnostic Procedures
Diagnostic Procedures
You might also like
- Swedish MassageDocument45 pagesSwedish MassageLawrence Cada Nofies100% (6)
- Case Study - Congestive Heart FailureDocument71 pagesCase Study - Congestive Heart FailureFrancis Adrian100% (3)
- Nursing Care Plan For Acute BronchitisDocument6 pagesNursing Care Plan For Acute BronchitisNur Panca Retnaningsih50% (2)
- Curvas Interpretacion Clinica 4Document9 pagesCurvas Interpretacion Clinica 4Patty MArivel ReinosoNo ratings yet
- Jcinvest00338 0038Document8 pagesJcinvest00338 0038Priyadharshini KumarNo ratings yet
- 1.B.09 Resp TestsDocument2 pages1.B.09 Resp Testsalemante100% (1)
- Anesth in Advanced Vent SupportDocument14 pagesAnesth in Advanced Vent SupportFrancisco DuqueNo ratings yet
- 2017 Article 84Document12 pages2017 Article 84flik_gantengNo ratings yet
- Respiratory ICU PDFDocument130 pagesRespiratory ICU PDFAhmed Shihab AhmedNo ratings yet
- Jcinvest00633 0061Document9 pagesJcinvest00633 0061Ravikiran SuryanarayanamurthyNo ratings yet
- Mechanical Ventilation - Chapter 1Document8 pagesMechanical Ventilation - Chapter 1Raninda JuliantiNo ratings yet
- Physiology of Mechanical VentilationDocument12 pagesPhysiology of Mechanical VentilationCarlos ZepedaNo ratings yet
- Respiratory Insufficiency - Pathophysiology,: Diagnosis, Oxygen TherapyDocument11 pagesRespiratory Insufficiency - Pathophysiology,: Diagnosis, Oxygen TherapyBintang UbamnataNo ratings yet
- Mechvent Presentation Midterm To FinalsDocument38 pagesMechvent Presentation Midterm To Finalsfloremie carinoNo ratings yet
- Interpreting Pulmonary Function TestsDocument10 pagesInterpreting Pulmonary Function TestsSuresh Kumar100% (1)
- Module 1 (AEP) - Section 2Document33 pagesModule 1 (AEP) - Section 2asimhafiz0044No ratings yet
- Restrictive Lung DisordersDocument5 pagesRestrictive Lung DisordersSonali RajputNo ratings yet
- Chapter 1 Respiratory System Nomenclature and Ambient ConditionsDocument9 pagesChapter 1 Respiratory System Nomenclature and Ambient Conditionsaisyahasrii_No ratings yet
- Influence of Cardiomegaly On Disordered Breathing During Exercise in Chronic Heart FailureDocument8 pagesInfluence of Cardiomegaly On Disordered Breathing During Exercise in Chronic Heart FailurenadiaNo ratings yet
- Pathophysiology and Classification of Respiratory Failure. Tejpreet Singh Lamba. 2016Document9 pagesPathophysiology and Classification of Respiratory Failure. Tejpreet Singh Lamba. 2016Danitza VeraNo ratings yet
- Atm 06 19 392 PDFDocument13 pagesAtm 06 19 392 PDFPetyr GoranovNo ratings yet
- 24 - Physiology of The Respiratory System PDFDocument38 pages24 - Physiology of The Respiratory System PDFlovelyc95No ratings yet
- The Effects of Lung Recruitment On The Phase III.26Document9 pagesThe Effects of Lung Recruitment On The Phase III.26Fermin LombardiaNo ratings yet
- Oxygen CascadeDocument12 pagesOxygen Cascadehy3pjb1984No ratings yet
- Respiratory Phsysiology 2nd Edition - A - Answers To Self-Study ProbDocument6 pagesRespiratory Phsysiology 2nd Edition - A - Answers To Self-Study ProbRonny Araya AbarcaNo ratings yet
- Jonkman2022 Article LungRecruitmentDocument3 pagesJonkman2022 Article LungRecruitmentCarolina Aguilar OtáloraNo ratings yet
- Atm 06 19 389Document9 pagesAtm 06 19 389Carlos QuirogaNo ratings yet
- EmfizemDocument4 pagesEmfizemJelenaJankovNo ratings yet
- P V Courve in ArdsDocument5 pagesP V Courve in ArdsAdrian BălanNo ratings yet
- Physiology of Respiration 2Document31 pagesPhysiology of Respiration 2kuhutansittinurhalizaNo ratings yet
- Спирометрия Глава 15Document81 pagesСпирометрия Глава 15Mikhail PisarevNo ratings yet
- Respiratory Monitoring Arterial Blood Gas Analysis Pulse Oximetry and End Tida Carbon Dioxide AnalysisDocument4 pagesRespiratory Monitoring Arterial Blood Gas Analysis Pulse Oximetry and End Tida Carbon Dioxide AnalysiskradoNo ratings yet
- Lung Tissue Resistance in Diffuse Interstitial Pulmonary FibrosisDocument9 pagesLung Tissue Resistance in Diffuse Interstitial Pulmonary FibrosisEndhy KurniawanNo ratings yet
- Lung Hyperinflation in COPD: Applying Physiology To Clinical PracticeDocument12 pagesLung Hyperinflation in COPD: Applying Physiology To Clinical PracticeJaya Semara PutraNo ratings yet
- 6 - Glossary - PactDocument7 pages6 - Glossary - PactSanj.etcNo ratings yet
- Respiratory FailureDocument7 pagesRespiratory FailureJesse OnealNo ratings yet
- Manajemen VentiDocument2 pagesManajemen VentiBos AseNo ratings yet
- Pumonary Function TestDocument24 pagesPumonary Function Testmerin sunilNo ratings yet
- Resp Physio SAQsDocument25 pagesResp Physio SAQsanaeshkl100% (1)
- Applsci 09 02842 PDFDocument13 pagesApplsci 09 02842 PDFFelicia SutarliNo ratings yet
- Principals of Mechanical Ventilation in Neonates: DR Mohd Maghayreh PRTH - IrbidDocument78 pagesPrincipals of Mechanical Ventilation in Neonates: DR Mohd Maghayreh PRTH - IrbidAnonymous 58LGc3No ratings yet
- Modes of Mechanical VentilationDocument4 pagesModes of Mechanical Ventilationsgod34100% (1)
- Respiration 473Document3 pagesRespiration 473api-315353725No ratings yet
- Mechanical VentilationDocument62 pagesMechanical Ventilationdrphaninadella100% (1)
- Basic Principles of Mechanical VentilationDocument34 pagesBasic Principles of Mechanical VentilationMohamed KorieshNo ratings yet
- PronoDocument14 pagesPronoHENRYNo ratings yet
- Respiratoryfunctionandimportancetoanesthesia Final 140103050711 Phpapp02Document62 pagesRespiratoryfunctionandimportancetoanesthesia Final 140103050711 Phpapp02rijjorajooNo ratings yet
- 42 Respiratory Insufficiency-Pathophysiology, Diagnosis, Oxygen TherapyDocument73 pages42 Respiratory Insufficiency-Pathophysiology, Diagnosis, Oxygen TherapyLaila AcehNo ratings yet
- Pulmonary EdemaDocument5 pagesPulmonary EdemaMaris Angelica AyuyaoNo ratings yet
- Pulmonary Function TestDocument3 pagesPulmonary Function Testhm3398No ratings yet
- Interpretation On Pulmonary Function TestDocument105 pagesInterpretation On Pulmonary Function Testsalmamaged7619No ratings yet
- 231 FullDocument6 pages231 FullSuman DeyNo ratings yet
- Age-Related Changes in The Respiratory SystemDocument4 pagesAge-Related Changes in The Respiratory SystemSNo ratings yet
- Endothelial and Epithelial Barriers: Structure and FunctionDocument5 pagesEndothelial and Epithelial Barriers: Structure and FunctionLestariIrawanHadiNo ratings yet
- Ventilation Dead Space Ventilation Physiology of RespirationDocument55 pagesVentilation Dead Space Ventilation Physiology of RespirationkuhutansittinurhalizaNo ratings yet
- New Ventilators For The ICU-usefulness of Lung Performance ReportingDocument7 pagesNew Ventilators For The ICU-usefulness of Lung Performance ReportingAnonymous gXiDxwuJsNo ratings yet
- Measurement of Lung Volumes by Plethysmography: Ers/Ats Workshop Report SeriesDocument13 pagesMeasurement of Lung Volumes by Plethysmography: Ers/Ats Workshop Report SeriesCarlos Cortez MansillaNo ratings yet
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- Pulmonary Function Tests in Clinical PracticeFrom EverandPulmonary Function Tests in Clinical PracticeAli AltalagRating: 5 out of 5 stars5/5 (1)
- Lung Function in Health and Disease Basic Concepts of Respiratory Physiology and PathophysiologyFrom EverandLung Function in Health and Disease Basic Concepts of Respiratory Physiology and PathophysiologyNo ratings yet
- Monitoring Mechanical Ventilation Using Ventilator WaveformsFrom EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNo ratings yet
- Sliding Sidebar Menu in PowerPoint LiveDocument3 pagesSliding Sidebar Menu in PowerPoint LiveMonique BorresNo ratings yet
- Mandaloria NDocument5 pagesMandaloria NMonique BorresNo ratings yet
- Powerpoint Morph Animation Tutorial - Streched Photo TransitionDocument3 pagesPowerpoint Morph Animation Tutorial - Streched Photo TransitionMonique BorresNo ratings yet
- PowerPoint Image PlaceholdersDocument5 pagesPowerPoint Image PlaceholdersMonique BorresNo ratings yet
- CASE 1 Group 2 7 1Document4 pagesCASE 1 Group 2 7 1Monique BorresNo ratings yet
- BORRESDocument3 pagesBORRESMonique BorresNo ratings yet
- ScriptDocument4 pagesScriptMonique BorresNo ratings yet
- RespiDocument11 pagesRespiMonique BorresNo ratings yet
- Case ReportDocument16 pagesCase ReportMonique BorresNo ratings yet
- Urology Case Protocol PreceptorialDocument2 pagesUrology Case Protocol PreceptorialMonique BorresNo ratings yet
- INTEGRATION SESSION GROUPINGS FOR MD3 2022 2023 - Session 1 To 6Document3 pagesINTEGRATION SESSION GROUPINGS FOR MD3 2022 2023 - Session 1 To 6Monique BorresNo ratings yet
- Differential Diagnosis 3Document1 pageDifferential Diagnosis 3Monique BorresNo ratings yet
- IM-A PrePromo Removals Recall 2012Document3 pagesIM-A PrePromo Removals Recall 2012Monique BorresNo ratings yet
- CPC 2023 No TransitionDocument41 pagesCPC 2023 No TransitionMonique BorresNo ratings yet
- (2021) 1.1 Prelim Topics - Dra. YuloDocument10 pages(2021) 1.1 Prelim Topics - Dra. YuloMonique BorresNo ratings yet
- Bone Marrow ExaminationDocument31 pagesBone Marrow ExaminationMonique BorresNo ratings yet
- 0760modes of InheritanceDocument69 pages0760modes of InheritanceMonique Borres100% (1)
- NCP TBDocument7 pagesNCP TBLorraine CilloNo ratings yet
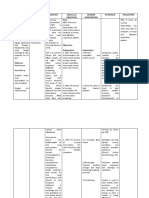
- Cues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalDocument4 pagesCues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalMonica Angelique SalayoNo ratings yet
- Mechanism of Breath Sounds ProductionDocument10 pagesMechanism of Breath Sounds ProductionMonica_azizaNo ratings yet
- Adult EDACP Patient Discharge Instructions - March20Document3 pagesAdult EDACP Patient Discharge Instructions - March20Takisha McpheeNo ratings yet
- Unacadmey Basic Organic Chemistry PDFDocument92 pagesUnacadmey Basic Organic Chemistry PDFAbhishek VermaNo ratings yet
- Msds tk21, CuredDocument3 pagesMsds tk21, CuredBachrul UlumNo ratings yet
- Chapter 2Document23 pagesChapter 2Nur ShahirahNo ratings yet
- NCP - CapDocument4 pagesNCP - CapSherryNo ratings yet
- Bronco Pulmonary SegmentDocument24 pagesBronco Pulmonary SegmentAnkit PancholiNo ratings yet
- Tracheobronchial LN EnlargementDocument6 pagesTracheobronchial LN EnlargementKarla FeliuNo ratings yet
- Animal ScienceDocument94 pagesAnimal ScienceMarson Andrei DapanasNo ratings yet
- WHO Operational Protocols Diphtheria PDFDocument25 pagesWHO Operational Protocols Diphtheria PDFAnonymous hETtEBkk7No ratings yet
- ITE NOTES (AutoRecovered)Document17 pagesITE NOTES (AutoRecovered)claravhvuNo ratings yet
- Case Study Nasopharyngeal CancerDocument31 pagesCase Study Nasopharyngeal CancerMae UsquisaNo ratings yet
- Chapter - 14 The Respiratory System PDFDocument7 pagesChapter - 14 The Respiratory System PDFben martin100% (1)
- Substance Use and Abuse For Students 2018-2019Document50 pagesSubstance Use and Abuse For Students 2018-2019ZauraNo ratings yet
- NCP Ineffective AirwayDocument3 pagesNCP Ineffective AirwayCat San Gabriel AmuraoNo ratings yet
- A Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Document10 pagesA Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Janina RojoNo ratings yet
- Msds H2 SO4Document7 pagesMsds H2 SO4Nur HabibahNo ratings yet
- NCP NminDocument5 pagesNCP NminkrizziajNo ratings yet
- Bronchial AshthmaDocument116 pagesBronchial Ashthmashaikh shabistaNo ratings yet
- Angle Orthod. 2019 89 5 713-20Document8 pagesAngle Orthod. 2019 89 5 713-20brookortontiaNo ratings yet
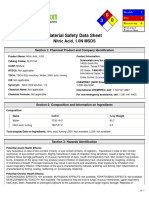
- Nitric Acid PDFDocument6 pagesNitric Acid PDFshella168No ratings yet
- Nbme 16Document14 pagesNbme 16Maneesh Gaddam67% (3)
- Lung SoundsDocument6 pagesLung SoundsQuinn Madalang100% (1)
- Anaphy Reviiewer - RabeDocument16 pagesAnaphy Reviiewer - RabeAyessa Marie BarbosaNo ratings yet
- Respiratory System PhysiologyDocument15 pagesRespiratory System Physiologymonster monNo ratings yet







































































































Download as pdf or txt
You might also like
- Swedish MassageDocument45 pagesSwedish MassageLawrence Cada Nofies100% (6)
- Case Study - Congestive Heart FailureDocument71 pagesCase Study - Congestive Heart FailureFrancis Adrian100% (3)
- Nursing Care Plan For Acute BronchitisDocument6 pagesNursing Care Plan For Acute BronchitisNur Panca Retnaningsih50% (2)
- Curvas Interpretacion Clinica 4Document9 pagesCurvas Interpretacion Clinica 4Patty MArivel ReinosoNo ratings yet
- Jcinvest00338 0038Document8 pagesJcinvest00338 0038Priyadharshini KumarNo ratings yet
- 1.B.09 Resp TestsDocument2 pages1.B.09 Resp Testsalemante100% (1)
- Anesth in Advanced Vent SupportDocument14 pagesAnesth in Advanced Vent SupportFrancisco DuqueNo ratings yet
- 2017 Article 84Document12 pages2017 Article 84flik_gantengNo ratings yet
- Respiratory ICU PDFDocument130 pagesRespiratory ICU PDFAhmed Shihab AhmedNo ratings yet
- Jcinvest00633 0061Document9 pagesJcinvest00633 0061Ravikiran SuryanarayanamurthyNo ratings yet
- Mechanical Ventilation - Chapter 1Document8 pagesMechanical Ventilation - Chapter 1Raninda JuliantiNo ratings yet
- Physiology of Mechanical VentilationDocument12 pagesPhysiology of Mechanical VentilationCarlos ZepedaNo ratings yet
- Respiratory Insufficiency - Pathophysiology,: Diagnosis, Oxygen TherapyDocument11 pagesRespiratory Insufficiency - Pathophysiology,: Diagnosis, Oxygen TherapyBintang UbamnataNo ratings yet
- Mechvent Presentation Midterm To FinalsDocument38 pagesMechvent Presentation Midterm To Finalsfloremie carinoNo ratings yet
- Interpreting Pulmonary Function TestsDocument10 pagesInterpreting Pulmonary Function TestsSuresh Kumar100% (1)
- Module 1 (AEP) - Section 2Document33 pagesModule 1 (AEP) - Section 2asimhafiz0044No ratings yet
- Restrictive Lung DisordersDocument5 pagesRestrictive Lung DisordersSonali RajputNo ratings yet
- Chapter 1 Respiratory System Nomenclature and Ambient ConditionsDocument9 pagesChapter 1 Respiratory System Nomenclature and Ambient Conditionsaisyahasrii_No ratings yet
- Influence of Cardiomegaly On Disordered Breathing During Exercise in Chronic Heart FailureDocument8 pagesInfluence of Cardiomegaly On Disordered Breathing During Exercise in Chronic Heart FailurenadiaNo ratings yet
- Pathophysiology and Classification of Respiratory Failure. Tejpreet Singh Lamba. 2016Document9 pagesPathophysiology and Classification of Respiratory Failure. Tejpreet Singh Lamba. 2016Danitza VeraNo ratings yet
- Atm 06 19 392 PDFDocument13 pagesAtm 06 19 392 PDFPetyr GoranovNo ratings yet
- 24 - Physiology of The Respiratory System PDFDocument38 pages24 - Physiology of The Respiratory System PDFlovelyc95No ratings yet
- The Effects of Lung Recruitment On The Phase III.26Document9 pagesThe Effects of Lung Recruitment On The Phase III.26Fermin LombardiaNo ratings yet
- Oxygen CascadeDocument12 pagesOxygen Cascadehy3pjb1984No ratings yet
- Respiratory Phsysiology 2nd Edition - A - Answers To Self-Study ProbDocument6 pagesRespiratory Phsysiology 2nd Edition - A - Answers To Self-Study ProbRonny Araya AbarcaNo ratings yet
- Jonkman2022 Article LungRecruitmentDocument3 pagesJonkman2022 Article LungRecruitmentCarolina Aguilar OtáloraNo ratings yet
- Atm 06 19 389Document9 pagesAtm 06 19 389Carlos QuirogaNo ratings yet
- EmfizemDocument4 pagesEmfizemJelenaJankovNo ratings yet
- P V Courve in ArdsDocument5 pagesP V Courve in ArdsAdrian BălanNo ratings yet
- Physiology of Respiration 2Document31 pagesPhysiology of Respiration 2kuhutansittinurhalizaNo ratings yet
- Спирометрия Глава 15Document81 pagesСпирометрия Глава 15Mikhail PisarevNo ratings yet
- Respiratory Monitoring Arterial Blood Gas Analysis Pulse Oximetry and End Tida Carbon Dioxide AnalysisDocument4 pagesRespiratory Monitoring Arterial Blood Gas Analysis Pulse Oximetry and End Tida Carbon Dioxide AnalysiskradoNo ratings yet
- Lung Tissue Resistance in Diffuse Interstitial Pulmonary FibrosisDocument9 pagesLung Tissue Resistance in Diffuse Interstitial Pulmonary FibrosisEndhy KurniawanNo ratings yet
- Lung Hyperinflation in COPD: Applying Physiology To Clinical PracticeDocument12 pagesLung Hyperinflation in COPD: Applying Physiology To Clinical PracticeJaya Semara PutraNo ratings yet
- 6 - Glossary - PactDocument7 pages6 - Glossary - PactSanj.etcNo ratings yet
- Respiratory FailureDocument7 pagesRespiratory FailureJesse OnealNo ratings yet
- Manajemen VentiDocument2 pagesManajemen VentiBos AseNo ratings yet
- Pumonary Function TestDocument24 pagesPumonary Function Testmerin sunilNo ratings yet
- Resp Physio SAQsDocument25 pagesResp Physio SAQsanaeshkl100% (1)
- Applsci 09 02842 PDFDocument13 pagesApplsci 09 02842 PDFFelicia SutarliNo ratings yet
- Principals of Mechanical Ventilation in Neonates: DR Mohd Maghayreh PRTH - IrbidDocument78 pagesPrincipals of Mechanical Ventilation in Neonates: DR Mohd Maghayreh PRTH - IrbidAnonymous 58LGc3No ratings yet
- Modes of Mechanical VentilationDocument4 pagesModes of Mechanical Ventilationsgod34100% (1)
- Respiration 473Document3 pagesRespiration 473api-315353725No ratings yet
- Mechanical VentilationDocument62 pagesMechanical Ventilationdrphaninadella100% (1)
- Basic Principles of Mechanical VentilationDocument34 pagesBasic Principles of Mechanical VentilationMohamed KorieshNo ratings yet
- PronoDocument14 pagesPronoHENRYNo ratings yet
- Respiratoryfunctionandimportancetoanesthesia Final 140103050711 Phpapp02Document62 pagesRespiratoryfunctionandimportancetoanesthesia Final 140103050711 Phpapp02rijjorajooNo ratings yet
- 42 Respiratory Insufficiency-Pathophysiology, Diagnosis, Oxygen TherapyDocument73 pages42 Respiratory Insufficiency-Pathophysiology, Diagnosis, Oxygen TherapyLaila AcehNo ratings yet
- Pulmonary EdemaDocument5 pagesPulmonary EdemaMaris Angelica AyuyaoNo ratings yet
- Pulmonary Function TestDocument3 pagesPulmonary Function Testhm3398No ratings yet
- Interpretation On Pulmonary Function TestDocument105 pagesInterpretation On Pulmonary Function Testsalmamaged7619No ratings yet
- 231 FullDocument6 pages231 FullSuman DeyNo ratings yet
- Age-Related Changes in The Respiratory SystemDocument4 pagesAge-Related Changes in The Respiratory SystemSNo ratings yet
- Endothelial and Epithelial Barriers: Structure and FunctionDocument5 pagesEndothelial and Epithelial Barriers: Structure and FunctionLestariIrawanHadiNo ratings yet
- Ventilation Dead Space Ventilation Physiology of RespirationDocument55 pagesVentilation Dead Space Ventilation Physiology of RespirationkuhutansittinurhalizaNo ratings yet
- New Ventilators For The ICU-usefulness of Lung Performance ReportingDocument7 pagesNew Ventilators For The ICU-usefulness of Lung Performance ReportingAnonymous gXiDxwuJsNo ratings yet
- Measurement of Lung Volumes by Plethysmography: Ers/Ats Workshop Report SeriesDocument13 pagesMeasurement of Lung Volumes by Plethysmography: Ers/Ats Workshop Report SeriesCarlos Cortez MansillaNo ratings yet
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- Pulmonary Function Tests in Clinical PracticeFrom EverandPulmonary Function Tests in Clinical PracticeAli AltalagRating: 5 out of 5 stars5/5 (1)
- Lung Function in Health and Disease Basic Concepts of Respiratory Physiology and PathophysiologyFrom EverandLung Function in Health and Disease Basic Concepts of Respiratory Physiology and PathophysiologyNo ratings yet
- Monitoring Mechanical Ventilation Using Ventilator WaveformsFrom EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNo ratings yet
- Sliding Sidebar Menu in PowerPoint LiveDocument3 pagesSliding Sidebar Menu in PowerPoint LiveMonique BorresNo ratings yet
- Mandaloria NDocument5 pagesMandaloria NMonique BorresNo ratings yet
- Powerpoint Morph Animation Tutorial - Streched Photo TransitionDocument3 pagesPowerpoint Morph Animation Tutorial - Streched Photo TransitionMonique BorresNo ratings yet
- PowerPoint Image PlaceholdersDocument5 pagesPowerPoint Image PlaceholdersMonique BorresNo ratings yet
- CASE 1 Group 2 7 1Document4 pagesCASE 1 Group 2 7 1Monique BorresNo ratings yet
- BORRESDocument3 pagesBORRESMonique BorresNo ratings yet
- ScriptDocument4 pagesScriptMonique BorresNo ratings yet
- RespiDocument11 pagesRespiMonique BorresNo ratings yet
- Case ReportDocument16 pagesCase ReportMonique BorresNo ratings yet
- Urology Case Protocol PreceptorialDocument2 pagesUrology Case Protocol PreceptorialMonique BorresNo ratings yet
- INTEGRATION SESSION GROUPINGS FOR MD3 2022 2023 - Session 1 To 6Document3 pagesINTEGRATION SESSION GROUPINGS FOR MD3 2022 2023 - Session 1 To 6Monique BorresNo ratings yet
- Differential Diagnosis 3Document1 pageDifferential Diagnosis 3Monique BorresNo ratings yet
- IM-A PrePromo Removals Recall 2012Document3 pagesIM-A PrePromo Removals Recall 2012Monique BorresNo ratings yet
- CPC 2023 No TransitionDocument41 pagesCPC 2023 No TransitionMonique BorresNo ratings yet
- (2021) 1.1 Prelim Topics - Dra. YuloDocument10 pages(2021) 1.1 Prelim Topics - Dra. YuloMonique BorresNo ratings yet
- Bone Marrow ExaminationDocument31 pagesBone Marrow ExaminationMonique BorresNo ratings yet
- 0760modes of InheritanceDocument69 pages0760modes of InheritanceMonique Borres100% (1)
- NCP TBDocument7 pagesNCP TBLorraine CilloNo ratings yet
- Cues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalDocument4 pagesCues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalMonica Angelique SalayoNo ratings yet
- Mechanism of Breath Sounds ProductionDocument10 pagesMechanism of Breath Sounds ProductionMonica_azizaNo ratings yet
- Adult EDACP Patient Discharge Instructions - March20Document3 pagesAdult EDACP Patient Discharge Instructions - March20Takisha McpheeNo ratings yet
- Unacadmey Basic Organic Chemistry PDFDocument92 pagesUnacadmey Basic Organic Chemistry PDFAbhishek VermaNo ratings yet
- Msds tk21, CuredDocument3 pagesMsds tk21, CuredBachrul UlumNo ratings yet
- Chapter 2Document23 pagesChapter 2Nur ShahirahNo ratings yet
- NCP - CapDocument4 pagesNCP - CapSherryNo ratings yet
- Bronco Pulmonary SegmentDocument24 pagesBronco Pulmonary SegmentAnkit PancholiNo ratings yet
- Tracheobronchial LN EnlargementDocument6 pagesTracheobronchial LN EnlargementKarla FeliuNo ratings yet
- Animal ScienceDocument94 pagesAnimal ScienceMarson Andrei DapanasNo ratings yet
- WHO Operational Protocols Diphtheria PDFDocument25 pagesWHO Operational Protocols Diphtheria PDFAnonymous hETtEBkk7No ratings yet
- ITE NOTES (AutoRecovered)Document17 pagesITE NOTES (AutoRecovered)claravhvuNo ratings yet
- Case Study Nasopharyngeal CancerDocument31 pagesCase Study Nasopharyngeal CancerMae UsquisaNo ratings yet
- Chapter - 14 The Respiratory System PDFDocument7 pagesChapter - 14 The Respiratory System PDFben martin100% (1)
- Substance Use and Abuse For Students 2018-2019Document50 pagesSubstance Use and Abuse For Students 2018-2019ZauraNo ratings yet
- NCP Ineffective AirwayDocument3 pagesNCP Ineffective AirwayCat San Gabriel AmuraoNo ratings yet
- A Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Document10 pagesA Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Janina RojoNo ratings yet
- Msds H2 SO4Document7 pagesMsds H2 SO4Nur HabibahNo ratings yet
- NCP NminDocument5 pagesNCP NminkrizziajNo ratings yet
- Bronchial AshthmaDocument116 pagesBronchial Ashthmashaikh shabistaNo ratings yet
- Angle Orthod. 2019 89 5 713-20Document8 pagesAngle Orthod. 2019 89 5 713-20brookortontiaNo ratings yet
- Nitric Acid PDFDocument6 pagesNitric Acid PDFshella168No ratings yet
- Nbme 16Document14 pagesNbme 16Maneesh Gaddam67% (3)
- Lung SoundsDocument6 pagesLung SoundsQuinn Madalang100% (1)
- Anaphy Reviiewer - RabeDocument16 pagesAnaphy Reviiewer - RabeAyessa Marie BarbosaNo ratings yet
- Respiratory System PhysiologyDocument15 pagesRespiratory System Physiologymonster monNo ratings yet