
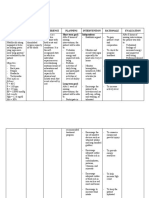
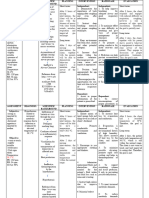
PNEUMONIA
PNEUMONIA
You might also like
- Nursing Management A. Nursing Care PlanDocument12 pagesNursing Management A. Nursing Care Planmabzbutterfly69% (13)
- NCP LeptospirosisDocument2 pagesNCP LeptospirosisLouise Anne Asuncion OclimaNo ratings yet
- Lesson Plan in Circulatory SystemDocument10 pagesLesson Plan in Circulatory SystemRey Sarsoza92% (38)
- HYPONATREMIADocument3 pagesHYPONATREMIADienizs Labini TadenaNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanJobelyn TunayNo ratings yet
- Renal Failure NCPDocument3 pagesRenal Failure NCPJet Ray-Ann GaringanNo ratings yet
- Fluid Volume Deficit Related To Loose Watery Stool Diarrhea)Document2 pagesFluid Volume Deficit Related To Loose Watery Stool Diarrhea)Jesse James Advincula Edjec100% (15)
- NCPDocument6 pagesNCPLevyanne GsanchezNo ratings yet
- Pae Clinical Case Week 8Document10 pagesPae Clinical Case Week 8ScribdTranslationsNo ratings yet
- Renal Failure NCPDocument3 pagesRenal Failure NCPjsksNo ratings yet
- Lacanlale, Kristle Anne F. BSN 1Y-2-Irr 1 Group 2: Assessment Diagnosis Planning Intervention EvaluationDocument4 pagesLacanlale, Kristle Anne F. BSN 1Y-2-Irr 1 Group 2: Assessment Diagnosis Planning Intervention EvaluationKristle Anne Federigan - LacanlaleNo ratings yet
- HydroceleDocument10 pagesHydroceleRyan ReNo ratings yet
- BSN2 C Ihps NCP FinalDocument7 pagesBSN2 C Ihps NCP FinalAdrian DecolongonNo ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation Short Term Goal: IndependentDocument4 pagesNursing Care Plan Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation Short Term Goal: IndependentasdasdasdNo ratings yet
- Prado, Catherine BSN IIB (Activity 1 Case Scenario)Document52 pagesPrado, Catherine BSN IIB (Activity 1 Case Scenario)Catherine PradoNo ratings yet
- Romero, Deinielle Ingrid M. (Hiv)Document8 pagesRomero, Deinielle Ingrid M. (Hiv)Deinielle Magdangal RomeroNo ratings yet
- C. Case Study thesis-NCP (Revised)Document5 pagesC. Case Study thesis-NCP (Revised)Lopirts NiganiNo ratings yet
- Hypovolemic Shock Sample NCPDocument14 pagesHypovolemic Shock Sample NCPRENEROSE TORRES100% (1)
- Medical Diagnosis: Chronic Kidney Disease Stage 5 Patient's NameDocument4 pagesMedical Diagnosis: Chronic Kidney Disease Stage 5 Patient's NameHadeer Mahmoud Abuslima100% (1)
- Assessment: Nursing Care PlanDocument3 pagesAssessment: Nursing Care PlanDana LabusonNo ratings yet
- NCP Med WingDocument4 pagesNCP Med WingACOB, Jamil C.No ratings yet
- Villanueva Bsn-1a - NcplecDocument6 pagesVillanueva Bsn-1a - NcplecKhyra Ysabelle VillanuevaNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationVince Adrian FiguracionNo ratings yet
- Breast Mass Bilateral To Consider FibroadenomaDocument5 pagesBreast Mass Bilateral To Consider FibroadenomaYum CNo ratings yet
- NCP Case Analysis GastritisDocument7 pagesNCP Case Analysis GastritisSteffi GolezNo ratings yet
- Gastroenteritis NCPDocument6 pagesGastroenteritis NCPKaguraNo ratings yet
- Gestational Diabetes - Case Study 2Document13 pagesGestational Diabetes - Case Study 2Bb RabbitNo ratings yet
- FHP - NCP - Kidney FailureDocument9 pagesFHP - NCP - Kidney FailureFrancis AdrianNo ratings yet
- Nursing Care Plan No. 2: Cue Nursing Diagnosis Desired Outcome Intervention Rationale EvaluationDocument2 pagesNursing Care Plan No. 2: Cue Nursing Diagnosis Desired Outcome Intervention Rationale EvaluationJIRAH MAY NAELGANo ratings yet
- NCP For Intranatal MotherDocument12 pagesNCP For Intranatal Motherpriyanka67% (6)
- Pedia NCPDocument6 pagesPedia NCPZel MartinezNo ratings yet
- ROSABIA, Micaela Pauline J. .-BSN-2A-ISDH-GS-NURSERY-NCPDocument6 pagesROSABIA, Micaela Pauline J. .-BSN-2A-ISDH-GS-NURSERY-NCPkimberly quitonNo ratings yet
- NCP Drug Study 2, Ojoy Dan Joshua LDocument4 pagesNCP Drug Study 2, Ojoy Dan Joshua Ldan.ojoy18No ratings yet
- Assessment Diagnosis Rationale Planning Intervention Rationale EvaluationDocument3 pagesAssessment Diagnosis Rationale Planning Intervention Rationale Evaluationbambem aevanNo ratings yet
- Ate Gabs Nyo Pagod NaDocument3 pagesAte Gabs Nyo Pagod NaGabrielle EvangelistaNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument7 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationpamelaideaNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationMina SumaoangNo ratings yet
- PDF NCP For Intranatal MotherDocument12 pagesPDF NCP For Intranatal MotherDaily DoseNo ratings yet
- NCP Nausea and VomitingDocument4 pagesNCP Nausea and VomitingKingJayson Pacman06No ratings yet
- NCP-SUGATON-HYPERTHERMIA IndivdualDocument2 pagesNCP-SUGATON-HYPERTHERMIA IndivdualPrincess Faniega SugatonNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term: Short TermDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term: Short TermLorie May GuillangNo ratings yet
- Sedation For Icu Patients PresentationDocument8 pagesSedation For Icu Patients Presentationapi-736869233No ratings yet
- Pneumonia Ni KevinDocument5 pagesPneumonia Ni Kevinjacobprince0016No ratings yet
- Case AbstractDocument11 pagesCase AbstractGovernance BookNo ratings yet
- Assessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective DataDocument2 pagesAssessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective DataCheila CruzNo ratings yet
- Community Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientDocument4 pagesCommunity Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientKrisianne Mae Lorenzo Francisco100% (1)
- Fluid Volume Deficit Related To Nausea and VomitDocument3 pagesFluid Volume Deficit Related To Nausea and VomitJakeNo ratings yet
- NCP (Actual and Risk) ERESDocument7 pagesNCP (Actual and Risk) ERESKAROL MARIAE LUZ ERESNo ratings yet
- Assesment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssesment Diagnosis Planning Intervention Rationale EvaluationTrisha Suazo100% (1)
- Nursing Care PlanDocument12 pagesNursing Care Plankeishaaa29100% (6)
- Short Term: Short TermDocument3 pagesShort Term: Short TermreolalasmjNo ratings yet
- UtsaDocument17 pagesUtsaCallie ParkNo ratings yet
- Nursing Care Plan Patient's Name: Age: Sex: Address:: Nursing-Notes/communicable - Diseases - Notes/amoebiasisDocument4 pagesNursing Care Plan Patient's Name: Age: Sex: Address:: Nursing-Notes/communicable - Diseases - Notes/amoebiasisGILIANNE MARIE JIMENEANo ratings yet
- NCP 3rd ROTATIONDocument17 pagesNCP 3rd ROTATIONMarie Ashley CasiaNo ratings yet
- NCP Dehydration (Fluid Volume Deficit)Document3 pagesNCP Dehydration (Fluid Volume Deficit)Charissa de LeonNo ratings yet
- NCP 4Document2 pagesNCP 4ako at ang exoNo ratings yet
- Fascinating Facts About Phytonutrients in Spices and Healthy Food: Scientifically Proven FactsFrom EverandFascinating Facts About Phytonutrients in Spices and Healthy Food: Scientifically Proven FactsNo ratings yet
- Heart of the Field "Refresher & Nha Certification Quick Notes"From EverandHeart of the Field "Refresher & Nha Certification Quick Notes"No ratings yet
- Community-Health-Nursing ReviewerDocument12 pagesCommunity-Health-Nursing ReviewerRica ParcasioNo ratings yet
- Pediatric Disorders at Risk and High Risk Newborn Infants 1Document25 pagesPediatric Disorders at Risk and High Risk Newborn Infants 1Rica ParcasioNo ratings yet
- Purposive Communication 3Document2 pagesPurposive Communication 3Rica ParcasioNo ratings yet
- Purposive Communication 1Document4 pagesPurposive Communication 1Rica ParcasioNo ratings yet
- NCM 108 - Ethical PrinciplesDocument17 pagesNCM 108 - Ethical PrinciplesRica ParcasioNo ratings yet
- Lec Framework Care of MotherDocument27 pagesLec Framework Care of MotherRica ParcasioNo ratings yet
- NCP Drug StudyDocument14 pagesNCP Drug StudyRica ParcasioNo ratings yet
- Sex SelectionDocument2 pagesSex SelectionRica ParcasioNo ratings yet
- NCP High Risk PregnancyDocument7 pagesNCP High Risk PregnancyRica ParcasioNo ratings yet
- Clinical Scenarios in ICUDocument107 pagesClinical Scenarios in ICUmatenten100% (4)
- Basic Health Research RiskesdasDocument359 pagesBasic Health Research RiskesdasDelia ShantyNo ratings yet
- High Blood Pleasure (HYPERTENSION) Symptoms and TreatmentDocument2 pagesHigh Blood Pleasure (HYPERTENSION) Symptoms and TreatmentmedibirdNo ratings yet
- Amlodipine - Drug Information - UpToDateDocument9 pagesAmlodipine - Drug Information - UpToDateBárbaraNo ratings yet
- NICE Pre EclampsiaDocument40 pagesNICE Pre EclampsiakazugawaNo ratings yet
- Cilnidipine Adverse Effect in Hypertensive Chronic Kidney Disease Patient With Pedal Edema A Case ReportDocument3 pagesCilnidipine Adverse Effect in Hypertensive Chronic Kidney Disease Patient With Pedal Edema A Case Reportvyshnavi machirajuNo ratings yet
- Nursing Care Plan - Cesarean SectionDocument1 pageNursing Care Plan - Cesarean SectionMarceline VueenNo ratings yet
- TNTP Health CardDocument4 pagesTNTP Health CardJennifer AlbaradoNo ratings yet
- Medical Surgical Nursing Pre-Test 2Document6 pagesMedical Surgical Nursing Pre-Test 2Blaine ManiegoNo ratings yet
- PDF JNC 8 Guidelines - CompressDocument2 pagesPDF JNC 8 Guidelines - Compressnaila inayatiNo ratings yet
- Unit 3Document10 pagesUnit 3korounganba4444No ratings yet
- Hubungan Kadar Gula Darah Dengan Hipertensi Pada Pasien Diabetes Mellitus Tipe 2 Di RSUP SanglahDocument4 pagesHubungan Kadar Gula Darah Dengan Hipertensi Pada Pasien Diabetes Mellitus Tipe 2 Di RSUP SanglahFauzan MuttaqinNo ratings yet
- Q&ADocument45 pagesQ&AElba De Asis Manacob0% (1)
- National High Blood Pressure Education Program Working Group Rep 1990Document22 pagesNational High Blood Pressure Education Program Working Group Rep 1990carlosarmijoNo ratings yet
- ADA Type 2 Diabetes in ChildrensDocument10 pagesADA Type 2 Diabetes in ChildrensCho Maharani Rijhigo BaeNo ratings yet
- Referral Paulina IrvinDocument3 pagesReferral Paulina IrvinPolAngelesNo ratings yet
- Lawsuit by Family of Darryl BectonDocument29 pagesLawsuit by Family of Darryl Bectonwamu885No ratings yet
- Drugs Used in The Management of Pre-EclampsiaDocument11 pagesDrugs Used in The Management of Pre-EclampsiaVenance NtengoNo ratings yet
- Ehad 883Document3 pagesEhad 883nhunhuochachNo ratings yet
- Isolated Systolic Hypertension in AdultDocument8 pagesIsolated Systolic Hypertension in AdultBkash ShahNo ratings yet
- Open Book Quiz 2Document12 pagesOpen Book Quiz 2bibisha hadidjaNo ratings yet
- Mill.) Terhadap Tekanan Darah Pasien Hipertensi Di WilayahDocument8 pagesMill.) Terhadap Tekanan Darah Pasien Hipertensi Di WilayahVivin MarscellaNo ratings yet
- Diagnostic Skills of Acupuncture: Lecture By: M.K. SastryDocument106 pagesDiagnostic Skills of Acupuncture: Lecture By: M.K. SastryLupa IngatanNo ratings yet
- La-Jin & Pai-Da (Enlgish) (1.0)Document8 pagesLa-Jin & Pai-Da (Enlgish) (1.0)David WeeNo ratings yet
- Hypertension in PregnancyDocument21 pagesHypertension in PregnancyIndah LatifahNo ratings yet
- Causes of AneurysmsDocument11 pagesCauses of AneurysmsMathew Ace M. OmilaNo ratings yet
- Hypertensive Renal DiseaseDocument2 pagesHypertensive Renal DiseaseHenry KaweesaNo ratings yet
- Notes On anti-HTN Drugs (Public Edition)Document17 pagesNotes On anti-HTN Drugs (Public Edition)Abdullah Al ArifNo ratings yet
- Pulmonary HypertensionDocument3 pagesPulmonary HypertensionJiezl Abellano AfinidadNo ratings yet
































































































Download as docx, pdf, or txt
You might also like
- Nursing Management A. Nursing Care PlanDocument12 pagesNursing Management A. Nursing Care Planmabzbutterfly69% (13)
- NCP LeptospirosisDocument2 pagesNCP LeptospirosisLouise Anne Asuncion OclimaNo ratings yet
- Lesson Plan in Circulatory SystemDocument10 pagesLesson Plan in Circulatory SystemRey Sarsoza92% (38)
- HYPONATREMIADocument3 pagesHYPONATREMIADienizs Labini TadenaNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanJobelyn TunayNo ratings yet
- Renal Failure NCPDocument3 pagesRenal Failure NCPJet Ray-Ann GaringanNo ratings yet
- Fluid Volume Deficit Related To Loose Watery Stool Diarrhea)Document2 pagesFluid Volume Deficit Related To Loose Watery Stool Diarrhea)Jesse James Advincula Edjec100% (15)
- NCPDocument6 pagesNCPLevyanne GsanchezNo ratings yet
- Pae Clinical Case Week 8Document10 pagesPae Clinical Case Week 8ScribdTranslationsNo ratings yet
- Renal Failure NCPDocument3 pagesRenal Failure NCPjsksNo ratings yet
- Lacanlale, Kristle Anne F. BSN 1Y-2-Irr 1 Group 2: Assessment Diagnosis Planning Intervention EvaluationDocument4 pagesLacanlale, Kristle Anne F. BSN 1Y-2-Irr 1 Group 2: Assessment Diagnosis Planning Intervention EvaluationKristle Anne Federigan - LacanlaleNo ratings yet
- HydroceleDocument10 pagesHydroceleRyan ReNo ratings yet
- BSN2 C Ihps NCP FinalDocument7 pagesBSN2 C Ihps NCP FinalAdrian DecolongonNo ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation Short Term Goal: IndependentDocument4 pagesNursing Care Plan Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation Short Term Goal: IndependentasdasdasdNo ratings yet
- Prado, Catherine BSN IIB (Activity 1 Case Scenario)Document52 pagesPrado, Catherine BSN IIB (Activity 1 Case Scenario)Catherine PradoNo ratings yet
- Romero, Deinielle Ingrid M. (Hiv)Document8 pagesRomero, Deinielle Ingrid M. (Hiv)Deinielle Magdangal RomeroNo ratings yet
- C. Case Study thesis-NCP (Revised)Document5 pagesC. Case Study thesis-NCP (Revised)Lopirts NiganiNo ratings yet
- Hypovolemic Shock Sample NCPDocument14 pagesHypovolemic Shock Sample NCPRENEROSE TORRES100% (1)
- Medical Diagnosis: Chronic Kidney Disease Stage 5 Patient's NameDocument4 pagesMedical Diagnosis: Chronic Kidney Disease Stage 5 Patient's NameHadeer Mahmoud Abuslima100% (1)
- Assessment: Nursing Care PlanDocument3 pagesAssessment: Nursing Care PlanDana LabusonNo ratings yet
- NCP Med WingDocument4 pagesNCP Med WingACOB, Jamil C.No ratings yet
- Villanueva Bsn-1a - NcplecDocument6 pagesVillanueva Bsn-1a - NcplecKhyra Ysabelle VillanuevaNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationVince Adrian FiguracionNo ratings yet
- Breast Mass Bilateral To Consider FibroadenomaDocument5 pagesBreast Mass Bilateral To Consider FibroadenomaYum CNo ratings yet
- NCP Case Analysis GastritisDocument7 pagesNCP Case Analysis GastritisSteffi GolezNo ratings yet
- Gastroenteritis NCPDocument6 pagesGastroenteritis NCPKaguraNo ratings yet
- Gestational Diabetes - Case Study 2Document13 pagesGestational Diabetes - Case Study 2Bb RabbitNo ratings yet
- FHP - NCP - Kidney FailureDocument9 pagesFHP - NCP - Kidney FailureFrancis AdrianNo ratings yet
- Nursing Care Plan No. 2: Cue Nursing Diagnosis Desired Outcome Intervention Rationale EvaluationDocument2 pagesNursing Care Plan No. 2: Cue Nursing Diagnosis Desired Outcome Intervention Rationale EvaluationJIRAH MAY NAELGANo ratings yet
- NCP For Intranatal MotherDocument12 pagesNCP For Intranatal Motherpriyanka67% (6)
- Pedia NCPDocument6 pagesPedia NCPZel MartinezNo ratings yet
- ROSABIA, Micaela Pauline J. .-BSN-2A-ISDH-GS-NURSERY-NCPDocument6 pagesROSABIA, Micaela Pauline J. .-BSN-2A-ISDH-GS-NURSERY-NCPkimberly quitonNo ratings yet
- NCP Drug Study 2, Ojoy Dan Joshua LDocument4 pagesNCP Drug Study 2, Ojoy Dan Joshua Ldan.ojoy18No ratings yet
- Assessment Diagnosis Rationale Planning Intervention Rationale EvaluationDocument3 pagesAssessment Diagnosis Rationale Planning Intervention Rationale Evaluationbambem aevanNo ratings yet
- Ate Gabs Nyo Pagod NaDocument3 pagesAte Gabs Nyo Pagod NaGabrielle EvangelistaNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument7 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationpamelaideaNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationMina SumaoangNo ratings yet
- PDF NCP For Intranatal MotherDocument12 pagesPDF NCP For Intranatal MotherDaily DoseNo ratings yet
- NCP Nausea and VomitingDocument4 pagesNCP Nausea and VomitingKingJayson Pacman06No ratings yet
- NCP-SUGATON-HYPERTHERMIA IndivdualDocument2 pagesNCP-SUGATON-HYPERTHERMIA IndivdualPrincess Faniega SugatonNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term: Short TermDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term: Short TermLorie May GuillangNo ratings yet
- Sedation For Icu Patients PresentationDocument8 pagesSedation For Icu Patients Presentationapi-736869233No ratings yet
- Pneumonia Ni KevinDocument5 pagesPneumonia Ni Kevinjacobprince0016No ratings yet
- Case AbstractDocument11 pagesCase AbstractGovernance BookNo ratings yet
- Assessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective DataDocument2 pagesAssessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective DataCheila CruzNo ratings yet
- Community Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientDocument4 pagesCommunity Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientKrisianne Mae Lorenzo Francisco100% (1)
- Fluid Volume Deficit Related To Nausea and VomitDocument3 pagesFluid Volume Deficit Related To Nausea and VomitJakeNo ratings yet
- NCP (Actual and Risk) ERESDocument7 pagesNCP (Actual and Risk) ERESKAROL MARIAE LUZ ERESNo ratings yet
- Assesment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssesment Diagnosis Planning Intervention Rationale EvaluationTrisha Suazo100% (1)
- Nursing Care PlanDocument12 pagesNursing Care Plankeishaaa29100% (6)
- Short Term: Short TermDocument3 pagesShort Term: Short TermreolalasmjNo ratings yet
- UtsaDocument17 pagesUtsaCallie ParkNo ratings yet
- Nursing Care Plan Patient's Name: Age: Sex: Address:: Nursing-Notes/communicable - Diseases - Notes/amoebiasisDocument4 pagesNursing Care Plan Patient's Name: Age: Sex: Address:: Nursing-Notes/communicable - Diseases - Notes/amoebiasisGILIANNE MARIE JIMENEANo ratings yet
- NCP 3rd ROTATIONDocument17 pagesNCP 3rd ROTATIONMarie Ashley CasiaNo ratings yet
- NCP Dehydration (Fluid Volume Deficit)Document3 pagesNCP Dehydration (Fluid Volume Deficit)Charissa de LeonNo ratings yet
- NCP 4Document2 pagesNCP 4ako at ang exoNo ratings yet
- Fascinating Facts About Phytonutrients in Spices and Healthy Food: Scientifically Proven FactsFrom EverandFascinating Facts About Phytonutrients in Spices and Healthy Food: Scientifically Proven FactsNo ratings yet
- Heart of the Field "Refresher & Nha Certification Quick Notes"From EverandHeart of the Field "Refresher & Nha Certification Quick Notes"No ratings yet
- Community-Health-Nursing ReviewerDocument12 pagesCommunity-Health-Nursing ReviewerRica ParcasioNo ratings yet
- Pediatric Disorders at Risk and High Risk Newborn Infants 1Document25 pagesPediatric Disorders at Risk and High Risk Newborn Infants 1Rica ParcasioNo ratings yet
- Purposive Communication 3Document2 pagesPurposive Communication 3Rica ParcasioNo ratings yet
- Purposive Communication 1Document4 pagesPurposive Communication 1Rica ParcasioNo ratings yet
- NCM 108 - Ethical PrinciplesDocument17 pagesNCM 108 - Ethical PrinciplesRica ParcasioNo ratings yet
- Lec Framework Care of MotherDocument27 pagesLec Framework Care of MotherRica ParcasioNo ratings yet
- NCP Drug StudyDocument14 pagesNCP Drug StudyRica ParcasioNo ratings yet
- Sex SelectionDocument2 pagesSex SelectionRica ParcasioNo ratings yet
- NCP High Risk PregnancyDocument7 pagesNCP High Risk PregnancyRica ParcasioNo ratings yet
- Clinical Scenarios in ICUDocument107 pagesClinical Scenarios in ICUmatenten100% (4)
- Basic Health Research RiskesdasDocument359 pagesBasic Health Research RiskesdasDelia ShantyNo ratings yet
- High Blood Pleasure (HYPERTENSION) Symptoms and TreatmentDocument2 pagesHigh Blood Pleasure (HYPERTENSION) Symptoms and TreatmentmedibirdNo ratings yet
- Amlodipine - Drug Information - UpToDateDocument9 pagesAmlodipine - Drug Information - UpToDateBárbaraNo ratings yet
- NICE Pre EclampsiaDocument40 pagesNICE Pre EclampsiakazugawaNo ratings yet
- Cilnidipine Adverse Effect in Hypertensive Chronic Kidney Disease Patient With Pedal Edema A Case ReportDocument3 pagesCilnidipine Adverse Effect in Hypertensive Chronic Kidney Disease Patient With Pedal Edema A Case Reportvyshnavi machirajuNo ratings yet
- Nursing Care Plan - Cesarean SectionDocument1 pageNursing Care Plan - Cesarean SectionMarceline VueenNo ratings yet
- TNTP Health CardDocument4 pagesTNTP Health CardJennifer AlbaradoNo ratings yet
- Medical Surgical Nursing Pre-Test 2Document6 pagesMedical Surgical Nursing Pre-Test 2Blaine ManiegoNo ratings yet
- PDF JNC 8 Guidelines - CompressDocument2 pagesPDF JNC 8 Guidelines - Compressnaila inayatiNo ratings yet
- Unit 3Document10 pagesUnit 3korounganba4444No ratings yet
- Hubungan Kadar Gula Darah Dengan Hipertensi Pada Pasien Diabetes Mellitus Tipe 2 Di RSUP SanglahDocument4 pagesHubungan Kadar Gula Darah Dengan Hipertensi Pada Pasien Diabetes Mellitus Tipe 2 Di RSUP SanglahFauzan MuttaqinNo ratings yet
- Q&ADocument45 pagesQ&AElba De Asis Manacob0% (1)
- National High Blood Pressure Education Program Working Group Rep 1990Document22 pagesNational High Blood Pressure Education Program Working Group Rep 1990carlosarmijoNo ratings yet
- ADA Type 2 Diabetes in ChildrensDocument10 pagesADA Type 2 Diabetes in ChildrensCho Maharani Rijhigo BaeNo ratings yet
- Referral Paulina IrvinDocument3 pagesReferral Paulina IrvinPolAngelesNo ratings yet
- Lawsuit by Family of Darryl BectonDocument29 pagesLawsuit by Family of Darryl Bectonwamu885No ratings yet
- Drugs Used in The Management of Pre-EclampsiaDocument11 pagesDrugs Used in The Management of Pre-EclampsiaVenance NtengoNo ratings yet
- Ehad 883Document3 pagesEhad 883nhunhuochachNo ratings yet
- Isolated Systolic Hypertension in AdultDocument8 pagesIsolated Systolic Hypertension in AdultBkash ShahNo ratings yet
- Open Book Quiz 2Document12 pagesOpen Book Quiz 2bibisha hadidjaNo ratings yet
- Mill.) Terhadap Tekanan Darah Pasien Hipertensi Di WilayahDocument8 pagesMill.) Terhadap Tekanan Darah Pasien Hipertensi Di WilayahVivin MarscellaNo ratings yet
- Diagnostic Skills of Acupuncture: Lecture By: M.K. SastryDocument106 pagesDiagnostic Skills of Acupuncture: Lecture By: M.K. SastryLupa IngatanNo ratings yet
- La-Jin & Pai-Da (Enlgish) (1.0)Document8 pagesLa-Jin & Pai-Da (Enlgish) (1.0)David WeeNo ratings yet
- Hypertension in PregnancyDocument21 pagesHypertension in PregnancyIndah LatifahNo ratings yet
- Causes of AneurysmsDocument11 pagesCauses of AneurysmsMathew Ace M. OmilaNo ratings yet
- Hypertensive Renal DiseaseDocument2 pagesHypertensive Renal DiseaseHenry KaweesaNo ratings yet
- Notes On anti-HTN Drugs (Public Edition)Document17 pagesNotes On anti-HTN Drugs (Public Edition)Abdullah Al ArifNo ratings yet
- Pulmonary HypertensionDocument3 pagesPulmonary HypertensionJiezl Abellano AfinidadNo ratings yet