
Journal Orthopaedic Research - 2006 - Beynnon - Ankle Ligament Injury Risk Factors A Prospective Study of College Athletes
Journal Orthopaedic Research - 2006 - Beynnon - Ankle Ligament Injury Risk Factors A Prospective Study of College Athletes
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Reproductive - Systems - in - Vertebrates ss2Document12 pagesReproductive - Systems - in - Vertebrates ss2Ezeh Princess100% (1)
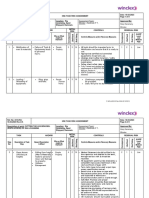
- 2318-RA 18.03.2023-REV 0A Cutting The Leg Bracing - RIG Rig LovansingDocument9 pages2318-RA 18.03.2023-REV 0A Cutting The Leg Bracing - RIG Rig LovansingHafeez AliNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Natuzza Evolo Mother Natuzza and Her Gifts Given by GodDocument7 pagesNatuzza Evolo Mother Natuzza and Her Gifts Given by GodNurli Girsang100% (1)
- Dsme Piping - Practice PDFDocument117 pagesDsme Piping - Practice PDFJesus PlacedesNo ratings yet
- Standard Welded Wire Mesh For Concrete ReinforcementDocument3 pagesStandard Welded Wire Mesh For Concrete Reinforcementmarksantana100% (2)
- Growth of The ESKD Population Progress or Peril .3Document2 pagesGrowth of The ESKD Population Progress or Peril .3Arista RachmaNo ratings yet
- Errata 36Document4 pagesErrata 36Arista RachmaNo ratings yet
- This Month S Highlights.38Document3 pagesThis Month S Highlights.38Arista RachmaNo ratings yet
- Nucleophosmin Phosphorylation As A Diagnostic And.9Document13 pagesNucleophosmin Phosphorylation As A Diagnostic And.9Arista RachmaNo ratings yet
- Asn News.39Document3 pagesAsn News.39Arista RachmaNo ratings yet
- The ADEMEX Study Make Haste Slowly.35Document4 pagesThe ADEMEX Study Make Haste Slowly.35Arista RachmaNo ratings yet
- Improving Clinical Outcomes in The Era Of.5Document6 pagesImproving Clinical Outcomes in The Era Of.5Arista RachmaNo ratings yet
- The Multiplication Principle As The Basis For.28Document21 pagesThe Multiplication Principle As The Basis For.28Arista RachmaNo ratings yet
- Expression Profiling of Fibroblasts in Chronic And.11Document15 pagesExpression Profiling of Fibroblasts in Chronic And.11Arista RachmaNo ratings yet
- The Quality of Reporting of Kidney Research A.2Document2 pagesThe Quality of Reporting of Kidney Research A.2Arista RachmaNo ratings yet
- Morphological Processes of Foot Process Effacement.12Document13 pagesMorphological Processes of Foot Process Effacement.12Arista RachmaNo ratings yet
- Dynamic Changes of The Total Pore Area Available.22Document6 pagesDynamic Changes of The Total Pore Area Available.22Arista RachmaNo ratings yet
- Endogenous Notch Signaling in Adult Kidneys.13Document17 pagesEndogenous Notch Signaling in Adult Kidneys.13Arista RachmaNo ratings yet
- Advantages of Single Nucleus Over Single Cell RNA.7Document10 pagesAdvantages of Single Nucleus Over Single Cell RNA.7Arista RachmaNo ratings yet
- Impaired Renal HCO3 Excretion in Cystic Fibrosis.12Document17 pagesImpaired Renal HCO3 Excretion in Cystic Fibrosis.12Arista RachmaNo ratings yet
- Effects of Dapagliflozin in Stage 4 Chronic Kidney.26Document10 pagesEffects of Dapagliflozin in Stage 4 Chronic Kidney.26Arista RachmaNo ratings yet
- Diagnosis and Treatment of Hyponatremia .7Document10 pagesDiagnosis and Treatment of Hyponatremia .7Arista RachmaNo ratings yet
- Retraction Central Role For Adipocyte Na, K ATPase.18Document2 pagesRetraction Central Role For Adipocyte Na, K ATPase.18Arista RachmaNo ratings yet
- Ultrastructural Evidence For Direct Renal.9Document5 pagesUltrastructural Evidence For Direct Renal.9Arista RachmaNo ratings yet
- Postoperative AKI Prevention Is Better Than Cure .4Document3 pagesPostoperative AKI Prevention Is Better Than Cure .4Arista RachmaNo ratings yet
- Acute Start Peritoneal Dialysis During The.8Document3 pagesAcute Start Peritoneal Dialysis During The.8Arista RachmaNo ratings yet
- AKI and Collapsing Glomerulopathy Associated With.10Document8 pagesAKI and Collapsing Glomerulopathy Associated With.10Arista RachmaNo ratings yet
- Anomalies of The TCF2 Gene Are The Main Cause Of.32Document11 pagesAnomalies of The TCF2 Gene Are The Main Cause Of.32Arista RachmaNo ratings yet
- HDDDDocument2 pagesHDDDArista RachmaNo ratings yet
- Urinary N Acetyl D Glucosaminidase Activity.30Document9 pagesUrinary N Acetyl D Glucosaminidase Activity.30Arista RachmaNo ratings yet
- Discovery of Autoantibodies Targeting Nephrin In.23Document15 pagesDiscovery of Autoantibodies Targeting Nephrin In.23Arista RachmaNo ratings yet
- Pathologic Classification of Diabetic Nephropathy.7Document8 pagesPathologic Classification of Diabetic Nephropathy.7Arista RachmaNo ratings yet
- Bicarbonate Therapy in Severe Metabolic Acidosis.7Document4 pagesBicarbonate Therapy in Severe Metabolic Acidosis.7Arista RachmaNo ratings yet
- Just Add Water.1Document3 pagesJust Add Water.1Arista RachmaNo ratings yet
- When Is It Appropriate To Order An Ionized.6Document4 pagesWhen Is It Appropriate To Order An Ionized.6Arista RachmaNo ratings yet
- 1986 GT CatalogDocument16 pages1986 GT CatalogtspinnerNo ratings yet
- P.5 English Revision Set 2 Namagunga Primary Boarding SchoolDocument14 pagesP.5 English Revision Set 2 Namagunga Primary Boarding SchoolnkugwafavourNo ratings yet
- Thunder Cake StoryDocument5 pagesThunder Cake Storyapi-21226401No ratings yet
- TMO Journal Pantacle - 2001-1Document29 pagesTMO Journal Pantacle - 2001-1Frater T.A.S.100% (6)
- Clarke No Clarke Yes (Clexa)Document7 pagesClarke No Clarke Yes (Clexa)mercedesmgNo ratings yet
- Shapeshell - Steel Structure Painting Technical Specification 2020-02-10 PDFDocument4 pagesShapeshell - Steel Structure Painting Technical Specification 2020-02-10 PDFmorisNo ratings yet
- Do Dice Play GodDocument6 pagesDo Dice Play Godninafatima allamNo ratings yet
- Control Electrical Appliances Using PCDocument46 pagesControl Electrical Appliances Using PCsumit gandhi100% (1)
- Ropa2000 307Document4 pagesRopa2000 307HORACIONo ratings yet
- Moloney Johannine TheologyDocument20 pagesMoloney Johannine Theologygogel33% (3)
- Candito 6 Week Program 1Document22 pagesCandito 6 Week Program 1Melysunn ReevsNo ratings yet
- Riello G750 ManuelDocument21 pagesRiello G750 Manuelmelvin hoferNo ratings yet
- What Is The Production Process of Inorganic Pigment PowderDocument3 pagesWhat Is The Production Process of Inorganic Pigment Powderkinley dorjeeNo ratings yet
- AnswerDocument2 pagesAnswerHidayah TeacherNo ratings yet
- Private Cloud Appliance x9 DatasheetDocument3 pagesPrivate Cloud Appliance x9 DatasheetKesava ReddyNo ratings yet
- 1 - Restless Earth UPDATEDDocument4 pages1 - Restless Earth UPDATEDMROHANLONNo ratings yet
- Indian Childhood CirrhosisDocument20 pagesIndian Childhood Cirrhosissubinj_3100% (4)
- HW2 CIVE210 Equilibrium-Particles SOLUTIONDocument12 pagesHW2 CIVE210 Equilibrium-Particles SOLUTIONNNo ratings yet
- Clanbook Tremere (Revised Edition) (2000) WW2357 (With Bookmarks) (OEF)Document107 pagesClanbook Tremere (Revised Edition) (2000) WW2357 (With Bookmarks) (OEF)cwod100% (1)
- TM 9 2320 304 14 and PDocument1,321 pagesTM 9 2320 304 14 and PjordanloNo ratings yet
- Grade 3.strawberry Time - Posttest.silentDocument3 pagesGrade 3.strawberry Time - Posttest.silentJean Claudine Manday100% (1)
- Medicines Control Authority of ZimbabweDocument38 pagesMedicines Control Authority of ZimbabweBK RegulatoryNo ratings yet
- Lesley Nair Thematic Summary of All You ZombiesDocument3 pagesLesley Nair Thematic Summary of All You Zombiesnair1904No ratings yet
- LSB03277 en SpaceLYnk BrochureDocument7 pagesLSB03277 en SpaceLYnk BrochureBobeică Iustin CătălinNo ratings yet
- GR WU - 25th - 29 TH April, 2022Document10 pagesGR WU - 25th - 29 TH April, 2022Nishtha JainNo ratings yet


































































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Reproductive - Systems - in - Vertebrates ss2Document12 pagesReproductive - Systems - in - Vertebrates ss2Ezeh Princess100% (1)
- 2318-RA 18.03.2023-REV 0A Cutting The Leg Bracing - RIG Rig LovansingDocument9 pages2318-RA 18.03.2023-REV 0A Cutting The Leg Bracing - RIG Rig LovansingHafeez AliNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Natuzza Evolo Mother Natuzza and Her Gifts Given by GodDocument7 pagesNatuzza Evolo Mother Natuzza and Her Gifts Given by GodNurli Girsang100% (1)
- Dsme Piping - Practice PDFDocument117 pagesDsme Piping - Practice PDFJesus PlacedesNo ratings yet
- Standard Welded Wire Mesh For Concrete ReinforcementDocument3 pagesStandard Welded Wire Mesh For Concrete Reinforcementmarksantana100% (2)
- Growth of The ESKD Population Progress or Peril .3Document2 pagesGrowth of The ESKD Population Progress or Peril .3Arista RachmaNo ratings yet
- Errata 36Document4 pagesErrata 36Arista RachmaNo ratings yet
- This Month S Highlights.38Document3 pagesThis Month S Highlights.38Arista RachmaNo ratings yet
- Nucleophosmin Phosphorylation As A Diagnostic And.9Document13 pagesNucleophosmin Phosphorylation As A Diagnostic And.9Arista RachmaNo ratings yet
- Asn News.39Document3 pagesAsn News.39Arista RachmaNo ratings yet
- The ADEMEX Study Make Haste Slowly.35Document4 pagesThe ADEMEX Study Make Haste Slowly.35Arista RachmaNo ratings yet
- Improving Clinical Outcomes in The Era Of.5Document6 pagesImproving Clinical Outcomes in The Era Of.5Arista RachmaNo ratings yet
- The Multiplication Principle As The Basis For.28Document21 pagesThe Multiplication Principle As The Basis For.28Arista RachmaNo ratings yet
- Expression Profiling of Fibroblasts in Chronic And.11Document15 pagesExpression Profiling of Fibroblasts in Chronic And.11Arista RachmaNo ratings yet
- The Quality of Reporting of Kidney Research A.2Document2 pagesThe Quality of Reporting of Kidney Research A.2Arista RachmaNo ratings yet
- Morphological Processes of Foot Process Effacement.12Document13 pagesMorphological Processes of Foot Process Effacement.12Arista RachmaNo ratings yet
- Dynamic Changes of The Total Pore Area Available.22Document6 pagesDynamic Changes of The Total Pore Area Available.22Arista RachmaNo ratings yet
- Endogenous Notch Signaling in Adult Kidneys.13Document17 pagesEndogenous Notch Signaling in Adult Kidneys.13Arista RachmaNo ratings yet
- Advantages of Single Nucleus Over Single Cell RNA.7Document10 pagesAdvantages of Single Nucleus Over Single Cell RNA.7Arista RachmaNo ratings yet
- Impaired Renal HCO3 Excretion in Cystic Fibrosis.12Document17 pagesImpaired Renal HCO3 Excretion in Cystic Fibrosis.12Arista RachmaNo ratings yet
- Effects of Dapagliflozin in Stage 4 Chronic Kidney.26Document10 pagesEffects of Dapagliflozin in Stage 4 Chronic Kidney.26Arista RachmaNo ratings yet
- Diagnosis and Treatment of Hyponatremia .7Document10 pagesDiagnosis and Treatment of Hyponatremia .7Arista RachmaNo ratings yet
- Retraction Central Role For Adipocyte Na, K ATPase.18Document2 pagesRetraction Central Role For Adipocyte Na, K ATPase.18Arista RachmaNo ratings yet
- Ultrastructural Evidence For Direct Renal.9Document5 pagesUltrastructural Evidence For Direct Renal.9Arista RachmaNo ratings yet
- Postoperative AKI Prevention Is Better Than Cure .4Document3 pagesPostoperative AKI Prevention Is Better Than Cure .4Arista RachmaNo ratings yet
- Acute Start Peritoneal Dialysis During The.8Document3 pagesAcute Start Peritoneal Dialysis During The.8Arista RachmaNo ratings yet
- AKI and Collapsing Glomerulopathy Associated With.10Document8 pagesAKI and Collapsing Glomerulopathy Associated With.10Arista RachmaNo ratings yet
- Anomalies of The TCF2 Gene Are The Main Cause Of.32Document11 pagesAnomalies of The TCF2 Gene Are The Main Cause Of.32Arista RachmaNo ratings yet
- HDDDDocument2 pagesHDDDArista RachmaNo ratings yet
- Urinary N Acetyl D Glucosaminidase Activity.30Document9 pagesUrinary N Acetyl D Glucosaminidase Activity.30Arista RachmaNo ratings yet
- Discovery of Autoantibodies Targeting Nephrin In.23Document15 pagesDiscovery of Autoantibodies Targeting Nephrin In.23Arista RachmaNo ratings yet
- Pathologic Classification of Diabetic Nephropathy.7Document8 pagesPathologic Classification of Diabetic Nephropathy.7Arista RachmaNo ratings yet
- Bicarbonate Therapy in Severe Metabolic Acidosis.7Document4 pagesBicarbonate Therapy in Severe Metabolic Acidosis.7Arista RachmaNo ratings yet
- Just Add Water.1Document3 pagesJust Add Water.1Arista RachmaNo ratings yet
- When Is It Appropriate To Order An Ionized.6Document4 pagesWhen Is It Appropriate To Order An Ionized.6Arista RachmaNo ratings yet
- 1986 GT CatalogDocument16 pages1986 GT CatalogtspinnerNo ratings yet
- P.5 English Revision Set 2 Namagunga Primary Boarding SchoolDocument14 pagesP.5 English Revision Set 2 Namagunga Primary Boarding SchoolnkugwafavourNo ratings yet
- Thunder Cake StoryDocument5 pagesThunder Cake Storyapi-21226401No ratings yet
- TMO Journal Pantacle - 2001-1Document29 pagesTMO Journal Pantacle - 2001-1Frater T.A.S.100% (6)
- Clarke No Clarke Yes (Clexa)Document7 pagesClarke No Clarke Yes (Clexa)mercedesmgNo ratings yet
- Shapeshell - Steel Structure Painting Technical Specification 2020-02-10 PDFDocument4 pagesShapeshell - Steel Structure Painting Technical Specification 2020-02-10 PDFmorisNo ratings yet
- Do Dice Play GodDocument6 pagesDo Dice Play Godninafatima allamNo ratings yet
- Control Electrical Appliances Using PCDocument46 pagesControl Electrical Appliances Using PCsumit gandhi100% (1)
- Ropa2000 307Document4 pagesRopa2000 307HORACIONo ratings yet
- Moloney Johannine TheologyDocument20 pagesMoloney Johannine Theologygogel33% (3)
- Candito 6 Week Program 1Document22 pagesCandito 6 Week Program 1Melysunn ReevsNo ratings yet
- Riello G750 ManuelDocument21 pagesRiello G750 Manuelmelvin hoferNo ratings yet
- What Is The Production Process of Inorganic Pigment PowderDocument3 pagesWhat Is The Production Process of Inorganic Pigment Powderkinley dorjeeNo ratings yet
- AnswerDocument2 pagesAnswerHidayah TeacherNo ratings yet
- Private Cloud Appliance x9 DatasheetDocument3 pagesPrivate Cloud Appliance x9 DatasheetKesava ReddyNo ratings yet
- 1 - Restless Earth UPDATEDDocument4 pages1 - Restless Earth UPDATEDMROHANLONNo ratings yet
- Indian Childhood CirrhosisDocument20 pagesIndian Childhood Cirrhosissubinj_3100% (4)
- HW2 CIVE210 Equilibrium-Particles SOLUTIONDocument12 pagesHW2 CIVE210 Equilibrium-Particles SOLUTIONNNo ratings yet
- Clanbook Tremere (Revised Edition) (2000) WW2357 (With Bookmarks) (OEF)Document107 pagesClanbook Tremere (Revised Edition) (2000) WW2357 (With Bookmarks) (OEF)cwod100% (1)
- TM 9 2320 304 14 and PDocument1,321 pagesTM 9 2320 304 14 and PjordanloNo ratings yet
- Grade 3.strawberry Time - Posttest.silentDocument3 pagesGrade 3.strawberry Time - Posttest.silentJean Claudine Manday100% (1)
- Medicines Control Authority of ZimbabweDocument38 pagesMedicines Control Authority of ZimbabweBK RegulatoryNo ratings yet
- Lesley Nair Thematic Summary of All You ZombiesDocument3 pagesLesley Nair Thematic Summary of All You Zombiesnair1904No ratings yet
- LSB03277 en SpaceLYnk BrochureDocument7 pagesLSB03277 en SpaceLYnk BrochureBobeică Iustin CătălinNo ratings yet
- GR WU - 25th - 29 TH April, 2022Document10 pagesGR WU - 25th - 29 TH April, 2022Nishtha JainNo ratings yet