
Critical Care of The Vascular Surgery Patient
Critical Care of The Vascular Surgery Patient
You might also like
- Fat Bees Skinny BeesDocument150 pagesFat Bees Skinny BeesAdam Barbarossa100% (2)
- Cardiovascular System PhysiologyDocument109 pagesCardiovascular System PhysiologyKing kakaNo ratings yet
- Neurointerventional Management - Diagnosis and Treatment 2ed.Document647 pagesNeurointerventional Management - Diagnosis and Treatment 2ed.Herbert Baquerizo Vargas100% (2)
- Eficacia Del FlowaveDocument6 pagesEficacia Del FlowaveLISFLOWERNo ratings yet
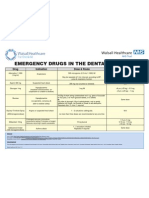
- Emergency Drugs Poster - Layout 1 in Dental PracticeDocument1 pageEmergency Drugs Poster - Layout 1 in Dental PracticeFady AtefNo ratings yet
- Balloon Angioplasty of Infrapopliteal Arteries - A Systematic Review and Proposed Algorithm For Optimal Endovascular TherapyDocument18 pagesBalloon Angioplasty of Infrapopliteal Arteries - A Systematic Review and Proposed Algorithm For Optimal Endovascular TherapyMárcio MacedoNo ratings yet
- Kuliah EmergensiDocument66 pagesKuliah EmergensiRifqi RamdhaniNo ratings yet
- 3 Soft Tissue Injury HabtamuDocument80 pages3 Soft Tissue Injury HabtamuWasihunNo ratings yet
- Lymphedema ReviewDocument8 pagesLymphedema ReviewSAKAI69No ratings yet
- Varicose Vein Treatment Tips and Trick - Ablation or GlueDocument30 pagesVaricose Vein Treatment Tips and Trick - Ablation or GlueNata NakamuraNo ratings yet
- Abdominal Wall SurgeryDocument4 pagesAbdominal Wall Surgeryjegan555No ratings yet
- 2carotid ArteryDocument57 pages2carotid ArteryShivik PatelNo ratings yet
- 7-Postoperative Care and ComplicationsDocument25 pages7-Postoperative Care and ComplicationsAiden JosephatNo ratings yet
- Intestinal ObstructionDocument15 pagesIntestinal ObstructionEmmeline Dycangchon-GarmaNo ratings yet
- Thoracic IncisionsDocument10 pagesThoracic IncisionsRadioputro WicaksonoNo ratings yet
- Redo CabgDocument36 pagesRedo CabgSantanico De CVT deozaNo ratings yet
- FinalDocument39 pagesFinalAmeerNo ratings yet
- Non Operative Fracture Management: Splint and CastDocument78 pagesNon Operative Fracture Management: Splint and CastSaeda AhmedNo ratings yet
- Scalp Block and Cervical Plexus Block Techniques - UpToDateDocument28 pagesScalp Block and Cervical Plexus Block Techniques - UpToDateAna Belén Artero CastañoNo ratings yet
- Sclerotherapy German GuidelinesDocument8 pagesSclerotherapy German GuidelinesGabriela DrăgoiNo ratings yet
- Vascular Disease Approach 11-7-13Document65 pagesVascular Disease Approach 11-7-13Dian PuspaNo ratings yet
- TULUA Lipoabdominoplasty 2020Document18 pagesTULUA Lipoabdominoplasty 2020Antonio Cardenas100% (1)
- Centrally Mediated Abdominal Pain SyndromesDocument4 pagesCentrally Mediated Abdominal Pain SyndromesPolo Good BoyNo ratings yet
- 59 Minimally Invasive CV Surgery and ECMODocument7 pages59 Minimally Invasive CV Surgery and ECMOVictor PazNo ratings yet
- Endovascular Revascularization and FreeDocument8 pagesEndovascular Revascularization and FreeNewLo0kNo ratings yet
- Anesthesia in Day Care PDFDocument15 pagesAnesthesia in Day Care PDFHKN nairNo ratings yet
- DVTDocument13 pagesDVTapi-253732526No ratings yet
- 5th Year Logbook August 2019Document15 pages5th Year Logbook August 2019Charity B JajiNo ratings yet
- Carcinoma Vulva - FinalDocument70 pagesCarcinoma Vulva - FinalAastha Jain100% (1)
- Surgical Intervention For Peripheral Arterial DiseaseDocument15 pagesSurgical Intervention For Peripheral Arterial DiseaseDewi NurNo ratings yet
- Acls 2022Document50 pagesAcls 2022Hoàng Luân BùiNo ratings yet
- SurgeryDocument13 pagesSurgerykarendelarosa06100% (2)
- Lower Extremity RevascularizationDocument9 pagesLower Extremity RevascularizationleagagaNo ratings yet
- Soft - Tissue 4.1.0.0.REL CAPCPDocument21 pagesSoft - Tissue 4.1.0.0.REL CAPCPaNo ratings yet
- Chordal Preservation TechniquesDocument8 pagesChordal Preservation TechniquesKunwar Sidharth SaurabhNo ratings yet
- Antibiotic Guidelines For AdultsDocument9 pagesAntibiotic Guidelines For AdultsVarshini Tamil SelvanNo ratings yet
- Bailey & Love Bailey & Love Bailey & Love Bailey & Love Bailey & Love Bailey & LoveDocument12 pagesBailey & Love Bailey & Love Bailey & Love Bailey & Love Bailey & Love Bailey & LoveSaifianNo ratings yet
- Umbilicalherniarepair: Overview of Approaches and Review of LiteratureDocument16 pagesUmbilicalherniarepair: Overview of Approaches and Review of LiteratureVictor Matias BarriosNo ratings yet
- Wound Care: Supplementary MaterialsDocument24 pagesWound Care: Supplementary MaterialsSuzanne100% (1)
- Drug Coasted Balloon Angioplasty Compared With Uncoated Balloons in The Treatment of Infrapopliteal Artery LesionsDocument7 pagesDrug Coasted Balloon Angioplasty Compared With Uncoated Balloons in The Treatment of Infrapopliteal Artery Lesionslia indria watiNo ratings yet
- Vascular AccessDocument49 pagesVascular Accessঅনুপম দাশNo ratings yet
- Modified Jobe Versus Docking Technique For Elbow Ulnar Collateral Ligament ReconstructionDocument13 pagesModified Jobe Versus Docking Technique For Elbow Ulnar Collateral Ligament ReconstructionLuisFernandoDelRíoEspinozaNo ratings yet
- Protocol For The Examination of Specimens From Patients With Plasma Cell NeoplasmsDocument12 pagesProtocol For The Examination of Specimens From Patients With Plasma Cell NeoplasmsMaikka IlaganNo ratings yet
- Mitral StenosisDocument67 pagesMitral StenosisNamithaNo ratings yet
- Diabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSDocument20 pagesDiabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSPrashant LokhandeNo ratings yet
- Clinical Surgery in General RCS Course ManualDocument2 pagesClinical Surgery in General RCS Course ManualsafiNo ratings yet
- NPWT Renasys and Pico Clinical GuidelinesDocument78 pagesNPWT Renasys and Pico Clinical GuidelinesArdianto SucintaNo ratings yet
- Rotarex IFUDocument5 pagesRotarex IFURemon NassimNo ratings yet
- Opthal Instruments: by Dr. Nigam Rashmi Dhar For Free PDF, Ebooks, Notes, MCQ Join Free Whatsapp Medical GRP 009779804202884Document58 pagesOpthal Instruments: by Dr. Nigam Rashmi Dhar For Free PDF, Ebooks, Notes, MCQ Join Free Whatsapp Medical GRP 009779804202884Ram sarenNo ratings yet
- Histology Uestions From LecturioDocument80 pagesHistology Uestions From LecturioChinyere OkoraforNo ratings yet
- Surgical Access IncisionsDocument7 pagesSurgical Access IncisionsFiliberto RiosNo ratings yet
- Eczema & Psoriasis: Dr. MburuDocument69 pagesEczema & Psoriasis: Dr. MburuKeith OmwoyoNo ratings yet
- Anatomy FACEDocument11 pagesAnatomy FACEMilton quisbert paredesNo ratings yet
- Evaluacion Inicial Del Paciente QuemadoDocument12 pagesEvaluacion Inicial Del Paciente QuemadoRyan BNo ratings yet
- Lasers in SurgeryDocument22 pagesLasers in Surgerynuclearbrain11No ratings yet
- Biomechanics of Cervical SpineDocument58 pagesBiomechanics of Cervical SpinesanavoraNo ratings yet
- Chest Trauma: Annet Mary Mathew Anu Krishna Arathi.KDocument60 pagesChest Trauma: Annet Mary Mathew Anu Krishna Arathi.KAsif AbbasNo ratings yet
- Current Concepts in Lower Extremity Reconstruction.36Document15 pagesCurrent Concepts in Lower Extremity Reconstruction.36Aura RivasNo ratings yet
- CGHS RateListDocument45 pagesCGHS RateListSandip SharmaNo ratings yet
- Tipsy Avant ResumeDocument3 pagesTipsy Avant ResumeTIPSY ANTONYNo ratings yet
- Abdominal Aortic Aneurysms-EditDocument32 pagesAbdominal Aortic Aneurysms-EditrandikaNo ratings yet
- 25 Cardiovascular DiseaseDocument35 pages25 Cardiovascular DiseaseBramantyo NugrosNo ratings yet
- Additional File 1. Patient-Ventilator Asynchronies: Double CyclingDocument4 pagesAdditional File 1. Patient-Ventilator Asynchronies: Double CyclingHerbert Baquerizo VargasNo ratings yet
- Early Intervention Can Improve Clinical Outcome of Acute Interstitial PneumoniaDocument9 pagesEarly Intervention Can Improve Clinical Outcome of Acute Interstitial PneumoniaHerbert Baquerizo VargasNo ratings yet
- When Pressure Is Positive - A Literature Review of The Prehospital Use of Continous Positive Airway PressureDocument9 pagesWhen Pressure Is Positive - A Literature Review of The Prehospital Use of Continous Positive Airway PressureHerbert Baquerizo VargasNo ratings yet
- Critical Care Reviews Book 2017Document356 pagesCritical Care Reviews Book 2017Herbert Baquerizo VargasNo ratings yet
- Retroperitoneal Pelvic Packing in The Management of Hemodynamically Unstable Pelvic Fractures: A Level I Trauma Center ExperienceDocument8 pagesRetroperitoneal Pelvic Packing in The Management of Hemodynamically Unstable Pelvic Fractures: A Level I Trauma Center ExperienceHerbert Baquerizo VargasNo ratings yet
- Death, Dying, and End of Life: ResearchDocument1 pageDeath, Dying, and End of Life: ResearchHerbert Baquerizo VargasNo ratings yet
- Noninvasive Reduction of Open-Book Pelvic Fractures by Circumferential CompressionDocument7 pagesNoninvasive Reduction of Open-Book Pelvic Fractures by Circumferential CompressionHerbert Baquerizo VargasNo ratings yet
- ArticleDocument6 pagesArticleHerbert Baquerizo VargasNo ratings yet
- Preface Xi Nancy A. Collop: Number 3 JULY 2008Document4 pagesPreface Xi Nancy A. Collop: Number 3 JULY 2008Herbert Baquerizo VargasNo ratings yet
- Diagnosis and Management of Obesity Hypoventilation Syndrome in The ICUDocument17 pagesDiagnosis and Management of Obesity Hypoventilation Syndrome in The ICUHerbert Baquerizo VargasNo ratings yet
- Sleep and Mechanical VentilationDocument15 pagesSleep and Mechanical VentilationHerbert Baquerizo VargasNo ratings yet
- 2015 Genetics From Genes To Genomes 5th Edition 5th Edition Test BankDocument38 pages2015 Genetics From Genes To Genomes 5th Edition 5th Edition Test Bankzacharyjackson20051996pbd100% (45)
- Gsa PPDocument15 pagesGsa PPSheikh Sahil MobinNo ratings yet
- Correction of Intestinal Disbacteriosis in Children With Chronic Hepatitis B Associated With LambliasisDocument8 pagesCorrection of Intestinal Disbacteriosis in Children With Chronic Hepatitis B Associated With LambliasisCentral Asian StudiesNo ratings yet
- Neligan Vol 3 Chapter 03 MainDocument55 pagesNeligan Vol 3 Chapter 03 MainisabelNo ratings yet
- Orthodontics DDA 214: DR Shabeel PNDocument47 pagesOrthodontics DDA 214: DR Shabeel PNShabeel PnNo ratings yet
- PCCPDocument1 pagePCCPOliver TabagNo ratings yet
- Physical Properties of Skin and Its ApplicationsDocument94 pagesPhysical Properties of Skin and Its ApplicationsdrshilpibhadaniNo ratings yet
- Intermediate Biology Olympiad Question PaperDocument43 pagesIntermediate Biology Olympiad Question Paperkatie weiNo ratings yet
- Hazard - CaregivingDocument36 pagesHazard - CaregivingamitafcragereyesNo ratings yet
- Case Spina BifidaDocument5 pagesCase Spina Bifidaroseavy100% (1)
- Emotional DisturbanceDocument62 pagesEmotional Disturbanceapi-340604729No ratings yet
- Diseases Associated With The Various Organ SystemsDocument10 pagesDiseases Associated With The Various Organ SystemsKimh SampagNo ratings yet
- ETT Vs LMADocument33 pagesETT Vs LMAitaindrianiNo ratings yet
- Beyond MeatDocument14 pagesBeyond MeatNguyen Thu TraNo ratings yet
- Health Community January2012Document8 pagesHealth Community January2012cristilyn pangosfianNo ratings yet
- Community Acquired PneumoniaDocument17 pagesCommunity Acquired PneumoniaDaniel Puentes SánchezNo ratings yet
- Seminar 1Document41 pagesSeminar 1Aprillia Dian PertiwiNo ratings yet
- Pneumocystis CariniiDocument22 pagesPneumocystis CariniijNo ratings yet
- SEMINAR MEDIS HERMINA PADANG - DR - Berri Rahmadhoni, SpOGDocument17 pagesSEMINAR MEDIS HERMINA PADANG - DR - Berri Rahmadhoni, SpOGsiska paramitaNo ratings yet
- Examples On How To Write A Conclusion For A Research PaperDocument8 pagesExamples On How To Write A Conclusion For A Research PaperafeatoxmoNo ratings yet
- Botox HH TrainingDocument15 pagesBotox HH TrainingMohan J Reddy100% (5)
- Review of 2015 SPM BiologyDocument16 pagesReview of 2015 SPM BiologyMark CwmNo ratings yet
- A Short Guide To Occult SymbolsDocument25 pagesA Short Guide To Occult SymbolshezzypezzyNo ratings yet
- Heart MurmurDocument7 pagesHeart MurmurChuu Suen TayNo ratings yet
- 2.37 Rso Training Standard Syllabi For Training Courses On Radiological SafetyDocument96 pages2.37 Rso Training Standard Syllabi For Training Courses On Radiological SafetyashwiniNo ratings yet
- Disability Rights in IndiaDocument23 pagesDisability Rights in IndiaAnirban Saikia100% (1)
- Thyroid Function TestsDocument25 pagesThyroid Function TestsEva SinghNo ratings yet
- Histologi Integument - 2022 - Wo Audio-Dikonversi-DikompresiDocument50 pagesHistologi Integument - 2022 - Wo Audio-Dikonversi-DikompresiMsatriaNo ratings yet
- "Horse Care and Health" Brent KelleyDocument65 pages"Horse Care and Health" Brent KelleyIno-san Yamanaka100% (4)




































































































Download as pdf or txt
You might also like
- Fat Bees Skinny BeesDocument150 pagesFat Bees Skinny BeesAdam Barbarossa100% (2)
- Cardiovascular System PhysiologyDocument109 pagesCardiovascular System PhysiologyKing kakaNo ratings yet
- Neurointerventional Management - Diagnosis and Treatment 2ed.Document647 pagesNeurointerventional Management - Diagnosis and Treatment 2ed.Herbert Baquerizo Vargas100% (2)
- Eficacia Del FlowaveDocument6 pagesEficacia Del FlowaveLISFLOWERNo ratings yet
- Emergency Drugs Poster - Layout 1 in Dental PracticeDocument1 pageEmergency Drugs Poster - Layout 1 in Dental PracticeFady AtefNo ratings yet
- Balloon Angioplasty of Infrapopliteal Arteries - A Systematic Review and Proposed Algorithm For Optimal Endovascular TherapyDocument18 pagesBalloon Angioplasty of Infrapopliteal Arteries - A Systematic Review and Proposed Algorithm For Optimal Endovascular TherapyMárcio MacedoNo ratings yet
- Kuliah EmergensiDocument66 pagesKuliah EmergensiRifqi RamdhaniNo ratings yet
- 3 Soft Tissue Injury HabtamuDocument80 pages3 Soft Tissue Injury HabtamuWasihunNo ratings yet
- Lymphedema ReviewDocument8 pagesLymphedema ReviewSAKAI69No ratings yet
- Varicose Vein Treatment Tips and Trick - Ablation or GlueDocument30 pagesVaricose Vein Treatment Tips and Trick - Ablation or GlueNata NakamuraNo ratings yet
- Abdominal Wall SurgeryDocument4 pagesAbdominal Wall Surgeryjegan555No ratings yet
- 2carotid ArteryDocument57 pages2carotid ArteryShivik PatelNo ratings yet
- 7-Postoperative Care and ComplicationsDocument25 pages7-Postoperative Care and ComplicationsAiden JosephatNo ratings yet
- Intestinal ObstructionDocument15 pagesIntestinal ObstructionEmmeline Dycangchon-GarmaNo ratings yet
- Thoracic IncisionsDocument10 pagesThoracic IncisionsRadioputro WicaksonoNo ratings yet
- Redo CabgDocument36 pagesRedo CabgSantanico De CVT deozaNo ratings yet
- FinalDocument39 pagesFinalAmeerNo ratings yet
- Non Operative Fracture Management: Splint and CastDocument78 pagesNon Operative Fracture Management: Splint and CastSaeda AhmedNo ratings yet
- Scalp Block and Cervical Plexus Block Techniques - UpToDateDocument28 pagesScalp Block and Cervical Plexus Block Techniques - UpToDateAna Belén Artero CastañoNo ratings yet
- Sclerotherapy German GuidelinesDocument8 pagesSclerotherapy German GuidelinesGabriela DrăgoiNo ratings yet
- Vascular Disease Approach 11-7-13Document65 pagesVascular Disease Approach 11-7-13Dian PuspaNo ratings yet
- TULUA Lipoabdominoplasty 2020Document18 pagesTULUA Lipoabdominoplasty 2020Antonio Cardenas100% (1)
- Centrally Mediated Abdominal Pain SyndromesDocument4 pagesCentrally Mediated Abdominal Pain SyndromesPolo Good BoyNo ratings yet
- 59 Minimally Invasive CV Surgery and ECMODocument7 pages59 Minimally Invasive CV Surgery and ECMOVictor PazNo ratings yet
- Endovascular Revascularization and FreeDocument8 pagesEndovascular Revascularization and FreeNewLo0kNo ratings yet
- Anesthesia in Day Care PDFDocument15 pagesAnesthesia in Day Care PDFHKN nairNo ratings yet
- DVTDocument13 pagesDVTapi-253732526No ratings yet
- 5th Year Logbook August 2019Document15 pages5th Year Logbook August 2019Charity B JajiNo ratings yet
- Carcinoma Vulva - FinalDocument70 pagesCarcinoma Vulva - FinalAastha Jain100% (1)
- Surgical Intervention For Peripheral Arterial DiseaseDocument15 pagesSurgical Intervention For Peripheral Arterial DiseaseDewi NurNo ratings yet
- Acls 2022Document50 pagesAcls 2022Hoàng Luân BùiNo ratings yet
- SurgeryDocument13 pagesSurgerykarendelarosa06100% (2)
- Lower Extremity RevascularizationDocument9 pagesLower Extremity RevascularizationleagagaNo ratings yet
- Soft - Tissue 4.1.0.0.REL CAPCPDocument21 pagesSoft - Tissue 4.1.0.0.REL CAPCPaNo ratings yet
- Chordal Preservation TechniquesDocument8 pagesChordal Preservation TechniquesKunwar Sidharth SaurabhNo ratings yet
- Antibiotic Guidelines For AdultsDocument9 pagesAntibiotic Guidelines For AdultsVarshini Tamil SelvanNo ratings yet
- Bailey & Love Bailey & Love Bailey & Love Bailey & Love Bailey & Love Bailey & LoveDocument12 pagesBailey & Love Bailey & Love Bailey & Love Bailey & Love Bailey & Love Bailey & LoveSaifianNo ratings yet
- Umbilicalherniarepair: Overview of Approaches and Review of LiteratureDocument16 pagesUmbilicalherniarepair: Overview of Approaches and Review of LiteratureVictor Matias BarriosNo ratings yet
- Wound Care: Supplementary MaterialsDocument24 pagesWound Care: Supplementary MaterialsSuzanne100% (1)
- Drug Coasted Balloon Angioplasty Compared With Uncoated Balloons in The Treatment of Infrapopliteal Artery LesionsDocument7 pagesDrug Coasted Balloon Angioplasty Compared With Uncoated Balloons in The Treatment of Infrapopliteal Artery Lesionslia indria watiNo ratings yet
- Vascular AccessDocument49 pagesVascular Accessঅনুপম দাশNo ratings yet
- Modified Jobe Versus Docking Technique For Elbow Ulnar Collateral Ligament ReconstructionDocument13 pagesModified Jobe Versus Docking Technique For Elbow Ulnar Collateral Ligament ReconstructionLuisFernandoDelRíoEspinozaNo ratings yet
- Protocol For The Examination of Specimens From Patients With Plasma Cell NeoplasmsDocument12 pagesProtocol For The Examination of Specimens From Patients With Plasma Cell NeoplasmsMaikka IlaganNo ratings yet
- Mitral StenosisDocument67 pagesMitral StenosisNamithaNo ratings yet
- Diabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSDocument20 pagesDiabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSPrashant LokhandeNo ratings yet
- Clinical Surgery in General RCS Course ManualDocument2 pagesClinical Surgery in General RCS Course ManualsafiNo ratings yet
- NPWT Renasys and Pico Clinical GuidelinesDocument78 pagesNPWT Renasys and Pico Clinical GuidelinesArdianto SucintaNo ratings yet
- Rotarex IFUDocument5 pagesRotarex IFURemon NassimNo ratings yet
- Opthal Instruments: by Dr. Nigam Rashmi Dhar For Free PDF, Ebooks, Notes, MCQ Join Free Whatsapp Medical GRP 009779804202884Document58 pagesOpthal Instruments: by Dr. Nigam Rashmi Dhar For Free PDF, Ebooks, Notes, MCQ Join Free Whatsapp Medical GRP 009779804202884Ram sarenNo ratings yet
- Histology Uestions From LecturioDocument80 pagesHistology Uestions From LecturioChinyere OkoraforNo ratings yet
- Surgical Access IncisionsDocument7 pagesSurgical Access IncisionsFiliberto RiosNo ratings yet
- Eczema & Psoriasis: Dr. MburuDocument69 pagesEczema & Psoriasis: Dr. MburuKeith OmwoyoNo ratings yet
- Anatomy FACEDocument11 pagesAnatomy FACEMilton quisbert paredesNo ratings yet
- Evaluacion Inicial Del Paciente QuemadoDocument12 pagesEvaluacion Inicial Del Paciente QuemadoRyan BNo ratings yet
- Lasers in SurgeryDocument22 pagesLasers in Surgerynuclearbrain11No ratings yet
- Biomechanics of Cervical SpineDocument58 pagesBiomechanics of Cervical SpinesanavoraNo ratings yet
- Chest Trauma: Annet Mary Mathew Anu Krishna Arathi.KDocument60 pagesChest Trauma: Annet Mary Mathew Anu Krishna Arathi.KAsif AbbasNo ratings yet
- Current Concepts in Lower Extremity Reconstruction.36Document15 pagesCurrent Concepts in Lower Extremity Reconstruction.36Aura RivasNo ratings yet
- CGHS RateListDocument45 pagesCGHS RateListSandip SharmaNo ratings yet
- Tipsy Avant ResumeDocument3 pagesTipsy Avant ResumeTIPSY ANTONYNo ratings yet
- Abdominal Aortic Aneurysms-EditDocument32 pagesAbdominal Aortic Aneurysms-EditrandikaNo ratings yet
- 25 Cardiovascular DiseaseDocument35 pages25 Cardiovascular DiseaseBramantyo NugrosNo ratings yet
- Additional File 1. Patient-Ventilator Asynchronies: Double CyclingDocument4 pagesAdditional File 1. Patient-Ventilator Asynchronies: Double CyclingHerbert Baquerizo VargasNo ratings yet
- Early Intervention Can Improve Clinical Outcome of Acute Interstitial PneumoniaDocument9 pagesEarly Intervention Can Improve Clinical Outcome of Acute Interstitial PneumoniaHerbert Baquerizo VargasNo ratings yet
- When Pressure Is Positive - A Literature Review of The Prehospital Use of Continous Positive Airway PressureDocument9 pagesWhen Pressure Is Positive - A Literature Review of The Prehospital Use of Continous Positive Airway PressureHerbert Baquerizo VargasNo ratings yet
- Critical Care Reviews Book 2017Document356 pagesCritical Care Reviews Book 2017Herbert Baquerizo VargasNo ratings yet
- Retroperitoneal Pelvic Packing in The Management of Hemodynamically Unstable Pelvic Fractures: A Level I Trauma Center ExperienceDocument8 pagesRetroperitoneal Pelvic Packing in The Management of Hemodynamically Unstable Pelvic Fractures: A Level I Trauma Center ExperienceHerbert Baquerizo VargasNo ratings yet
- Death, Dying, and End of Life: ResearchDocument1 pageDeath, Dying, and End of Life: ResearchHerbert Baquerizo VargasNo ratings yet
- Noninvasive Reduction of Open-Book Pelvic Fractures by Circumferential CompressionDocument7 pagesNoninvasive Reduction of Open-Book Pelvic Fractures by Circumferential CompressionHerbert Baquerizo VargasNo ratings yet
- ArticleDocument6 pagesArticleHerbert Baquerizo VargasNo ratings yet
- Preface Xi Nancy A. Collop: Number 3 JULY 2008Document4 pagesPreface Xi Nancy A. Collop: Number 3 JULY 2008Herbert Baquerizo VargasNo ratings yet
- Diagnosis and Management of Obesity Hypoventilation Syndrome in The ICUDocument17 pagesDiagnosis and Management of Obesity Hypoventilation Syndrome in The ICUHerbert Baquerizo VargasNo ratings yet
- Sleep and Mechanical VentilationDocument15 pagesSleep and Mechanical VentilationHerbert Baquerizo VargasNo ratings yet
- 2015 Genetics From Genes To Genomes 5th Edition 5th Edition Test BankDocument38 pages2015 Genetics From Genes To Genomes 5th Edition 5th Edition Test Bankzacharyjackson20051996pbd100% (45)
- Gsa PPDocument15 pagesGsa PPSheikh Sahil MobinNo ratings yet
- Correction of Intestinal Disbacteriosis in Children With Chronic Hepatitis B Associated With LambliasisDocument8 pagesCorrection of Intestinal Disbacteriosis in Children With Chronic Hepatitis B Associated With LambliasisCentral Asian StudiesNo ratings yet
- Neligan Vol 3 Chapter 03 MainDocument55 pagesNeligan Vol 3 Chapter 03 MainisabelNo ratings yet
- Orthodontics DDA 214: DR Shabeel PNDocument47 pagesOrthodontics DDA 214: DR Shabeel PNShabeel PnNo ratings yet
- PCCPDocument1 pagePCCPOliver TabagNo ratings yet
- Physical Properties of Skin and Its ApplicationsDocument94 pagesPhysical Properties of Skin and Its ApplicationsdrshilpibhadaniNo ratings yet
- Intermediate Biology Olympiad Question PaperDocument43 pagesIntermediate Biology Olympiad Question Paperkatie weiNo ratings yet
- Hazard - CaregivingDocument36 pagesHazard - CaregivingamitafcragereyesNo ratings yet
- Case Spina BifidaDocument5 pagesCase Spina Bifidaroseavy100% (1)
- Emotional DisturbanceDocument62 pagesEmotional Disturbanceapi-340604729No ratings yet
- Diseases Associated With The Various Organ SystemsDocument10 pagesDiseases Associated With The Various Organ SystemsKimh SampagNo ratings yet
- ETT Vs LMADocument33 pagesETT Vs LMAitaindrianiNo ratings yet
- Beyond MeatDocument14 pagesBeyond MeatNguyen Thu TraNo ratings yet
- Health Community January2012Document8 pagesHealth Community January2012cristilyn pangosfianNo ratings yet
- Community Acquired PneumoniaDocument17 pagesCommunity Acquired PneumoniaDaniel Puentes SánchezNo ratings yet
- Seminar 1Document41 pagesSeminar 1Aprillia Dian PertiwiNo ratings yet
- Pneumocystis CariniiDocument22 pagesPneumocystis CariniijNo ratings yet
- SEMINAR MEDIS HERMINA PADANG - DR - Berri Rahmadhoni, SpOGDocument17 pagesSEMINAR MEDIS HERMINA PADANG - DR - Berri Rahmadhoni, SpOGsiska paramitaNo ratings yet
- Examples On How To Write A Conclusion For A Research PaperDocument8 pagesExamples On How To Write A Conclusion For A Research PaperafeatoxmoNo ratings yet
- Botox HH TrainingDocument15 pagesBotox HH TrainingMohan J Reddy100% (5)
- Review of 2015 SPM BiologyDocument16 pagesReview of 2015 SPM BiologyMark CwmNo ratings yet
- A Short Guide To Occult SymbolsDocument25 pagesA Short Guide To Occult SymbolshezzypezzyNo ratings yet
- Heart MurmurDocument7 pagesHeart MurmurChuu Suen TayNo ratings yet
- 2.37 Rso Training Standard Syllabi For Training Courses On Radiological SafetyDocument96 pages2.37 Rso Training Standard Syllabi For Training Courses On Radiological SafetyashwiniNo ratings yet
- Disability Rights in IndiaDocument23 pagesDisability Rights in IndiaAnirban Saikia100% (1)
- Thyroid Function TestsDocument25 pagesThyroid Function TestsEva SinghNo ratings yet
- Histologi Integument - 2022 - Wo Audio-Dikonversi-DikompresiDocument50 pagesHistologi Integument - 2022 - Wo Audio-Dikonversi-DikompresiMsatriaNo ratings yet
- "Horse Care and Health" Brent KelleyDocument65 pages"Horse Care and Health" Brent KelleyIno-san Yamanaka100% (4)