
Alliancehpsr Thailandabridgedprimasys PDF
Alliancehpsr Thailandabridgedprimasys PDF
You might also like
- Module 1 CHN 1Document15 pagesModule 1 CHN 1Danz KieNo ratings yet
- Family Welfare ProgrammeDocument19 pagesFamily Welfare ProgrammeMahesh Sahu100% (2)
- Primary Health Care Systems (Primasys) : Case Study From MexicoDocument16 pagesPrimary Health Care Systems (Primasys) : Case Study From MexicoEpi SidaNo ratings yet
- Primary Health Care Systems (Primasys) : Case Study From EthiopiaDocument12 pagesPrimary Health Care Systems (Primasys) : Case Study From EthiopiaMuluken TesfayeNo ratings yet
- Population PolicyDocument6 pagesPopulation PolicyIqra YameenNo ratings yet
- WHO HIS HSR 17.15 Eng PDFDocument12 pagesWHO HIS HSR 17.15 Eng PDFNebyuNo ratings yet
- Ing The Burden 2020-2015 16Document8 pagesIng The Burden 2020-2015 16EstreLLA ValenciaNo ratings yet
- dm2022 0082Document9 pagesdm2022 0082Harold Paulo MejiaNo ratings yet
- Gha 6 19650Document10 pagesGha 6 19650Betric HanNo ratings yet
- Universal Health Care Coverage Through Pluralistic Approaches: Experience From ThailandDocument27 pagesUniversal Health Care Coverage Through Pluralistic Approaches: Experience From ThailandThaworn SakunphanitNo ratings yet
- Philippine Pharmaceutical IndustryDocument103 pagesPhilippine Pharmaceutical IndustryVijay Kumar MunshiNo ratings yet
- ACS-Country-Report Tanzania PDFDocument31 pagesACS-Country-Report Tanzania PDFCapacita DesignNo ratings yet
- Cause Specific Mortality and Socioeconomic Status in Chakaria BangladeshDocument10 pagesCause Specific Mortality and Socioeconomic Status in Chakaria BangladeshSabujNo ratings yet
- DM No. 2022-0511 Reporting of ZOD - 03oct2022Document9 pagesDM No. 2022-0511 Reporting of ZOD - 03oct2022Catherine LargaNo ratings yet
- POPDEV (Basic Concepts)Document64 pagesPOPDEV (Basic Concepts)Paul Keene BonitaNo ratings yet
- FundingModel TBAndHIVConceptNote Final Ethiopia Oct15 2014Document94 pagesFundingModel TBAndHIVConceptNote Final Ethiopia Oct15 2014tokumaNo ratings yet
- LASI India Executive SummaryDocument52 pagesLASI India Executive SummaryNaudibya MajhiNo ratings yet
- Unfpa - Icomp Regional Consultation Family Planning in Asia and The Pacific Addressing The ChallengesDocument23 pagesUnfpa - Icomp Regional Consultation Family Planning in Asia and The Pacific Addressing The ChallengesYantoNo ratings yet
- FCHVDocument22 pagesFCHVSamzana ShresthaNo ratings yet
- Incentives and Disincentives: Necessary, Effective, Just?Document9 pagesIncentives and Disincentives: Necessary, Effective, Just?suman guptaNo ratings yet
- 077C10A61423Document14 pages077C10A61423Endy SitumbekoNo ratings yet
- DemographyDocument28 pagesDemographyAsad ullahNo ratings yet
- Document From Elle Final2Document18 pagesDocument From Elle Final2georgeNo ratings yet
- What Went Wrong With The Achievement of Replacement Fertility in Bangladesh and Its Consequences On The Demographic Dividend The Role of Proximate DeterminantsDocument24 pagesWhat Went Wrong With The Achievement of Replacement Fertility in Bangladesh and Its Consequences On The Demographic Dividend The Role of Proximate DeterminantsRussell KabirNo ratings yet
- Investing in Health: The Role of LGU Officials in Health Sector DevelopmentDocument58 pagesInvesting in Health: The Role of LGU Officials in Health Sector DevelopmentMaan Pastor MananzanNo ratings yet
- Vital Health StatisticsDocument71 pagesVital Health Statisticsritikaritika93% (14)
- Indonesia Packet Population PDFDocument65 pagesIndonesia Packet Population PDFMargareta Laura PattipeilohyNo ratings yet
- Population, Labour Force and EmploymentDocument11 pagesPopulation, Labour Force and EmploymentAsad RazaNo ratings yet
- Healthand Family Welfarestatisticsin India 201920Document253 pagesHealthand Family Welfarestatisticsin India 201920poonam valviNo ratings yet
- Fertility Trends in Bangladesh 2014Document13 pagesFertility Trends in Bangladesh 2014Rozen Tareque HasanNo ratings yet
- Asia-Pacific's Opportunity:: Investing To Avert An HIV/AIDS CrisisDocument20 pagesAsia-Pacific's Opportunity:: Investing To Avert An HIV/AIDS CrisismastahhhNo ratings yet
- 8-Point Action Agenda - The Medium-Term Strategy of The Health Sector For 2023-2028Document19 pages8-Point Action Agenda - The Medium-Term Strategy of The Health Sector For 2023-2028RURAL HEALTH CENTER TAMBLER BAWINGNo ratings yet
- WHO EURO 2020 1710 41461 56527 EngDocument15 pagesWHO EURO 2020 1710 41461 56527 EngBuffaloNo ratings yet
- Psa Gov PH Population and Housing Node 167965Document4 pagesPsa Gov PH Population and Housing Node 167965VNo ratings yet
- DOH 8-Point Action Agenda - The Medium-Term Strategy of The Health Sector For 2023-2028Document21 pagesDOH 8-Point Action Agenda - The Medium-Term Strategy of The Health Sector For 2023-2028ithran khoNo ratings yet
- 01.a.demographic Projections - Aslam MahmoodDocument51 pages01.a.demographic Projections - Aslam MahmoodMaulikJoshiNo ratings yet
- Moderators:-: Dr. Samreen Dr. Nikhat Dr. Abdullah Dr. Naveen Dr. SaleemDocument14 pagesModerators:-: Dr. Samreen Dr. Nikhat Dr. Abdullah Dr. Naveen Dr. SaleemorthooNo ratings yet
- Non - Communicable DiseaseDocument12 pagesNon - Communicable DiseaseFaruk AdemNo ratings yet
- Population and Its Control KailashDocument69 pagesPopulation and Its Control KailashKailash NagarNo ratings yet
- Determinants of Enrollment Decision in The Community-Based Health Insurance, North West Ethiopia: A Case-Control StudyDocument9 pagesDeterminants of Enrollment Decision in The Community-Based Health Insurance, North West Ethiopia: A Case-Control StudySabir ImamNo ratings yet
- SSM - Population Health: ArticleDocument9 pagesSSM - Population Health: ArticledwiNo ratings yet
- Population and Its Control by Kailash NagarDocument69 pagesPopulation and Its Control by Kailash NagarKailash NagarNo ratings yet
- David E. BloomDocument32 pagesDavid E. Bloomrnjn mhta.No ratings yet
- David E. BloomDocument32 pagesDavid E. Bloomrnjn mhta.No ratings yet
- Innovative Ways To Meet Health Challenges of Urban India - Radhika Arora - Sourav Neogi - Madhavi MisraDocument9 pagesInnovative Ways To Meet Health Challenges of Urban India - Radhika Arora - Sourav Neogi - Madhavi MisraJimmy KatiraNo ratings yet
- WHO HIS HSR 17.5 EngDocument12 pagesWHO HIS HSR 17.5 EngRaresNo ratings yet
- Review and Appraisal of Research Evidences Generated To Harness The Demographic Dividend in EthiopiaDocument16 pagesReview and Appraisal of Research Evidences Generated To Harness The Demographic Dividend in EthiopiaCentral Asian StudiesNo ratings yet
- National Health PolicyDocument58 pagesNational Health PolicyHarsha DeepakNo ratings yet
- Health Care Status in IndiaDocument46 pagesHealth Care Status in Indialucky prajapatiNo ratings yet
- Social Health Protection Toward UHC in Lao PDRDocument16 pagesSocial Health Protection Toward UHC in Lao PDRADBI EventsNo ratings yet
- After The Dividend: Caring For A Greying IndiaDocument5 pagesAfter The Dividend: Caring For A Greying IndiaAmit KumarNo ratings yet
- Socioeconomic Inequalities and Mortality Trends in BRICS, 1990-2010Document8 pagesSocioeconomic Inequalities and Mortality Trends in BRICS, 1990-2010Anonymous 6OPLC9UNo ratings yet
- Aquino Health AgendaDocument41 pagesAquino Health AgendaJannine Mae Zaragosa MosquisaNo ratings yet
- Research Article Willingness To Pay For Social Health Insurance and Associated Factors Among Health Care Providers in Addis Ababa, EthiopiaDocument7 pagesResearch Article Willingness To Pay For Social Health Insurance and Associated Factors Among Health Care Providers in Addis Ababa, EthiopiaaisyahNo ratings yet
- 2017Document107 pages2017GEGAYNo ratings yet
- National Health Accounts of The Republic of Botswana: 2000-2002Document35 pagesNational Health Accounts of The Republic of Botswana: 2000-2002iisteNo ratings yet
- Universal Health Coverage in China: A Health Economic PerspectiveFrom EverandUniversal Health Coverage in China: A Health Economic PerspectiveNo ratings yet
- Country Diagnostic Study on Long-Term Care in MongoliaFrom EverandCountry Diagnostic Study on Long-Term Care in MongoliaNo ratings yet
- Doing the Right Thing: 'New' Building Zimbabwe's Health System: 'New' Building Zimbabwe's Health System: 'New Building: 'New Building' Zimbabwe's Health SystemFrom EverandDoing the Right Thing: 'New' Building Zimbabwe's Health System: 'New' Building Zimbabwe's Health System: 'New Building: 'New Building' Zimbabwe's Health SystemNo ratings yet
- Daftar Aegency SingapuraDocument12 pagesDaftar Aegency SingapuraikrokNo ratings yet
- CHN-Interprofessional Care and Records.2022Document39 pagesCHN-Interprofessional Care and Records.2022Alfred Bueno DanganiNo ratings yet
- Ao2023-0020 Implementing Rules and Regulations of Republic Act No. 11959Document8 pagesAo2023-0020 Implementing Rules and Regulations of Republic Act No. 11959Learsi AfableNo ratings yet
- NHS FPX 6004 Assessment 2 Policy ProposalDocument5 pagesNHS FPX 6004 Assessment 2 Policy ProposalEmma WatsonNo ratings yet
- Pca-Choosing An Organization WorksheetDocument3 pagesPca-Choosing An Organization Worksheetapi-591182235No ratings yet
- Anthem Anthem Gold Hmo 35 4huvDocument11 pagesAnthem Anthem Gold Hmo 35 4huvLn TranNo ratings yet
- STEGH Annual Report 2013 - FA LRDocument2 pagesSTEGH Annual Report 2013 - FA LRJigga mannNo ratings yet
- Good Helth ServicesDocument19 pagesGood Helth ServicesDini UtamiNo ratings yet
- Star Health Assure - One Pager - Version 1.0 - April - 2022Document2 pagesStar Health Assure - One Pager - Version 1.0 - April - 2022Rohit kanyalNo ratings yet
- IPC-questionnaire-masteral EditedDocument4 pagesIPC-questionnaire-masteral EditedWinnie Lorraine Umali-PascualNo ratings yet
- USCE Database Compiled by Usmlesarthi TeamDocument15 pagesUSCE Database Compiled by Usmlesarthi Teamurwaafghan48No ratings yet
- AOC C - InputDocument34 pagesAOC C - InputZothankhumaNo ratings yet
- NURS FPX 6614 Assessment 3 Disseminating The Evidence Scholarly Video Media SubmissionDocument7 pagesNURS FPX 6614 Assessment 3 Disseminating The Evidence Scholarly Video Media SubmissionEmma WatsonNo ratings yet
- D 0131-HipotermiaDocument2 pagesD 0131-HipotermiaKamelNo ratings yet
- Topic 5 (End of Life Care Part 1)Document41 pagesTopic 5 (End of Life Care Part 1)BSN2G- SABLA-ON LORRAINE ANNENo ratings yet
- 2021 CPT CodesDocument8 pages2021 CPT CodesSundar RamanathanNo ratings yet
- Essay On "Why I Am Interested in Medicine and How I Will Use It To Provide Good Health Care For The People of Indonesia in The Future"Document3 pagesEssay On "Why I Am Interested in Medicine and How I Will Use It To Provide Good Health Care For The People of Indonesia in The Future"Ananda Cahya monalisaNo ratings yet
- Fair Work Information StatementDocument2 pagesFair Work Information StatementaNo ratings yet
- Informatics and Nursing Sensitive Quality Indicators: Name Institution Date CourseDocument5 pagesInformatics and Nursing Sensitive Quality Indicators: Name Institution Date CourseKevin SangNo ratings yet
- NURS FPX 6416 Assessment 3 Needs Assessment Meeting With StakeholdersDocument5 pagesNURS FPX 6416 Assessment 3 Needs Assessment Meeting With StakeholdersCarolyn HarkerNo ratings yet
- Hemalatha P 19-Dec-2024 WM Global Technology Services PVT Ltd-1 MEMBER4680Document3 pagesHemalatha P 19-Dec-2024 WM Global Technology Services PVT Ltd-1 MEMBER4680hemaaa899No ratings yet
- Unit Plane Unit 2 FonDocument11 pagesUnit Plane Unit 2 Fonthakurmanu6386No ratings yet
- Dentists Email ListDocument8 pagesDentists Email Listlawra nickNo ratings yet
- Cvicu Nurse ResumeDocument7 pagesCvicu Nurse Resumek1kywukigog2100% (2)
- Final - Final Maginhawang Baga Apsr - de LeonDocument12 pagesFinal - Final Maginhawang Baga Apsr - de LeonMaria Lowella de leonNo ratings yet
- Disability PDFDocument3 pagesDisability PDFgeri delaneyNo ratings yet
- ChatPDF-MGH's PATADocument4 pagesChatPDF-MGH's PATAFelipe GonzalezNo ratings yet
- Johns Hopkins Medicine Strategic Plan: Tool Kit For ManagersDocument15 pagesJohns Hopkins Medicine Strategic Plan: Tool Kit For ManagerssaritaNo ratings yet
- Contract Labour Compliance ChecklistDocument9 pagesContract Labour Compliance ChecklistGaurav2192No ratings yet
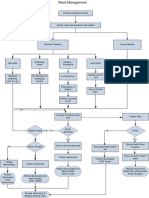
- Ward ManagementDocument1 pageWard Managementaman kumar jhaNo ratings yet























































































Download as pdf or txt
You might also like
- Module 1 CHN 1Document15 pagesModule 1 CHN 1Danz KieNo ratings yet
- Family Welfare ProgrammeDocument19 pagesFamily Welfare ProgrammeMahesh Sahu100% (2)
- Primary Health Care Systems (Primasys) : Case Study From MexicoDocument16 pagesPrimary Health Care Systems (Primasys) : Case Study From MexicoEpi SidaNo ratings yet
- Primary Health Care Systems (Primasys) : Case Study From EthiopiaDocument12 pagesPrimary Health Care Systems (Primasys) : Case Study From EthiopiaMuluken TesfayeNo ratings yet
- Population PolicyDocument6 pagesPopulation PolicyIqra YameenNo ratings yet
- WHO HIS HSR 17.15 Eng PDFDocument12 pagesWHO HIS HSR 17.15 Eng PDFNebyuNo ratings yet
- Ing The Burden 2020-2015 16Document8 pagesIng The Burden 2020-2015 16EstreLLA ValenciaNo ratings yet
- dm2022 0082Document9 pagesdm2022 0082Harold Paulo MejiaNo ratings yet
- Gha 6 19650Document10 pagesGha 6 19650Betric HanNo ratings yet
- Universal Health Care Coverage Through Pluralistic Approaches: Experience From ThailandDocument27 pagesUniversal Health Care Coverage Through Pluralistic Approaches: Experience From ThailandThaworn SakunphanitNo ratings yet
- Philippine Pharmaceutical IndustryDocument103 pagesPhilippine Pharmaceutical IndustryVijay Kumar MunshiNo ratings yet
- ACS-Country-Report Tanzania PDFDocument31 pagesACS-Country-Report Tanzania PDFCapacita DesignNo ratings yet
- Cause Specific Mortality and Socioeconomic Status in Chakaria BangladeshDocument10 pagesCause Specific Mortality and Socioeconomic Status in Chakaria BangladeshSabujNo ratings yet
- DM No. 2022-0511 Reporting of ZOD - 03oct2022Document9 pagesDM No. 2022-0511 Reporting of ZOD - 03oct2022Catherine LargaNo ratings yet
- POPDEV (Basic Concepts)Document64 pagesPOPDEV (Basic Concepts)Paul Keene BonitaNo ratings yet
- FundingModel TBAndHIVConceptNote Final Ethiopia Oct15 2014Document94 pagesFundingModel TBAndHIVConceptNote Final Ethiopia Oct15 2014tokumaNo ratings yet
- LASI India Executive SummaryDocument52 pagesLASI India Executive SummaryNaudibya MajhiNo ratings yet
- Unfpa - Icomp Regional Consultation Family Planning in Asia and The Pacific Addressing The ChallengesDocument23 pagesUnfpa - Icomp Regional Consultation Family Planning in Asia and The Pacific Addressing The ChallengesYantoNo ratings yet
- FCHVDocument22 pagesFCHVSamzana ShresthaNo ratings yet
- Incentives and Disincentives: Necessary, Effective, Just?Document9 pagesIncentives and Disincentives: Necessary, Effective, Just?suman guptaNo ratings yet
- 077C10A61423Document14 pages077C10A61423Endy SitumbekoNo ratings yet
- DemographyDocument28 pagesDemographyAsad ullahNo ratings yet
- Document From Elle Final2Document18 pagesDocument From Elle Final2georgeNo ratings yet
- What Went Wrong With The Achievement of Replacement Fertility in Bangladesh and Its Consequences On The Demographic Dividend The Role of Proximate DeterminantsDocument24 pagesWhat Went Wrong With The Achievement of Replacement Fertility in Bangladesh and Its Consequences On The Demographic Dividend The Role of Proximate DeterminantsRussell KabirNo ratings yet
- Investing in Health: The Role of LGU Officials in Health Sector DevelopmentDocument58 pagesInvesting in Health: The Role of LGU Officials in Health Sector DevelopmentMaan Pastor MananzanNo ratings yet
- Vital Health StatisticsDocument71 pagesVital Health Statisticsritikaritika93% (14)
- Indonesia Packet Population PDFDocument65 pagesIndonesia Packet Population PDFMargareta Laura PattipeilohyNo ratings yet
- Population, Labour Force and EmploymentDocument11 pagesPopulation, Labour Force and EmploymentAsad RazaNo ratings yet
- Healthand Family Welfarestatisticsin India 201920Document253 pagesHealthand Family Welfarestatisticsin India 201920poonam valviNo ratings yet
- Fertility Trends in Bangladesh 2014Document13 pagesFertility Trends in Bangladesh 2014Rozen Tareque HasanNo ratings yet
- Asia-Pacific's Opportunity:: Investing To Avert An HIV/AIDS CrisisDocument20 pagesAsia-Pacific's Opportunity:: Investing To Avert An HIV/AIDS CrisismastahhhNo ratings yet
- 8-Point Action Agenda - The Medium-Term Strategy of The Health Sector For 2023-2028Document19 pages8-Point Action Agenda - The Medium-Term Strategy of The Health Sector For 2023-2028RURAL HEALTH CENTER TAMBLER BAWINGNo ratings yet
- WHO EURO 2020 1710 41461 56527 EngDocument15 pagesWHO EURO 2020 1710 41461 56527 EngBuffaloNo ratings yet
- Psa Gov PH Population and Housing Node 167965Document4 pagesPsa Gov PH Population and Housing Node 167965VNo ratings yet
- DOH 8-Point Action Agenda - The Medium-Term Strategy of The Health Sector For 2023-2028Document21 pagesDOH 8-Point Action Agenda - The Medium-Term Strategy of The Health Sector For 2023-2028ithran khoNo ratings yet
- 01.a.demographic Projections - Aslam MahmoodDocument51 pages01.a.demographic Projections - Aslam MahmoodMaulikJoshiNo ratings yet
- Moderators:-: Dr. Samreen Dr. Nikhat Dr. Abdullah Dr. Naveen Dr. SaleemDocument14 pagesModerators:-: Dr. Samreen Dr. Nikhat Dr. Abdullah Dr. Naveen Dr. SaleemorthooNo ratings yet
- Non - Communicable DiseaseDocument12 pagesNon - Communicable DiseaseFaruk AdemNo ratings yet
- Population and Its Control KailashDocument69 pagesPopulation and Its Control KailashKailash NagarNo ratings yet
- Determinants of Enrollment Decision in The Community-Based Health Insurance, North West Ethiopia: A Case-Control StudyDocument9 pagesDeterminants of Enrollment Decision in The Community-Based Health Insurance, North West Ethiopia: A Case-Control StudySabir ImamNo ratings yet
- SSM - Population Health: ArticleDocument9 pagesSSM - Population Health: ArticledwiNo ratings yet
- Population and Its Control by Kailash NagarDocument69 pagesPopulation and Its Control by Kailash NagarKailash NagarNo ratings yet
- David E. BloomDocument32 pagesDavid E. Bloomrnjn mhta.No ratings yet
- David E. BloomDocument32 pagesDavid E. Bloomrnjn mhta.No ratings yet
- Innovative Ways To Meet Health Challenges of Urban India - Radhika Arora - Sourav Neogi - Madhavi MisraDocument9 pagesInnovative Ways To Meet Health Challenges of Urban India - Radhika Arora - Sourav Neogi - Madhavi MisraJimmy KatiraNo ratings yet
- WHO HIS HSR 17.5 EngDocument12 pagesWHO HIS HSR 17.5 EngRaresNo ratings yet
- Review and Appraisal of Research Evidences Generated To Harness The Demographic Dividend in EthiopiaDocument16 pagesReview and Appraisal of Research Evidences Generated To Harness The Demographic Dividend in EthiopiaCentral Asian StudiesNo ratings yet
- National Health PolicyDocument58 pagesNational Health PolicyHarsha DeepakNo ratings yet
- Health Care Status in IndiaDocument46 pagesHealth Care Status in Indialucky prajapatiNo ratings yet
- Social Health Protection Toward UHC in Lao PDRDocument16 pagesSocial Health Protection Toward UHC in Lao PDRADBI EventsNo ratings yet
- After The Dividend: Caring For A Greying IndiaDocument5 pagesAfter The Dividend: Caring For A Greying IndiaAmit KumarNo ratings yet
- Socioeconomic Inequalities and Mortality Trends in BRICS, 1990-2010Document8 pagesSocioeconomic Inequalities and Mortality Trends in BRICS, 1990-2010Anonymous 6OPLC9UNo ratings yet
- Aquino Health AgendaDocument41 pagesAquino Health AgendaJannine Mae Zaragosa MosquisaNo ratings yet
- Research Article Willingness To Pay For Social Health Insurance and Associated Factors Among Health Care Providers in Addis Ababa, EthiopiaDocument7 pagesResearch Article Willingness To Pay For Social Health Insurance and Associated Factors Among Health Care Providers in Addis Ababa, EthiopiaaisyahNo ratings yet
- 2017Document107 pages2017GEGAYNo ratings yet
- National Health Accounts of The Republic of Botswana: 2000-2002Document35 pagesNational Health Accounts of The Republic of Botswana: 2000-2002iisteNo ratings yet
- Universal Health Coverage in China: A Health Economic PerspectiveFrom EverandUniversal Health Coverage in China: A Health Economic PerspectiveNo ratings yet
- Country Diagnostic Study on Long-Term Care in MongoliaFrom EverandCountry Diagnostic Study on Long-Term Care in MongoliaNo ratings yet
- Doing the Right Thing: 'New' Building Zimbabwe's Health System: 'New' Building Zimbabwe's Health System: 'New Building: 'New Building' Zimbabwe's Health SystemFrom EverandDoing the Right Thing: 'New' Building Zimbabwe's Health System: 'New' Building Zimbabwe's Health System: 'New Building: 'New Building' Zimbabwe's Health SystemNo ratings yet
- Daftar Aegency SingapuraDocument12 pagesDaftar Aegency SingapuraikrokNo ratings yet
- CHN-Interprofessional Care and Records.2022Document39 pagesCHN-Interprofessional Care and Records.2022Alfred Bueno DanganiNo ratings yet
- Ao2023-0020 Implementing Rules and Regulations of Republic Act No. 11959Document8 pagesAo2023-0020 Implementing Rules and Regulations of Republic Act No. 11959Learsi AfableNo ratings yet
- NHS FPX 6004 Assessment 2 Policy ProposalDocument5 pagesNHS FPX 6004 Assessment 2 Policy ProposalEmma WatsonNo ratings yet
- Pca-Choosing An Organization WorksheetDocument3 pagesPca-Choosing An Organization Worksheetapi-591182235No ratings yet
- Anthem Anthem Gold Hmo 35 4huvDocument11 pagesAnthem Anthem Gold Hmo 35 4huvLn TranNo ratings yet
- STEGH Annual Report 2013 - FA LRDocument2 pagesSTEGH Annual Report 2013 - FA LRJigga mannNo ratings yet
- Good Helth ServicesDocument19 pagesGood Helth ServicesDini UtamiNo ratings yet
- Star Health Assure - One Pager - Version 1.0 - April - 2022Document2 pagesStar Health Assure - One Pager - Version 1.0 - April - 2022Rohit kanyalNo ratings yet
- IPC-questionnaire-masteral EditedDocument4 pagesIPC-questionnaire-masteral EditedWinnie Lorraine Umali-PascualNo ratings yet
- USCE Database Compiled by Usmlesarthi TeamDocument15 pagesUSCE Database Compiled by Usmlesarthi Teamurwaafghan48No ratings yet
- AOC C - InputDocument34 pagesAOC C - InputZothankhumaNo ratings yet
- NURS FPX 6614 Assessment 3 Disseminating The Evidence Scholarly Video Media SubmissionDocument7 pagesNURS FPX 6614 Assessment 3 Disseminating The Evidence Scholarly Video Media SubmissionEmma WatsonNo ratings yet
- D 0131-HipotermiaDocument2 pagesD 0131-HipotermiaKamelNo ratings yet
- Topic 5 (End of Life Care Part 1)Document41 pagesTopic 5 (End of Life Care Part 1)BSN2G- SABLA-ON LORRAINE ANNENo ratings yet
- 2021 CPT CodesDocument8 pages2021 CPT CodesSundar RamanathanNo ratings yet
- Essay On "Why I Am Interested in Medicine and How I Will Use It To Provide Good Health Care For The People of Indonesia in The Future"Document3 pagesEssay On "Why I Am Interested in Medicine and How I Will Use It To Provide Good Health Care For The People of Indonesia in The Future"Ananda Cahya monalisaNo ratings yet
- Fair Work Information StatementDocument2 pagesFair Work Information StatementaNo ratings yet
- Informatics and Nursing Sensitive Quality Indicators: Name Institution Date CourseDocument5 pagesInformatics and Nursing Sensitive Quality Indicators: Name Institution Date CourseKevin SangNo ratings yet
- NURS FPX 6416 Assessment 3 Needs Assessment Meeting With StakeholdersDocument5 pagesNURS FPX 6416 Assessment 3 Needs Assessment Meeting With StakeholdersCarolyn HarkerNo ratings yet
- Hemalatha P 19-Dec-2024 WM Global Technology Services PVT Ltd-1 MEMBER4680Document3 pagesHemalatha P 19-Dec-2024 WM Global Technology Services PVT Ltd-1 MEMBER4680hemaaa899No ratings yet
- Unit Plane Unit 2 FonDocument11 pagesUnit Plane Unit 2 Fonthakurmanu6386No ratings yet
- Dentists Email ListDocument8 pagesDentists Email Listlawra nickNo ratings yet
- Cvicu Nurse ResumeDocument7 pagesCvicu Nurse Resumek1kywukigog2100% (2)
- Final - Final Maginhawang Baga Apsr - de LeonDocument12 pagesFinal - Final Maginhawang Baga Apsr - de LeonMaria Lowella de leonNo ratings yet
- Disability PDFDocument3 pagesDisability PDFgeri delaneyNo ratings yet
- ChatPDF-MGH's PATADocument4 pagesChatPDF-MGH's PATAFelipe GonzalezNo ratings yet
- Johns Hopkins Medicine Strategic Plan: Tool Kit For ManagersDocument15 pagesJohns Hopkins Medicine Strategic Plan: Tool Kit For ManagerssaritaNo ratings yet
- Contract Labour Compliance ChecklistDocument9 pagesContract Labour Compliance ChecklistGaurav2192No ratings yet
- Ward ManagementDocument1 pageWard Managementaman kumar jhaNo ratings yet