Download as docx, pdf, or txt
You might also like
- Concept Map TBIDocument2 pagesConcept Map TBIraquel maniego67% (3)
- Diabetic Ketoacidosis: Dr. Kaustuv de Fellow (3 Yr.) Critical Care MedicineDocument31 pagesDiabetic Ketoacidosis: Dr. Kaustuv de Fellow (3 Yr.) Critical Care MedicineKaustuv DeNo ratings yet
- Diabetic KetoacidosisDocument2 pagesDiabetic KetoacidosisFrancis ChegeNo ratings yet
- MetabolicDocument23 pagesMetabolicbtidipNo ratings yet
- Diabetic KetoacidosisDocument16 pagesDiabetic Ketoacidosisjoyshe111100% (3)
- ST - WaterDocument7 pagesST - WaterlalitrajindoliaNo ratings yet
- Hyperglycemic Emergencies 2101Document47 pagesHyperglycemic Emergencies 2101IndahfitriaaNo ratings yet
- 1 DiurethicsDocument8 pages1 DiurethicsMoataz TrabehNo ratings yet
- KetoacidosisDocument1 pageKetoacidosisLee June LyngNo ratings yet
- Metabolic AlkalosisDocument15 pagesMetabolic AlkalosisMenna ElesawyNo ratings yet
- Common ElectrolyteDocument48 pagesCommon ElectrolytemekuriawNo ratings yet
- Diabetic Ketoacidosi S: Prepared byDocument28 pagesDiabetic Ketoacidosi S: Prepared byفيصل الاعرجNo ratings yet
- Fluid and Electrolyte Therapy in Diabetic KetoacidosisDocument13 pagesFluid and Electrolyte Therapy in Diabetic KetoacidosisLohJNo ratings yet
- Acid Base Balance and DisordersDocument25 pagesAcid Base Balance and DisordersIsmail Vokshi100% (1)
- Metabolic AlkalosisDocument8 pagesMetabolic AlkalosisPauline PerezNo ratings yet
- Fluid and Electrolyte ImbalanceDocument47 pagesFluid and Electrolyte Imbalanceanne claire feudoNo ratings yet
- Endocrine Emergencies in Dogs and CatsDocument29 pagesEndocrine Emergencies in Dogs and CatsSteffi AraujoNo ratings yet
- Quick Facts For Electrolyte AnalysisDocument3 pagesQuick Facts For Electrolyte AnalysiscrystalsheNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CKDocument15 pagesDr. Ali's Uworld Notes For Step 2 CKBoogy WoogyNo ratings yet
- Hyperkalemia: Samir El AnsaryDocument43 pagesHyperkalemia: Samir El AnsaryStrept PneumoniaNo ratings yet
- Acute DM ComplicationsDocument34 pagesAcute DM ComplicationsHillary RabinNo ratings yet
- Acute Complications of Diabetes Mellitus: DR Yemane G (MD, Assis. Prof. EMCC)Document63 pagesAcute Complications of Diabetes Mellitus: DR Yemane G (MD, Assis. Prof. EMCC)yared getachewNo ratings yet
- L7 Digestive Disorders NonruminantDocument3 pagesL7 Digestive Disorders NonruminantMayank MeenaNo ratings yet
- Blood Levels of Cholesterol Are Decreased in Hyperthyroidism and Increased in HypothyroidismDocument6 pagesBlood Levels of Cholesterol Are Decreased in Hyperthyroidism and Increased in HypothyroidismSimina ÎntunericNo ratings yet
- POTASSIUM HOMEOSTASIS كيمياء سريريةDocument4 pagesPOTASSIUM HOMEOSTASIS كيمياء سريريةMustafa Salah MahdiNo ratings yet
- Diabetic KetoacidosisDocument14 pagesDiabetic KetoacidosisYash Ramawat100% (1)
- NSG IV Test 3Document4 pagesNSG IV Test 3Maria Phebe SinsayNo ratings yet
- c15 Diuretic AgentsDocument13 pagesc15 Diuretic AgentsmohammadNo ratings yet
- Lecture+24 +25+diureticsDocument69 pagesLecture+24 +25+diureticsGhina RizwanNo ratings yet
- Fluid and Electrolyte Imbalances Part 2Document47 pagesFluid and Electrolyte Imbalances Part 2Abinaya RanganathanNo ratings yet
- E.Nasr M.D Professor of Medecine Nephrology Division ST George Hospital University of BalamandDocument51 pagesE.Nasr M.D Professor of Medecine Nephrology Division ST George Hospital University of Balamandsami crowNo ratings yet
- Metabolic Acid - Base ImbalancesDocument5 pagesMetabolic Acid - Base Imbalancesmardsz100% (1)
- Acute-Renal-Failure Lecture OnlyDocument17 pagesAcute-Renal-Failure Lecture OnlyeyesontheskyNo ratings yet
- Critical Care Management For Patient With Diabetic Ketoacidosis (Dka) NCM 118 LectureDocument12 pagesCritical Care Management For Patient With Diabetic Ketoacidosis (Dka) NCM 118 LectureBULONG Darlyn GraceNo ratings yet
- Hormones 23Document14 pagesHormones 23sumayaalammimNo ratings yet
- Dangerous Rhythms Tachycardia: Potassium Electrolyte HypokalemiaDocument7 pagesDangerous Rhythms Tachycardia: Potassium Electrolyte HypokalemiagorodoeNo ratings yet
- Acute Kidney InjuryDocument21 pagesAcute Kidney InjuryLALITH SAI KNo ratings yet
- Metabolic AlkalosisDocument9 pagesMetabolic AlkalosisMohammad Zaki BudimanNo ratings yet
- HYPOKALEMIADocument41 pagesHYPOKALEMIAsamudraandiNo ratings yet
- Electrolyte and Metabolic Disturbances Electrolyte and Metabolic DisturbancesDocument58 pagesElectrolyte and Metabolic Disturbances Electrolyte and Metabolic DisturbancesAbdulrahman Mahmoud GhaziNo ratings yet
- ReferatDocument53 pagesReferatHendri SaputraNo ratings yet
- Disturbances of Acid-Base BalanceDocument3 pagesDisturbances of Acid-Base BalanceDr. NateqNo ratings yet
- Physiology 1 Fluid ElectrolyteDocument38 pagesPhysiology 1 Fluid ElectrolyteHaziq KamardinNo ratings yet
- SodiumDocument48 pagesSodiumSanchita SahaNo ratings yet
- Mabes Fluid and Electrolyte ImbalancesDocument15 pagesMabes Fluid and Electrolyte ImbalancesMabesNo ratings yet
- Physio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionDocument5 pagesPhysio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionAnny AlvrzNo ratings yet
- SodiumDocument5 pagesSodiumTepperoniNo ratings yet
- Lecture 10.2-Laboratory Aspect of Electrolyte and Acid Based, DR Ira Puspitawati, SP - PK (2021)Document76 pagesLecture 10.2-Laboratory Aspect of Electrolyte and Acid Based, DR Ira Puspitawati, SP - PK (2021)NOVITA NUR ROHMA ROHMANo ratings yet
- Potassium Disorders: Syeda Shaheera ZaidiDocument60 pagesPotassium Disorders: Syeda Shaheera ZaidiMohammad AliNo ratings yet
- Hdp301f&e Imbalancesf2020Document6 pagesHdp301f&e Imbalancesf2020Linda NguyenNo ratings yet
- Hipocalemia e Hipercalemia. 2015 PDFDocument17 pagesHipocalemia e Hipercalemia. 2015 PDFMiguel Angel Manotas CañasNo ratings yet
- UWorld Cards July 14Document7 pagesUWorld Cards July 14smian08No ratings yet
- AlkalosisDocument2 pagesAlkalosisrosemoses305No ratings yet
- Hyperkalemia: Samir El AnsaryDocument45 pagesHyperkalemia: Samir El Ansarymariatul fithriasariNo ratings yet
- Water and Electrolyte Balance - 240629 - 132135Document26 pagesWater and Electrolyte Balance - 240629 - 132135AyeshaNo ratings yet
- Ascites, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandAscites, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Hepatic Encephalopathy: Causes, Tests, and Treatment OptionsFrom EverandHepatic Encephalopathy: Causes, Tests, and Treatment OptionsRating: 3.5 out of 5 stars3.5/5 (2)
- Fluid and Electrolytes for Nursing StudentsFrom EverandFluid and Electrolytes for Nursing StudentsRating: 5 out of 5 stars5/5 (12)
- Equine Fluid TherapyFrom EverandEquine Fluid TherapyC. Langdon FieldingNo ratings yet
- Physiol 93 B3Document1 pagePhysiol 93 B3DonkeyManNo ratings yet
- CEACCP - KetamineDocument5 pagesCEACCP - KetamineDonkeyManNo ratings yet
- CEACCP - Latex AllergyDocument4 pagesCEACCP - Latex AllergyDonkeyManNo ratings yet
- CEACCP - Illegal Substances in Anaesthetic and Intensive Care PracticesDocument5 pagesCEACCP - Illegal Substances in Anaesthetic and Intensive Care PracticesDonkeyManNo ratings yet
- Pharmacodynamics, Drug Action Targets, PharmacogeneticsDocument21 pagesPharmacodynamics, Drug Action Targets, PharmacogeneticsDonkeyManNo ratings yet
- Cellular Physiology SAQsDocument1 pageCellular Physiology SAQsDonkeyManNo ratings yet
- Define The Mechanisms of Action and Adverse Effects of Metoprolol, GTN, and Diltiazem When Used To Manage MIDocument2 pagesDefine The Mechanisms of Action and Adverse Effects of Metoprolol, GTN, and Diltiazem When Used To Manage MIDonkeyManNo ratings yet
- Pharm 02 A11Document4 pagesPharm 02 A11DonkeyManNo ratings yet
- CEACCP - Intrathecal Opioids in The Management of Acute Postoperative PainDocument5 pagesCEACCP - Intrathecal Opioids in The Management of Acute Postoperative PainDonkeyManNo ratings yet
- Pharm 00 B15Document2 pagesPharm 00 B15DonkeyManNo ratings yet
- Pharm 00 A9Document2 pagesPharm 00 A9DonkeyManNo ratings yet
- Pharm 02 A10Document2 pagesPharm 02 A10DonkeyManNo ratings yet
- Pharm 00 A15Document2 pagesPharm 00 A15DonkeyManNo ratings yet
- Compare and Contrast Neostigmine and The Organophosphate CompoundsDocument1 pageCompare and Contrast Neostigmine and The Organophosphate CompoundsDonkeyManNo ratings yet
- Pharm 00 B11Document1 pagePharm 00 B11DonkeyManNo ratings yet
- Pharm 00 B14Document2 pagesPharm 00 B14DonkeyManNo ratings yet
- Pharm 00 A14Document2 pagesPharm 00 A14DonkeyManNo ratings yet
- Compare and Contrast Atropine and Glycopyrulate, and Discuss The Clinical ImplicationsDocument2 pagesCompare and Contrast Atropine and Glycopyrulate, and Discuss The Clinical ImplicationsDonkeyManNo ratings yet
- Compare and Contrast The Pharamcology of Ephedrine and NoradrenalineDocument1 pageCompare and Contrast The Pharamcology of Ephedrine and NoradrenalineDonkeyManNo ratings yet
- Pharm 00 A12Document1 pagePharm 00 A12DonkeyManNo ratings yet
- Compare and Contrast The Pharmacology of Esmolol and PropanololDocument1 pageCompare and Contrast The Pharmacology of Esmolol and PropanololDonkeyManNo ratings yet
- FS Antimicrobial Dosing Obesity AMS Updates Issue4 - Nov2018Document4 pagesFS Antimicrobial Dosing Obesity AMS Updates Issue4 - Nov2018DonkeyManNo ratings yet
- Comparative Pharmacokinetics of Fentanyl and Alfentanil: Br. J. Anaesth. (1982), 54, 871Document7 pagesComparative Pharmacokinetics of Fentanyl and Alfentanil: Br. J. Anaesth. (1982), 54, 871DonkeyManNo ratings yet
- VOLATILEAGENTSDocument4 pagesVOLATILEAGENTSDonkeyManNo ratings yet
- The Physiology of The GIT and The Liver QuestionsDocument44 pagesThe Physiology of The GIT and The Liver QuestionsDonkeyManNo ratings yet
- Palliative Care HandbookDocument82 pagesPalliative Care HandbookDonkeyManNo ratings yet
- Base Excess (Be) Measure of Metabolic Acid-Base Status: Dr. David LynessDocument1 pageBase Excess (Be) Measure of Metabolic Acid-Base Status: Dr. David LynessDonkeyManNo ratings yet
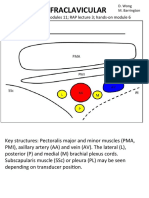
- Infraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6Document4 pagesInfraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6DonkeyManNo ratings yet
- Cholinergic Agents: Cholinergic Receptors Types of Receptor Muscarinic Receptor Nicotinic ReceptorDocument4 pagesCholinergic Agents: Cholinergic Receptors Types of Receptor Muscarinic Receptor Nicotinic ReceptorDonkeyManNo ratings yet
- Chapter-1 Structural OrissuesDocument18 pagesChapter-1 Structural OrissuesRama DeviNo ratings yet
- Learning Objectives: Interactive LinkDocument2 pagesLearning Objectives: Interactive LinkGhh TyuNo ratings yet
- Abdominal X RayDocument45 pagesAbdominal X RayAbdullah As'adNo ratings yet
- Nursing Manikins As Per IncDocument54 pagesNursing Manikins As Per IncRahul KashyapNo ratings yet
- 2nd Quarter Summative Test No.2 ScienceDocument2 pages2nd Quarter Summative Test No.2 ScienceMarilou KimayongNo ratings yet
- 6 Cardiac A&P WorkbookDocument29 pages6 Cardiac A&P WorkbookClayson BuftonNo ratings yet
- Endocrine System (Zoology)Document3 pagesEndocrine System (Zoology)Cheska de GuzmanNo ratings yet
- Urinary EssayDocument5 pagesUrinary EssayMuhamad Saddam Jamaludin SaNo ratings yet
- Assessment Diagnosis Rationale Planning Interventio N Rationale EvaluationDocument2 pagesAssessment Diagnosis Rationale Planning Interventio N Rationale Evaluationbambem aevanNo ratings yet
- Histology LabDocument9 pagesHistology Labsidro123100% (1)
- Istanbul Okan University Faculty of Medicine Student GuideDocument45 pagesIstanbul Okan University Faculty of Medicine Student GuideAyshaNo ratings yet
- Checklist Breast Examination Student's Name: - Section and Group: - ScoreDocument2 pagesChecklist Breast Examination Student's Name: - Section and Group: - ScoreMacen OrtegaNo ratings yet
- Histology Module 1 Review PT 2Document13 pagesHistology Module 1 Review PT 2Neera SaxenaNo ratings yet
- The Major Divisions of The Nervous SystemDocument17 pagesThe Major Divisions of The Nervous SystemLiana BaluyotNo ratings yet
- G-10 Biology, 3.2 Sense OrgansDocument10 pagesG-10 Biology, 3.2 Sense OrgansYohannes NigussieNo ratings yet
- BNYS SyllabusDocument260 pagesBNYS SyllabusBalagovind T PNo ratings yet
- SKIN and BODY MEMBRANESDocument9 pagesSKIN and BODY MEMBRANESNicole EncinaresNo ratings yet
- Chapter 12 - Lymphatic System and Body Defenses ReviewerDocument5 pagesChapter 12 - Lymphatic System and Body Defenses Reviewerkoshiaiko21No ratings yet
- An RNA Vaccine Drives Expansion and Efficacy of claudin-CAR-T Cells Against Solid TumorsDocument9 pagesAn RNA Vaccine Drives Expansion and Efficacy of claudin-CAR-T Cells Against Solid TumorsYusuf DemirNo ratings yet
- Reproductive SystemDocument6 pagesReproductive SystemanojanNo ratings yet
- 0301a AllDocument3 pages0301a AllWiendha LiendriasariNo ratings yet
- Woc ArdsDocument2 pagesWoc Ardssyarifah salmaNo ratings yet
- كتاب اسئلة جميلDocument401 pagesكتاب اسئلة جميلMohammadSAL-Rawashdeh100% (1)
- Immunology Serology in Laboratory Medicine 5th Edition Turgeon Test BankDocument9 pagesImmunology Serology in Laboratory Medicine 5th Edition Turgeon Test BankMarkJoneskjsme100% (15)
- CretinismDocument9 pagesCretinismBrendan chukwunonsoNo ratings yet
- 1-The Eustachian Tube Is Opened by Contraction ofDocument10 pages1-The Eustachian Tube Is Opened by Contraction ofNofouz MaswadaNo ratings yet
- Sistem EkskresiDocument8 pagesSistem EkskresiNatasyaNo ratings yet
- Presentation PathophysiologyDocument11 pagesPresentation PathophysiologyJade DeopidoNo ratings yet
- Reviewer in QUIZ 1 2 AND 3 5Document3 pagesReviewer in QUIZ 1 2 AND 3 5John Eldrin DuyagNo ratings yet